
Abstract
We present the case of a cognitively unimpaired 77-year-old man with elevated, asymmetric, and longitudinally increasing Flortaucipir tau PET despite normal (visually negative) amyloid PET. His atypical tau PET signal persisted and globally increased in a follow-up scan five years later. Across eight years of observations, temporoparietal atrophy was observed consistent with tau PET patterns, but he retained the cognitively unimpaired classification. Altogether, his atypical tau PET signal is not explained by any known risk factors or alternative pathologies, and other imaging findings were not remarkable. He remains enrolled for further observation.
INTRODUCTION
During routine analysis of imaging from a cognitively unimpaired 77-year-old right-handed male participant of the Mayo Clinic Study of Aging (MCSA), investigators discovered atypically elevated, asymmetric Flortaucipir positron emission tomography (PET) positivity (T+) despite visually non-elevated amyloid PET (A–).
METHODS
The participant provided written consent with approval of the Mayo Clinic Institutional Review Board. He was only seen for regularly scheduled volunteer visits that included neuropsychiatric testing, magnetic resonance imaging (MRI), and PET. PET imaging included Fluorodeoxyglucose (FDG), amyloid PET (Pittsburgh Compound B; PiB), and tau PET (Flortaucipir) scans. Regional gray matter (GM) volume, total intracranial volume, white matter hyperintensity (WMH), and tau and amyloid PET standardized uptake value ratio (SUVR) measurements (referenced to cerebellar crus) were estimated using previously published automated methods for each scan [1–4].
RESULTS
Medical history
The participant described a history of emphysema and chronic obstructive pulmonary disease, obstructive sleep apnea, hypertension, and osteoarthritis of the knee. When asked specifically, he denied any history of any cognitive disorder among first-degree relatives (parents and siblings), and he denied any history of any head injuries that caused memory loss, unconsciousness, or required a doctor visit or hospitalization. He reported less than ten years of formal education.
PET (Figs. 1 3, top)
Three amyloid (PiB) PET scans at ages 69, 72, and 77 were all considered A–by an expert nuclear medicine radiologist (VJL). However, whole-brain SUVR measurements were suprathreshold (>1.48) [5, 6], which was attributed to age-typical off-target white matter (WM) binding. Flortaucipir tau PET scans at ages 72 and 77 both had substantial left-hemisphere-predominant GM signal. At age 72, only the temporal lobe was clearly suprathreshold (>1.25) [5, 6] (left: 1.52, right: 1.26). By age 77, all lobes were suprathreshold in both hemispheres with additional focal uptake in left-predominant frontal, parietal, and occipital regions. The highest SUVRs were both temporal (left 2.40, right 1.63). All scans were of good quality and all potential technical explanations for the atypically elevated signal (e.g., motion, attenuation correction error, misregistration) were excluded. A FDG PET was also performed at age 69 and was unremarkable, but this was early in his course and its later trajectory is unknown.
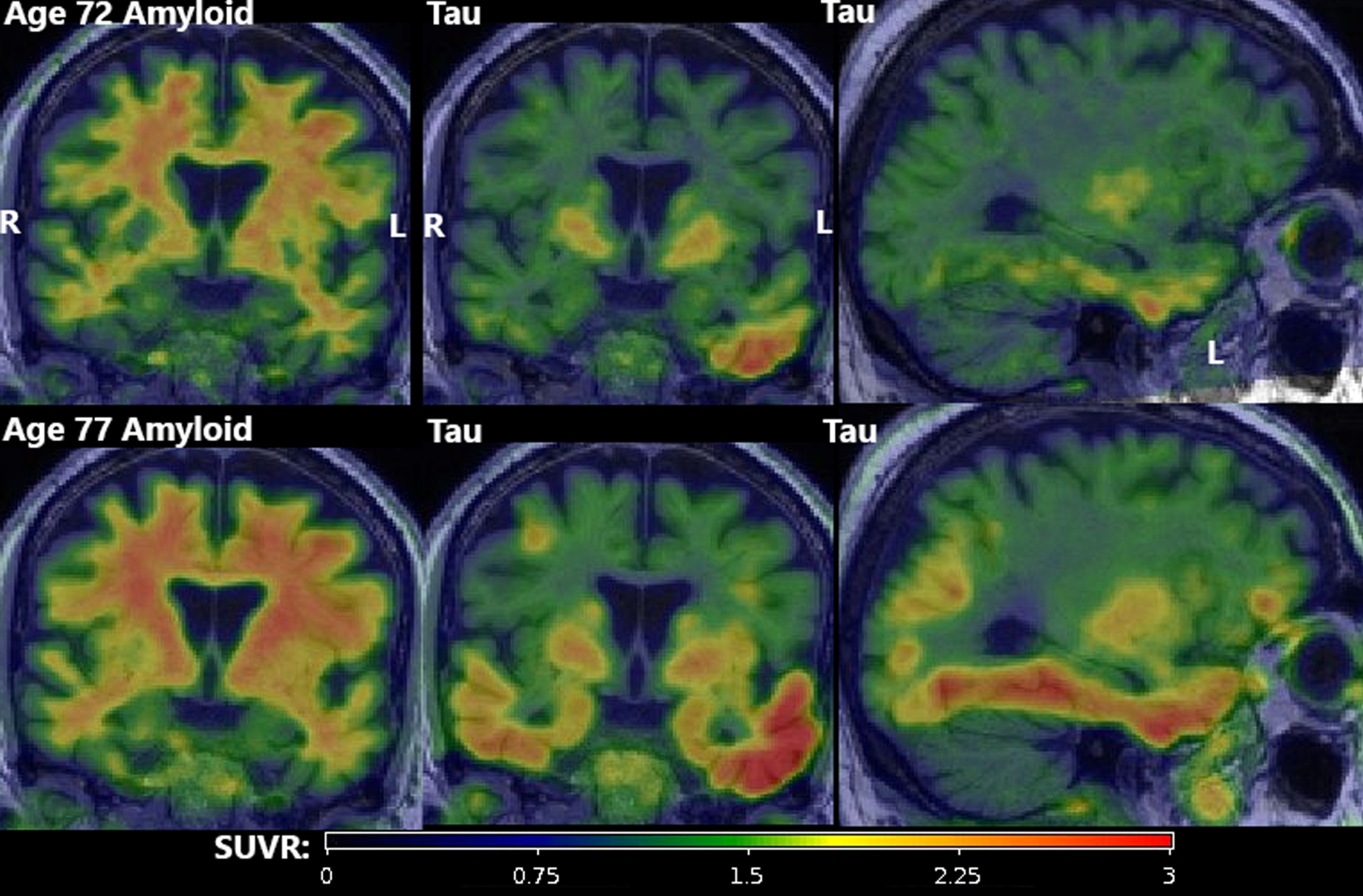
PET findings. Amyloid (first column; PiB) and tau PET (second two columns; Flortaucipir) at age 72 (top row) and age 77 (bottom row). All amyloid scans were visually negative (A–) despite quantitative elevation due to substantial but age-expected off-target binding in adjacent WM. Tau scans showed atypically high suprathreshold (T+) signal in an asymmetric (L > R) pattern primarily in the temporal lobe with focal uptake in the frontal, parietal, and occipital lobes. All scans were of good quality and all potential technical explanations for the atypically elevated signal (e.g., motion, attenuation correction error, misregistration) were excluded.
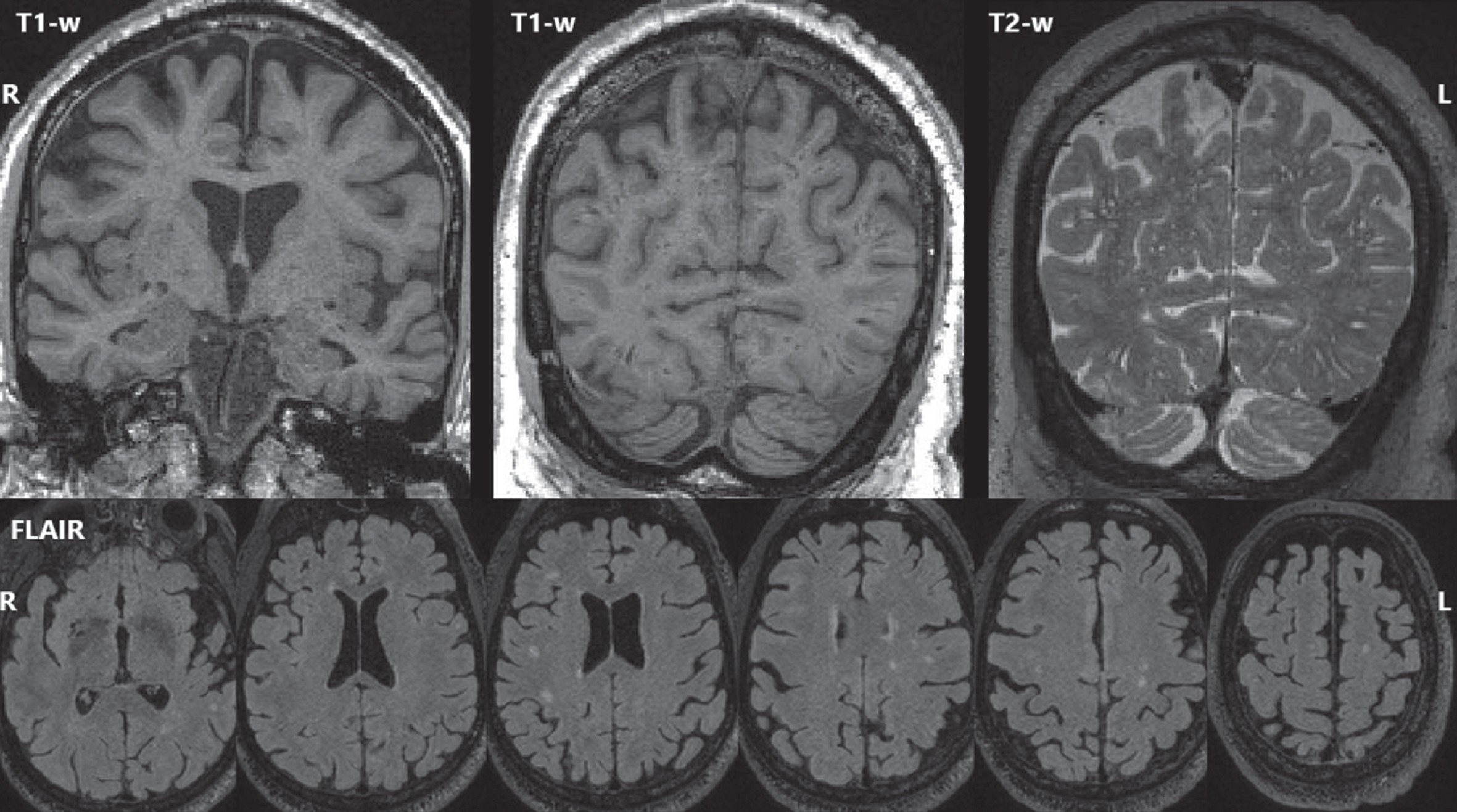
MRI findings. The most recent (age 77) T1-weighted MRI (top left, top center), and T2-weighted MRI (top right) showed mild global volume loss and extensive dilated perivascular spaces throughout the cerebrum. FLAIR MRI (bottom row) showed white matter hyperintensities (biomarkers of small vessel ischemic change) with an age-typical total volume but an atypical distribution with focal lesions scattered throughout deeper white matter rather than a more typical periventricular pattern.
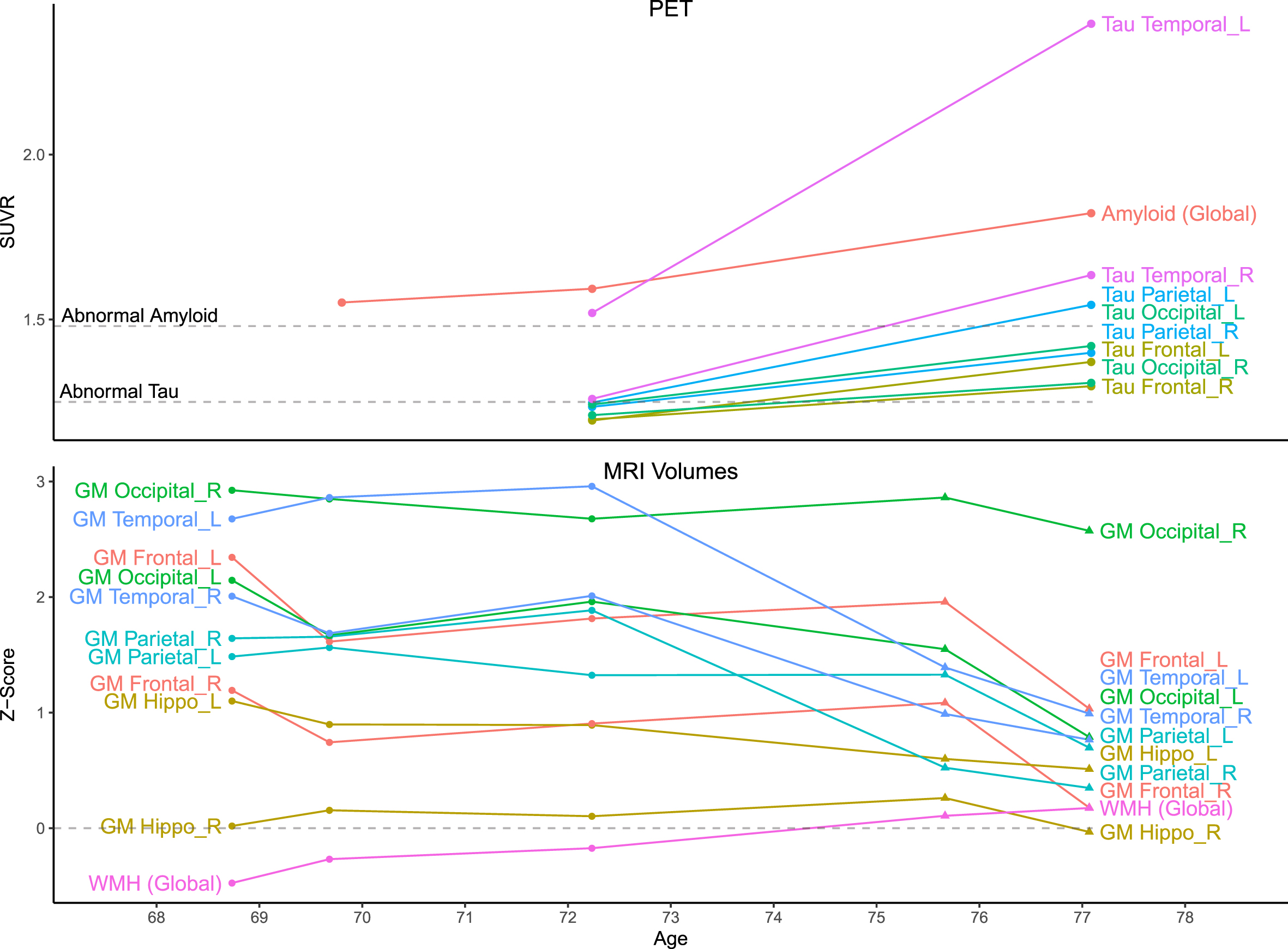
Quantitative data. Top) Amyloid (PiB) and tau (Flortaucipir) PET standardized uptake value ratio (SUVR) values were measured using a fully automated pipeline with a cerebellar crus reference region. Thresholds for amyloid positivity (A+: 1.48) and tau positivity (T+: 1.25) are shown. Amyloid scans were visually negative but SUVRs were suprathreshold due to off-target white matter binding. At age 72, tau SUVRs were suprathreshold only in the temporal lobe (L > R), but all were suprathreshold by age 77. Bottom) MRI volumes for each scan were normalized by total intracranial volume and z-scored relative to a sample of 169 unimpaired men ages 65–80 with Siemens MRI. Circles indicate timepoints with GE MRI and triangles with Siemens. Before z-scoring, GE-measured volumes were adjusted to better match Siemens using linear transformations derived for each region from a scan-rescan crossover dataset (n = 110; ages 34–97), but changes between these timepoints (age 72–75) should still be interpreted with caution. GM volumes were mostly stable until temporoparietal atrophy at ages 72–75, before global atrophy at 75–77. Relative to the reference group, GM volumes mostly began far above average and remained above average after declines, except for the right hippocampus (which was near average). WMH volumes slowly grew but remained near average.
MRI (Figs. 2 3, bottom)
Five 3T MRIs were acquired between ages 68–77. At age 77, there was mild global volume loss, but all GM volume measurements except right hippocampus exceeded reference group averages. Longitudinally, GM volumes were largely stable until temporoparietal atrophy at ages 72–75, then greater widespread atrophy at 75–77. The greatest atrophy occurred in the left temporal lobe, consistent with tau PET distribution. WMH (biomarkers of small vessel ischemic change) were also observed with total volume similar to the reference group but an atypical distribution of scattered deeper focal lesions rather than a typical periventricular predominance. Extensive dilated perivascular spaces were observed throughout the cerebrum including the temporal lobes and the basal ganglia.
Cognition
Testing was performed roughly annually between ages 68-77. Details are withheld to protect participant privacy, but he retained a status of cognitively unimpaired throughout the duration.
Genotyping
We assessed his genotypes for several common genetic variants associated with risk of neurodegenerative diseases (including in APOE, MAPT, TOMM40, GRN, and C9ORF72, among others) and found no overtly explanatory patterns. However, these assessments used genome-wide association study (GWAS) data, which does not encompass all base pairs in the genome and cannot assess rarer mutations. Further details are withheld to protect participant privacy.
DISCUSSION
The participant’s tau PET had widespread, asymmetric elevation that quickly rose longitudinally despite peri-threshold, visually A–amyloid PET. Elevated tau PET signal outside the medial temporal lobe (T+) only typically occurs in A+ individuals [7–9]. Within the medial temporal lobe, elevated tau PET signal in A– individuals is common [8, 10] and associated with Primary Age-Related Tauopathy (PART) [11, 12], but this participant’s signal greatly exceeds that typical for PART in both magnitude and distribution. Weak tau PET signal is often observed in juxtacortical WM of A– individuals with primary tauopathies [13–15], but this participant’s scan had much higher SUVR than is typical for those cases, and the signal was primarily located in GM. Similar GM A–T+ signal has been associated with rare MAPT mutations [16–21] whose status in this individual are not known (not all were included in our GWAS dataset), but those cases as described have included more bilateral/symmetric involvement. Furthermore, this individual’s pattern of common genetic variation at targeted risk alleles was observed frequently within the MCSA cohort, with no other known individuals having comparable tau PET patterns. His elevated signal may also be due to a previously unknown category of off-target binding. Therefore, the imaging findings are not explained by any known genetic factors. We have never observed a similar case among the approximately 1100 unimpaired MCSA participants with amyloid and tau PET.
One possible explanation for his unimpaired cognition despite high tau levels may be higher MRI GM volumes in the earliest visits, which were far above average (except right hippocampus). Even at the latest visit, GM volumes remained above average, which could explain his cognitive resilience. However, his education level (surrogate of cognitive reserve/resilience) of <10 years was not a likely explanation. The left-temporal tau predominance would be anticipated to yield language-domain decline, but he remained cognitively unimpaired. The right hippocampus had the lowest GM volume z-score relative to the population, but it was never significantly below average and remained relatively stable over time. The left hippocampus had a higher z-score than the right at baseline, but it showed stronger decline over time, consistent with the left-predominant tau pattern. The additional MRI-observed vascular abnormalities were consistent with the reported pulmonary conditions and sleep disorders but were not of a burden that would be considered unusual in this age and risk factor range.
Altogether, the participant’s unusual tau PET signal is not explained by any known pathologies or risk factors, and other imaging findings were not remarkable. He remains enrolled for further observation.
Footnotes
ACKNOWLEDGMENTS
The authors give thanks to all the volunteers, participants, and coordinators who contributed to this research. We gratefully thank our funding sources that made this work possible: NIH grants R37 AG011378, R01 AG041851, R01 AG056366, U01 AG006786, P50 AG016574, P30 AG062677, R01 AG034676, R01 NS097495, Gerald and Henrietta Rauenhorst Foundation, Elsie and Marvin Dekelboum Family Foundation, Alexander Family Alzheimer’s Disease Research Professorship of the Mayo Clinic, Liston Award, Schuler Foundation, and Mayo Foundation for Medical Education and Research. We also thank AVID Radiopharmaceuticals, Inc., for their support in supplying AV-1451 precursor, chemistry production advice, and FDA regulatory cross-filing permission and documentation needed for this work.
DATA AND CODE AVAILABILITY STATEMENT
This study describes a specific individual participant. To protect that participant’s privacy, these data will not be shared. In general, data from the Mayo Clinic Study of Aging are made available to qualified academic and industry researchers by request to the Mayo Clinic Study of Aging/Alzheimer’s Disease Research Center Executive Committee.