
Abstract
Background:
There are few studies on the locus coeruleus (LC) in frontotemporal lobar degeneration (FTLD) and the potential differences in the LC related to the underlying proteinopathy.
Objective:
The aim of this study was to investigate the LC in FTLD subgroups.
Methods:
Neuropathological cases diagnosed with FTLD were included. The subgroups consisted of FTLD with tau, transactive response DNA-binding protein 43 (TDP) and fused in sarcoma (FUS). Micro- and macroscopical degeneration of the LC were assessed with respect to the number of neurons and the degree of depigmentation. A group of cognitively healthy subjects and a group with vascular cognitive impairment (VCI) served as comparison groups.
Results:
A total of 85 FTLD cases were included, of which 44 had FTLD-TDP, 38 had FTLD-tau, and three had FTLD-FUS. The groups were compared with 25 VCI cases and 41 cognitively healthy control cases (N = 151 for the entire study). All FTLD groups had a statistically higher microscopical degeneration of the LC compared to the controls, but the FTLD-tau group had greater micro- and macroscopical degeneration than the FTLD-TDP group. Age correlated positively with the LC score in the FTLD-tau group, but not in the FTLD-TDP group.
Conclusion:
A greater microscopical degeneration of the LC was observed in all FTLD cases compared to healthy controls and those with VCI. The LC degeneration was more severe in FTLD-tau than in FTLD-TDP. The macroscopically differential degeneration of the LC in FTLD subgroups may facilitate differential diagnostics, potentially with imaging.
INTRODUCTION
Frontotemporal lobar degeneration (FTLD) is a common cause of early-onset dementia, with symptoms arising, on average, during the sixth decade of life [1, 2]. The FTLD diagnosis represents a spectrum of clinical phenotypes of frontotemporal dementia (FTD), encompassing changes in behavior, executive function, language, and motor skill symptoms [3]. Pathologically, FTLD includes three main groups according to protein type pathology: tau, transactive response DNA-binding protein 43 (TDP) and fused in sarcoma (FUS) [4–9]. These groups are further divided into subgroups in entities defined by histopathology and associated genetic variations [6, 8]. Tau and TDP-43 proteinopathies comprise approximately 85–95% of the FTLD pathologies and FTLD-FUS<5% [6, 10–14].
The locus coeruleus (LC) is the main source of norepinephrine in the brain. It is a bilateral nucleus in the pons that plays an important role in cognition, arousal, and attention as well as in the sleep cycle [15]. A disruption of its functions and its cellular integrity has been observed in neurocognitive disorders, such as Alzheimer’s disease (AD) and Lewy body disease (LBD) [16–20]. In AD, hyperphosphorylated tau is accumulated in degenerated neurons of the LC [21]. In LBD, phosphorylated alpha-synuclein is deposited as grains and Lewy bodies in the degenerated LC neurons [22, 23]. In addition to protein deposition, a structural degeneration of the LC neurons presents as a depigmentation and reduction in the number of cells [24–28].
The LC in FTLD has generated less research focus, and there are few reports about potential differences in LC degeneration related to the underlying proteinopathy [24]. A degeneration of the LC is recognized among tau proteinopathies [20, 27–30], while the LC has been reported without proteinopathy burden in cases diagnosed with FTLD-TDP [31–33]. Nevertheless, there are few comparative studies between FTLD tau- and TDP proteinopathies [24]. Several studies have reported greater degeneration of the LC in AD and LBD than in FTLD [26, 34] and vascular cognitive impairment (VCI) [25, 35]. However, in the former two studies, the FTLD group was assessed as one, regardless of protein pathology.
There are thus few comparative studies between FTLD tau- and TDP proteinopathies, primarily the one by Ohm et al. [24]. The study included a large number of individuals, had a comprehensive methodology, and presented data on degeneration severity relative to several clinical variables, of particular interest for pathogenetic considerations.
Differentiating the major pathological groups of FTLD with regard to LC status could be of diagnostic value and could be used in developing modes of treatment [36]. Considering the possibility to observe the LC with clinical MRI, the level of degeneration may be of use in the differential diagnostic workup in cognitively impaired individuals.
The aim of this study was to compare the LC in various FTLD subgroups and with non-neurodegenerative control groups, with the purpose of contributing to improved diagnostics in cognitively impaired individuals.
MATERIALS AND METHODS
Study design
In this study, the LC status was analyzed in various subgroups of FTLD and compared to VCI and a cognitively healthy control group. The comparison was conducted with both microscopic and macroscopic assessment, considering age and the duration of clinical disease in addition to protein type pathology. The assessment did not include comparisons of subtypes within each group of protein pathology due to uneven distribution among subtypes.
The study group was retrieved from consecutive cases having undergone a postmortem neuropathological examination at the Department of Pathology at the University Hospital in Lund, Sweden, in 2001–2020 and diagnosed with any form of FTLD. The procedures of neuropathological examination include extensive whole-brain coronal sectioning and sampling of multiple small regions, as previously presented in detail [37]. Cases in which the LC was not sampled were excluded. Clinical information was retrieved from the medical record system Melior. An approval from the Regional Ethical Review Board at Lund University, now the Swedish Ethical Review Authority, was obtained for this study numbers 944-2017, 00051-2019, and 06582-2019.
Study subjects
The neuropathological diagnoses were set by experienced neuropathologists prior to this study. The FTLD cases included three subgroups: FTLD-TDP, FTLD-tau, and FTLD-FUS. The TDP group included Type A, Type B, Type C, in recent years Type E [38], and FTLD with motor neuron disease or amyotrophic lateral sclerosis [27, 39] as well as cases without specific subtype. The tau group consisted of the subgroups Pick’s disease, corticobasal degeneration, progressive supranuclear palsy, or FTLD-tau without other specific subtype [40].
Control subjects
Two groups were studied for comparison of LC status. One group consisted of cognitively healthy individuals without prior medical history of cognitive impairment and no histopathologic findings of either neurocognitive or vascular-ischemic disorder. Another group of patients were clinically diagnosed with VCI or vascular dementia. Neuropathologically, they displayed clear vascular-ischemic pathology such as lacunar subcortical or scarred cortical infarcts, hypertensive and arteriosclerotic arteriopathy, and ischemic white matter rarefactions [41–45]. The latter cases had no neurodegenerative pathology.
Disease duration
Disease duration was defined as the year of diagnosed cognitive impairment or, when not available, the date of first symptoms described in the medical records until time of death.
Assessment of LC degeneration
Assessment of LC degeneration was conducted microscopically using hematoxylin-eosin-stained sections obtained from the pons at approximately mid-level. The LC was identified by its neuromelanin containing cells lateral to the apex of the fourth ventricle, and the cell count was performed on the best-preserved nucleus of the two sides. A modified scale based on an earlier-described assessment method [25, 26] was used for pathological assessment of the LC. The modified scale included only the cell numbers on the transversal section of the nucleus and an evaluation of the degree of pigmentation, whereas the earlier used assessment of pigment spilling was omitted.
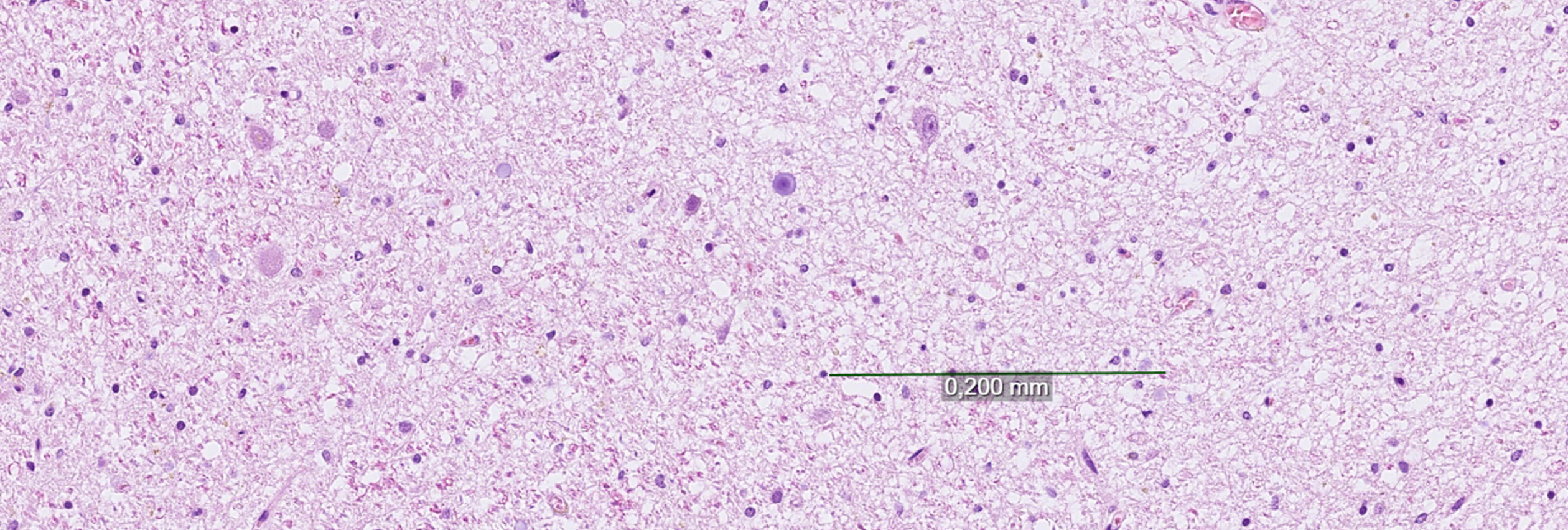
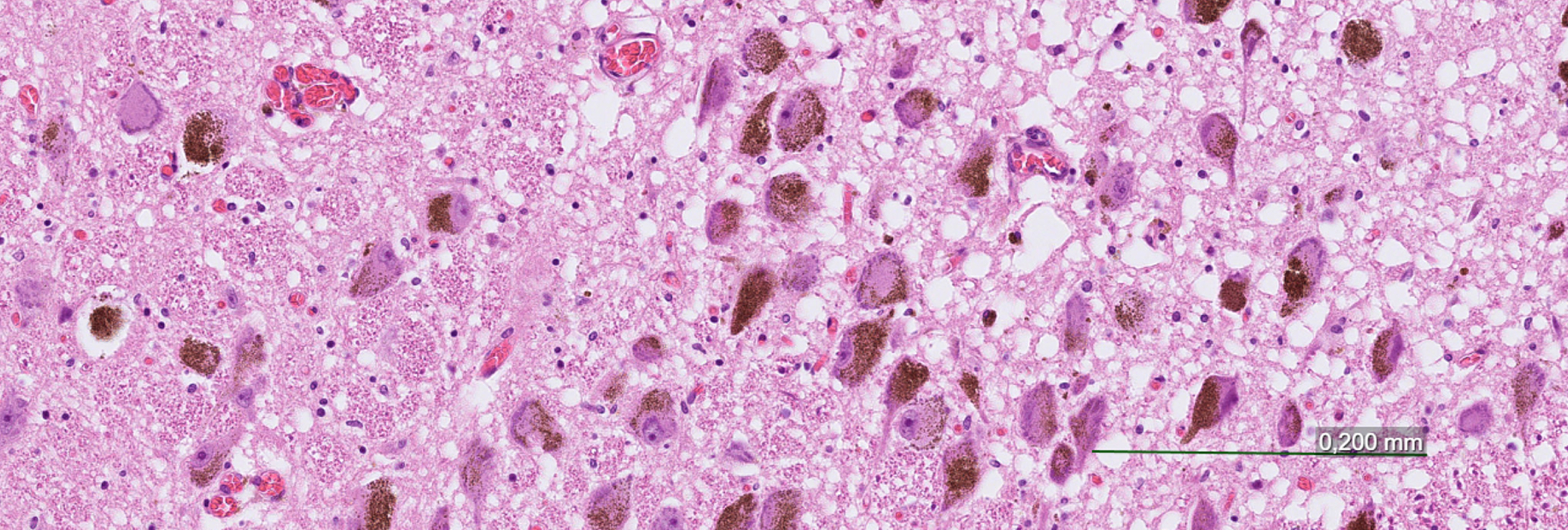
The assessment scale in this study was an inverted scale based on the number of counted pigmented neurons of the best-preserved nucleus. The scale ranged from 0 to 9 points with six intervals (see Table 1): 0–10 counted neurons generated the highest degeneration score of 9 points, 11–20 counted cells generated a score of 8 points, 21–40 counted cells generated 6 points, 41–60 counted cells generated 4 points, 61–80 counted cells generated 2 points, and≥81 counted cells were considered a healthy LC. An additional point was awarded if > 50% of the neurons substantially lacked pigmentation in the cases with a neuron count of 21 or more. Examples from this assessment are demonstrated in Figs. 1and 2 .
Assessment tool of the locus coeruleus based on the number of cells and pigmentation
*An additional point was assigned to the cases which had > 21 cells but > 50% of the cells being depigmented.
Example image of the locus coeruleus (LC) in neuropathological case diagnosed with frontotemporal lobar degeneration (FTLD) with tau proteinopathy at 13x magnification. Demonstrated in the image is a degenerated LC with a degeneration score of 9 points of 9 possible according to assessment tool introduced in the study. Scale bar representing 0.2 mm.
Example image of the locus coeruleus (LC) in neuropathological case diagnosed with frontotemporal lobar degeneration (FTLD) with transactive response DNA-binding protein 43 (TDP) proteinopathy at 13x magnification. Demonstrated in the image is the LC with a degeneration score 2 of 9 points possible according to the assessment tool introduced in the study. Scale bar representing 0.2 mm.
The macroscopic assessment was conducted by neuropathologists during autopsy and subsequent brain examinations and was noted in the pathology report. The nucleus was assigned a score of 2 if the LC was markedly pale and/or reduced in size, a score of 1 if the LC was moderately affected, and a score of 0 for a normal LC that was well-defined and highly pigmented.
Statistical analysis
Statistical analyses were conducted using RStudio 2021.09.1. Differences between groups were assessed using the Kruskal–Wallis test with subsequent pairwise Nemenyi testing. Correlations were assessed using Spearman rank correlation. For all analyses, p values of < 0.05 were considered statistically significant.
RESULTS
A total of 90 cases diagnosed with FTLD were retrieved. Of these, five were excluded due to two or more diagnoses of pathology relating to cognitive disease (mixed dementia). The remaining 85 cases included 44 with FTLD-TDP, 38 with FTLD-tau, and three with FTLD-FUS. In the comparison groups, 25 cases with VCI were included after the exclusion of cases with mixed disease, and 41 cases were included in the cognitively healthy control group. For demographic data, see Table 2.
Demographic data for study subjects according to subgroup
FTLD, frontotemporal lobar dementia; FUS, fused in sarcoma; TDP, transactive response DNA-binding protein 43; VCI, vascular cognitive impairment. aPresented in median years, interquartile range within brackets.
The median LC score in the FTLD-TDP group was 1.5 (interquartile range [IQR] 3) and the corresponding score was 4 (IQR 3) in the FTLD-tau group. Both the control group and the VCI group had median LC scores of 0 (IQR 2), and the FTLD-FUS group (n = 3) had a score of 3, 6, and 7 respectively.
The Kruskal–Wallis test was positive for a significant difference between groups (p < 0.001), and subsequent Nemenyi testing revealed that the FTLD-tau group (mean 3.97, SD 2.87) had higher scores than the FTLD-TDP (mean 1.84, SD 1.78, p = 0.0078), control (mean 0.71, SD 1.13, p < 0.001), and VCI groups (mean 1.18, SD 1.59, p < 0.001). The FTLD-TDP group had higher scores than the control group (p = 0.025) but not significantly different from those of the VCI group (p = 0.52). There was no significant difference between the VCI and control groups (p = 0.79). The FTLD-FUS group (mean 5.33, SD 2.08) was not included in the statistical analysis due to the low number of subjects (n = 3). A graphical representation is presented in Fig. 3.
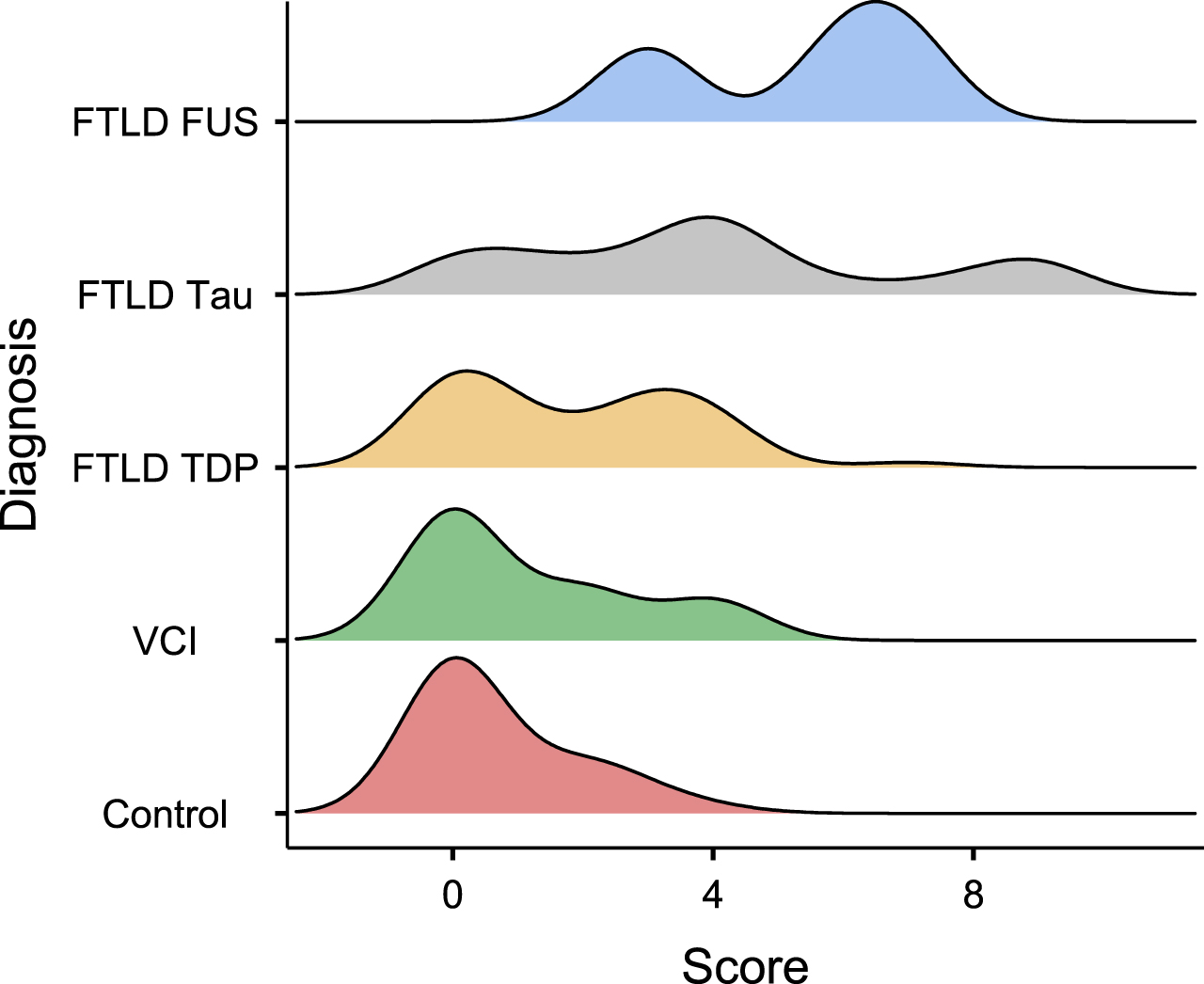
Density plot indicating the distribution of median degeneration score (x-axis) of the locus coeruleus (LC) according to various subgroups (y-axis) of FTLD, VCI, and cognitively healthy control subjects. The subgroups consisted of FTLD-TDP, FTLD-tau, and FTLD-FUS. A scale from 0 to 9 was used for assessment, with 0 being healthy LC and 9 being severely degenerated LC. The scoring system was based on the number of manually counted pigmented cells of the best-preserved nucleus as well as depigmentation. The highest degeneration score of 9 points was for 0–10 counted cells, followed by a score of 8 points for 11–20 counted cells, 6 points for 21–40 counted cells, 4 points for 41–60 counted cells, and 2 points for 61–80 cells. A healthy LC was considered to correspond to≥81 cells. An additional point was given if > 50% of the neurons substantially lacked pigmentation in the cases with a neuron count of 21 or more. The figure was made using Jamovi 2.2.2. FTLD, frontotemporal lobar dementia; FUS, fused in sarcoma; TDP, TAR-DNA binding protein 43; VCI, vascular cognitive impairment.
A macroscopic evaluation of the LC had been described in 87% of the cases (n = 131). A larger proportion of cases from the control and VCI groups had lacking information on the macroscopic appearance of the LC, thus, statistical analyses were conducted on the FTLD-TDP and FTLD-tau groups only (the FTLD-FUS [n = 3] group was not included in the statistical analysis). The median score was 0 (normal appearance) in the FTLD-TDP group and 1 (moderately pale or small) in the FTLD-tau group (p < 0.001 using the Kruskal–Wallis test for difference).
Information on disease duration was available in 68% (n = 30) of the FTLD-TDP cases, in 71% (n = 27) of the FTLD-tau cases, and in two of the three FTLD-FUS cases. The average duration of disease was 6.3 (SD 4.6) years and 6.0 (SD 4.1) years in the FTLD-TDP and FTLD-tau groups, respectively. Disease duration was four and 20 years in the two FTLD-FUS cases with available data. These differences were found to be not significant by the Kruskal–Wallis test (p = 0.74). Age significantly correlated with the LC score in the FTLD-tau group (p = 0.0012, rho = 0.50, 95% CI [0.26, 0.74]) and disease duration trended towards a correlation with LC score (p = 0.105, rho = 0.31, 95% CI [–0.010, 0.72]) but neither correlation was significant in the FTLD-TDP group (p = 0.26 and 0.40, respectively). The FTLD-FUS group was not included in the correlation analyses.
DISCUSSION
In this study, we analyzed the difference in LC degeneration, as mirrored by neuronal counts, between several proteinopathies of FTLD. FTLD-tau, FTLD-TDP, and FTLD-FUS demonstrated a more severe degeneration of the LC compared to controls. Additionally, the LC was more degenerated, both micro- and macroscopically, in the FTLD-tau group than in the FTLD-TDP group. Furthermore, there was a positive correlation between age and LC degeneration in the FTLD-tau group, but only a trend towards correlation between disease duration and LC degeneration. Microscopical degeneration of the LC did not differ between the VCI group and the cognitively healthy control group.
Methodologically, the present assessment of the LC degeneration, only including the number of remaining neurons and depigmentation, was a simplifying modification of an earlier-described assessment method where pigment spilling was also included [25, 26]. This was motivated by the observation that the cell counts alone correlated better with the total degree of LC degeneration than other factors [26, 34].
A degeneration of the LC in tau proteinopathies is consistent with previous reports on other tau-related diseases [20, 46]. This confirms recent findings that LC degeneration is more pronounced in FTLD-tau than in FTLD-TDP and that the degeneration in FTLD-tau is similar to that in AD [24]. Such a difference could be explained by the disparities in the pathological inclusion burden in the LC neurons between the groups [24].
The macroscopic evaluation of the LC did provide an indication for whether the LC is degenerated or not and could be of diagnostic guidance in the routine clinical setting. Since the LC was more affected in the FTLD-tau group than in the FTLD-TDP group, the macroscopic evaluation provides diagnostic information. In some cases, the macroscopic assessment did not correlate with the microscopic evaluation, indicating that a microscopic evaluation of the LC is necessary. These cases could be instances of a marked depigmentation of neurons despite a high neuronal count, resulting in discrepancy between the macroscopic and the microscopic score. Dissimilar results between macroscopic and microscopic assessments were encountered particularly in some cases of VCI (not specifically reported). The discrepancy could, for example, be caused by intercurrent edema of a recent ischemic event affecting the brain stem and the LC.
There are various means of assessing the LC. A reduction in the number of cells has been described in cognitive disorders such as AD and LBD [16, 47–49], while other studies have assessed a degeneration of the LC by measuring the amount of neuromelanin [24, 47]. In previous work from our group, it was concluded that cell count should be used as a method of assessing the LC, as it had a low intra- and interpersonal variability, and that additional assessment did not add diagnostic value [26, 34]. Moreover, a natural age-related increase in neuromelanin has been described, which could lead to various interpretations [50–53]. Nevertheless, additional aspects could be analyzed for a more detailed assessment [16, 55]. By using the LC for diagnostic guidance, the subsequent analyses could potentially be narrowed. However, criteria to help distinguish several cognitive disorders based on LC pathology require additional research and validation.
In this study, there was a positive correlation between LC degeneration and age in FTLD-tau but not in FTLD-TDP. Earlier studies revealed a reduction in the number of cells with age [47, 56]. This was contradicted by other reports when examining healthy brains without cognitive disorders [57–59]. The results indicate that the method used for assessing the LC is not sensitive to a physiological decrease in cell numbers but, rather, only to pathological cases [19, 25].
The duration of disease trended towards a positive correlation with LC degeneration in FTLD-tau but not in FTLD-TDP. Severity of clinical symptoms may potentially be associated with degree of LC degeneration. It has been reported that neuron loss in the LC is correlated to disease severity rather than to disease duration in FTLD-tau proteinopathies such as progressive supranuclear palsy [20, 25], and this association has also been reported in AD [60, 61].
A better differentiation of cognitive disorders postmortem could provide a basis for more robust clinical diagnostics, and a multimodal approach should be used for differentiation of FTLD subgroups in vivo. Earlier differentiation between the subgroups could perhaps be through the use of imaging techniques such as MRI [46, 63–65], where the LC can be visualized [66]. Since the present data demonstrate different macroscopic degeneration in FTLD subgroups and LC degeneration has been detected using MRI [60, 67], neuroimaging could potentially be used to differentiate between FTLD subgroups in the clinical setting.
Limitations
A limitation of this study is its retrospective nature with protocols not adjusted for the purpose of this study; in other words, the sections were not collected systematically, and the sectioning level of the LC could differ between cases. Consequently, this may have had an impact on the evaluation of the degeneration. The macroscopic evaluations did not follow any concrete criteria and had been described by various pathologists; such evaluations are based on experience and, therefore, can be subjective. The microscopic evaluations had been adapted to be as objective as possible, counting the number of cells; however, such reproducibility was not cross-checked in this study as it had been in earlier work [34].
Another limitation of this study is the potential referral bias for autopsy. It is possible that the more unclear cases were the ones sent for pathological examination. Additionally, there were very few cases of FTLD-FUS, and though they exhibited substantial LC degeneration, no conclusion could be made about this group. The method chosen also led to a lack of controls matched for age and gender, as the controls were retrieved from cases sent for pathological examinations. To correct for potentially confounding factors, a prospective study registering symptoms in a consistent manner with subsequent pathological examinations as well as genetic analyses would provide better insight into the effect of LC degeneration on FTLD.
Conclusion
The aim of this study was to compare the main FTLD subgroups with respect to LC degeneration. A greater degeneration was observed, microscopically and macroscopically, in FTLD-tau compared to FTLD-TDP. Additionally, the few FTLD-FUS cases revealed a severe degeneration of the LC. This study provides a simplified methodologic approach for neuropathological examinations of the LC. Additional prospective neuropathological studies and in vivo examinations are needed to better differentiate the subgroups of FTLD, to improve in vivo diagnostics and, possibly, the development of therapeutics.