
Abstract
Coronavirus (COVID-19) has emerged as a human catastrophe worldwide, and it has impacted human life more detrimentally than the combined effect of World Wars I and II. Various research studies reported that the disease is not confined to the respiratory system but also leads to neurological and neuropsychiatric disorders suggesting that the virus is potent to affect the central nervous system (CNS). Moreover, the damage to CNS may continue to rise even after the COVID-19 infection subsides which may further induce a long-term impact on the brain, resulting in cognitive impairment. Neuroimaging techniques is the ideal platform to detect and quantify pathological manifestations in the brain of COVID-19 survivors. In this context, a scheme based on structural, spectroscopic, and behavioral studies could be executed to monitor the gradual changes in the brain non-invasively due to COVID-19 which may further help in quantifying the impact of COVID-19 on the mental health of the survivors. Extensive research is required in this direction for identifying the mechanism and implications of COVID-19 in the brain. Cohort studies are urgently required for monitoring the effects of this pandemic on individuals of various subtypes longitudinally.
Keywords
INTRODUCTION
Coronavirus (COVID-19) is an infectious disease caused by severe acute respiratory syndrome corona virus-2 (SARS-CoV-2). COVID-19 came into existence from Wuhan City, China in December 2019 [1]. The World Health Organization (WHO) declared COVID-19 a pandemic on 11 March 2020 due to the continual dissemination of this disease throughout the world [2]. According to the WHO, as of 29 June 2021, a total of 181,176,715 cases including 3,930,496 deaths have been confirmed globally due to COVID-19, where 30,316,897 cases with 397,637 fatalities are reported solely from India [3]. A variety of precautionary measures have been outlined by the WHO to protect humans from this infectious disease such as social distancing, wearing a mask, avoiding crowds, and regular cleaning of hands, etc. [4]. Despite considering these protective measures, the virus is still continuously spreading worldwide and the number of individuals affecting by COVID-19 is increasing day by day. The mortality rate is too high in elderly patients with low immunity due to nutritional deficiencies [5]. In view of this, the identification of effective drugs is vital for eradicating viral load from the body of the individuals affected with COVID-19 [6]. According to the WHO, a total of fifteen vaccines have been developed up to now and some of them are approved to use on an emergency basis from the United States of America, Germany, United Kingdom, Russia, China and India.
The main characteristic of this disease is pneumonia [7]; however, cough, fever, dyspnea, anosmia, myalgia, sore throat, gastrointestinal penetrations, and rhinorrhea are the clinical manifestations that are possessed by an individual infected by COVID-19 [2, 8–10]. The infection is not limited to the respiratory system but also adversely affects other vital organs such as the heart, liver, and kidney as well as brain [10–12]. Increased loneliness, isolation, distress, anxiety, and depression can trigger the onset of psychological illness in people [9, 13]. As a matter of this fact, post-traumatic stress disorder, depression, obsessive-compulsive disorder, and anxiety have been found as the most prevalent disorders in the patients recovered from COVID-19 [14–16].
Human ability to perceive, manage, update, and act on information in accordance with past experiences contribute to cognitive function which largely depends on the structural and functional integrity of the prefrontal cortex [17]. Exposure to stress can disrupt prefrontal cortex (PFC) function, causing cognitive impairments [18, 19]. Numerous mental illnesses—including obsessive-compulsive disorder, depression, and anxiety disorders, etc., are characterized by PFC dysfunction [20]. Two recent studies, one from the ward of a general hospital and the other from a temporary quarantine facility, have shown that as high as 9.4%, 15.1%, 24.5%, and 96.2% of the COVID-19 patients had severe depressive, anxiety, and post-traumatic stress disorder symptoms. COVID-19 itself can put a lot of stress on the brain due to lockdown and complete isolation [21–23]. Many researchers and scientists have determined the presence of the SARS-CoV-2 virus in a variety of brain tissues such as cerebrospinal fluid (CSF), glial, and neuronal cells via genomic sequencing which is indicative of serious damage to the CNS [24]. The presence of SARS-CoV-2 RNA in CSF suggests a possible association of SARS-CoV-2 infection with neurological symptoms in COVID-19 patients [10, 25–27].
The FLAIR and diffusion weighted images have also reported non confluent multifocal white matter hyper-intensities in the affected individuals along with other imaging alterations [8, 28–30]. Moreover, the damage to CNS may continue to rise even after the pulmonary infection subsides. COVID-19 infection in the brain can be associated with ext-reme physical and psychological stress which stimulates the hypothalamic-pituitary-adrenal axis and aggravates neuroinflammation [31]. It is important to note from a previous study that cognitive disorders and neuroinflammation are correlated with each other [9, 32]. A significant decline in cognitive functioning has also been identified through low scores of neuropsychological tests (continuous performance test), greater reaction time, a deficit in attention and executive functioning of COVID-19 recovered patients [21, 33–36]. Structural changes have also been determined in the brain of COVID-19 patients as compared to the non-infected ones from a variety of studies where the researchers claimed enlarged volumes of several brain regions like the hippocampus, Heschl’s gyrus, olfactory cortices, cingulate gyrus, and Rolandic operculum [23, 37]. Anatomically distinct regions of the nasopharynx and brain show the presence of SARS-CoV-2 RNA and protein. This has been confirmed by the autopsy studies of the patients [37]. Furthermore, a description of morphological changes related to the infection such as thromboembolic ischemic infarction of the CNS has been given. This suggests the evidence of SARS-CoV-2 neurotropism. A meta-analysis study indicates that no virus is present in the CSF of patients and there is no direct neuroinvasion [38]. However, other groups of researchers have suggested that SARS-CoV-2 seems to follow neuroanatomical structures which further penetrates into defined neuroanatomical areas such as the primary respiratory and cardiovascular control center in the medulla oblongata [37, 39]. Therefore, it is important to implement long-term studies for determining the correlations among the clinical profile, laboratory investigations, and radiological observations besides neuropathological studies for an in-depth understanding of the neurological manifestations in the patients recovered from COVID-19. In this context, a scheme for examining the glutathione (GSH), glutamatergic, and GABAergic systems in hippocampal and dorsolateral prefrontal cortex (DLPFC) area of the brain has been proposed. Additionally, the implications of neuropsychological evaluation in diagnosing early mental health problems in COVID-19 survivors has also been outlined. The major rationale behind the proposed scheme is the increased level of oxidative stress in COVID-19 survivors which further contributes to the pathogenesis of several neurological diseases due to depletion of antioxidants.
COVID-19 INFECTION IN BRAIN: A POSSIBLE MECHANISM
Recent research findings suggest that coronavirus may enter the CNS via two pathways: direct [40] and indirect [41]. In the direct pathway, the virus may enter via the blood-brain barrier, blood-CSF barrier, and retrograde axonal transport to reach the neuronal cell bodies in the CNS (see Fig. 1). The olfactory, respiratory, and enteric nervous system networks are the three possible pathways through which retrograde axonal transport can occur [12–15]. Ongoing research suggests that SARS-CoV-2 is likely to enter the nervous system by crossing the neural–mucosal interface in olfactory mucosa, which subsequently deteriorates the close domain of olfactory endothelial, mucosal, and nervous tissue, involving the delicate sensory and olfactory nerve endings [37]. Other researchers have also reported that from the olfactory bulb, the virus may tend to target deeper parts of the brain such as the brainstem and thalamus by trans-synaptic transfer which has also been described for several distinct viral diseases. They suggest that the infection of the respiratory center of the brain might take place which explains the respiratory breakdown in patients [42].
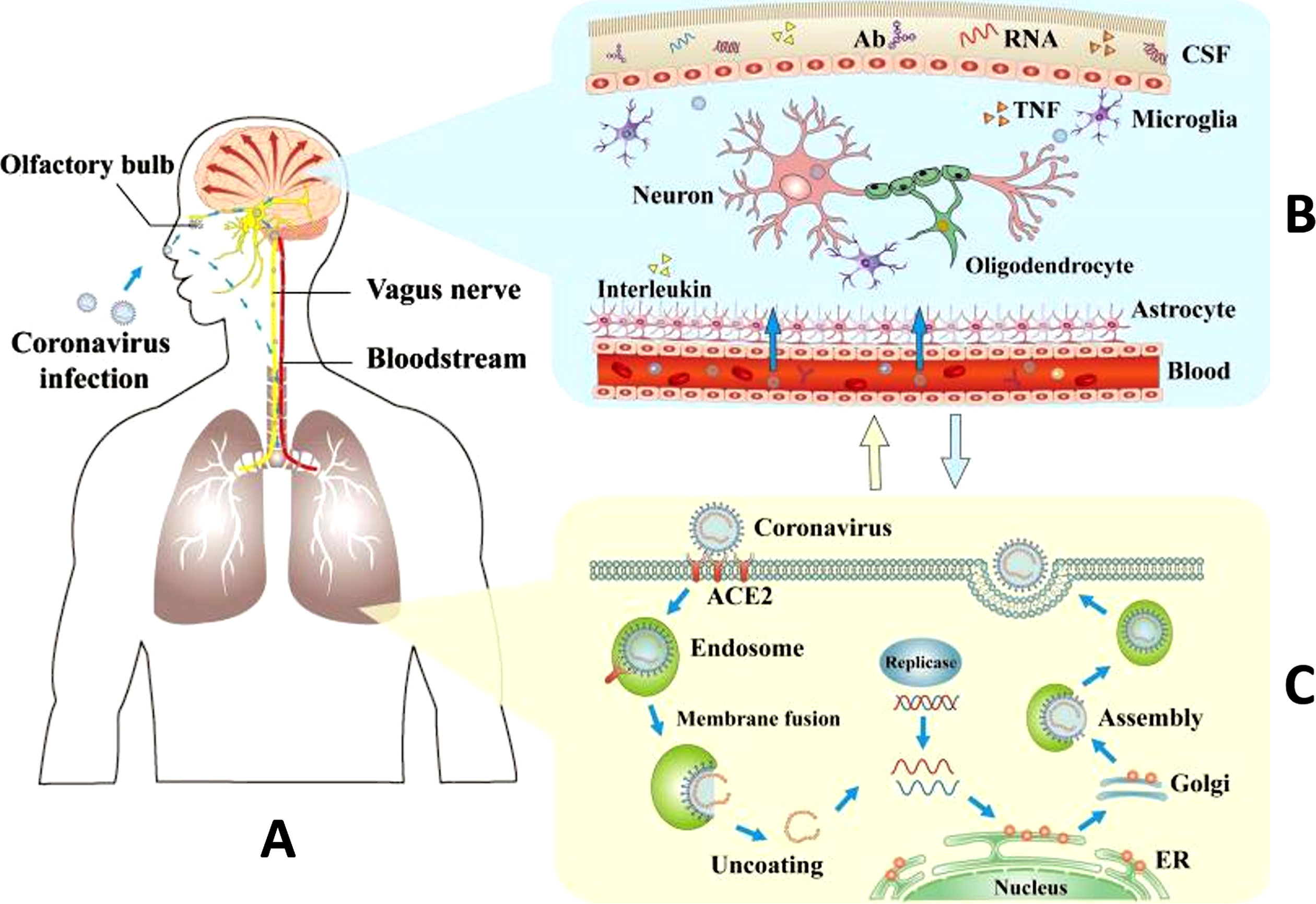
A schematic representation of COVID-19 virus routes to the respiratory system and the brain. A) COVID-19 infection routes for brain and lung damage, B) invasion of the SARS-CoV-2 into the nervous system through the blood-brain barrier, and C) intrusion of SARS-CoV-2 into lungs by fusing with an angiotensin-converting enzyme (ACE2). Reproduced with permission from the publisher [40]. Ab, antibody; ACE2, angiotensin-converting enzyme 2; CSF, cerebrospinal fluid; ER, endoplasmic reticulum; TNF, tumor necrosis factor.
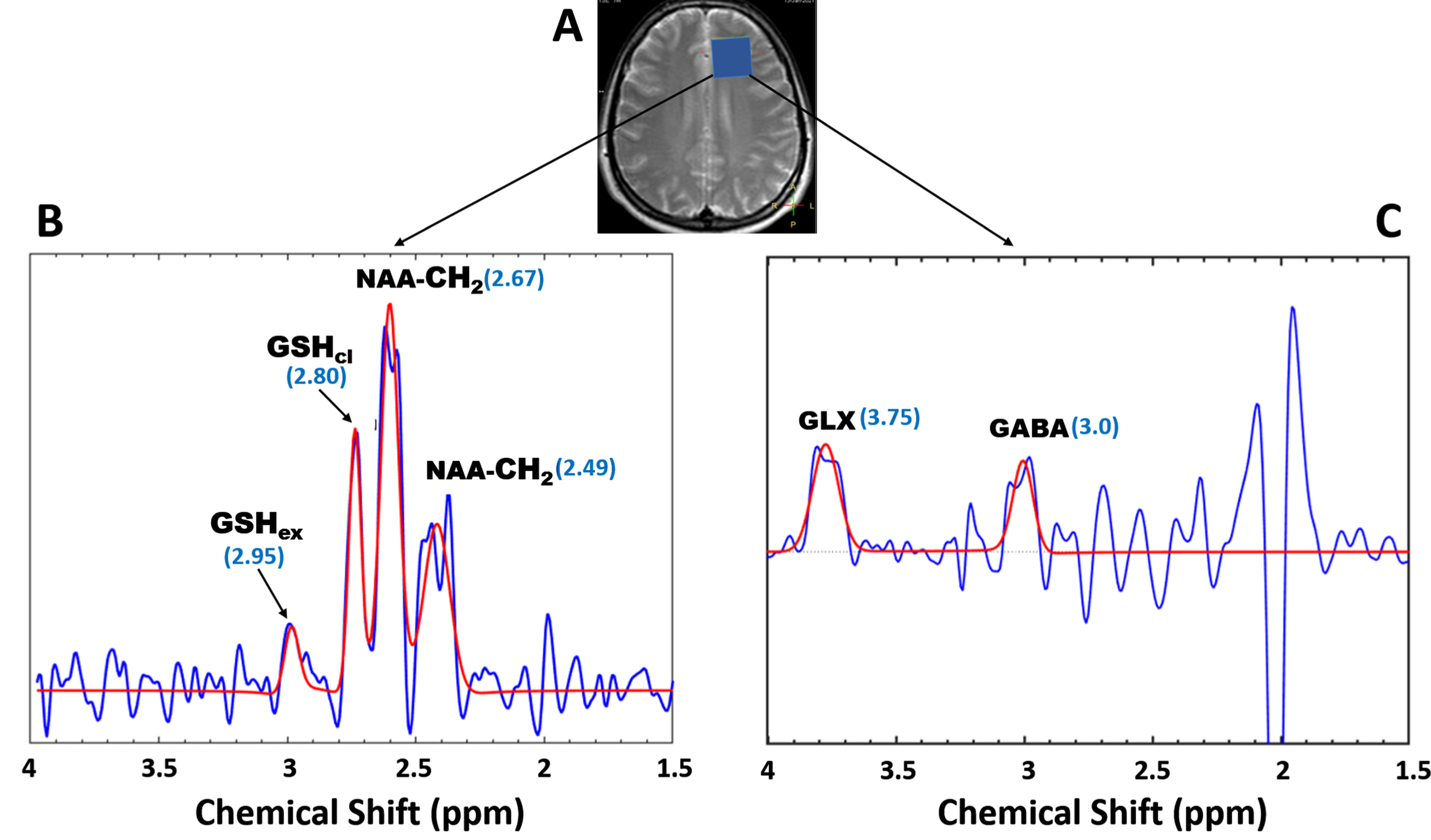
Detection of GSH, GABA+, and Glx metabolite from the DLPFC of a healthy young volunteer using 3T (Philips, Innova) scanner at NBRC. A) T2w image with a voxel placed in DLPFC region in the brain for acquiring GSH and GABA. B) Closed and extended GSH conformers with at 2.95 and 2.80 ppm [46] aspartate moiety signals from N-Acetyl-Aspartate at 2.67 ppm (NAA). C) MRS signal representing the peaks of GABA and glutamine/glutamate (Glx) where the baseline spectra and fitted spectra are shown in blue and red, respectively.
In respect to the indirect mechanisms, researchers proposed that respiratory failure-induced hypoxia and immune system malfunction may lead to neu-ronal damage [4, 43]. The pro-inflammatory cytok-ines (IL-6 and TNF-α) are released in abundance in response to a viral infection which causes excessive inflammation of the blood-brain barrier [10, 41]. Consequently, the permeability of the blood-brain barrier is increased which further provides a pathway for the virus to enter the brain indirectly. Infection of the peripheral myeloid cells is another possibility through which the virus may give rise to the psy-chiatric symptoms indirectly by causing neuroinflammation and virus-induced neuropathology [44].
OXIDATIVE STRESS, ANTIOXIDANTS AND NEUROTRANSMITTERS
Oxidative stress can be described as the increased production of reactive oxygen species and depletion of antioxidants which further contributes to the pathogenesis of several neurological diseases [5]. In patients infected with COVID-19, a high neutrophil to lymphocyte ratio has been observed which is strongly associated with an excessive level of reactive oxygen species. Consequently, the increasing load of viral infection causes a decrease in antioxidant defense. GSH deficiency appears to be a primary factor in enhancing SARS-CoV-2-induced oxidative damage which further gives rise to many clinical expressions such as multiorgan failure, acute respiratory distress syndrome, and even death in patients with COVID-19 infection [40]. GSH is the most important antioxidant in the human brain which plays a vital role in antioxidant defense. A variety of studies related to postmortem and neurological disorders have observed a significant depletion in GSH through magnetic resonance spectroscopy (MRS) [45]. Detection of extended and closed conformers of GSH has also been performed using the MEGA-PRESS sequence [46]. Alterations of GSH conformers is also detected [47]. Thus, measuring GSH for comparison between patient and control groups can be performed. Recently, it has also been found that GSH and its precursor’s supplements aid in recovery from respiratory distress in patients infected with COVID-19 [48, 49]. GSH has been identified as a source that can inhibit the main protease (Mpro) of COVID-19 [50]. In this context, the use of GSH as a supportive strategy for the treatment of COVID-19 infection can be recommended after a successful trial.
Primary excitatory and inhibitory neurotransmitters, i.e., GABA and glutamate also play a key role in modulating activity in the brain circuitry [51, 52]. Prolonged stress can cause loss of prefrontal glutamate transmission that may alter the hippocampal memory formation leading to dysfunction in cognitive function [53]. Dysfunction of the glutamatergic system can give rise to defects in neurotransmission, and cell viability which is further implicated in various psychiatric disorders [54]. Stress-induced alterations in the functionality of GABAergic inhibitory neurotransmission and synaptic integrity in the PFC may lead to dysfunction of PFC microcircuitry. This may further trigger cognitive impairments due to disruption in the execution of behavioral responses [55]. Therefore, the level of glutamate and GABA can serve as a promising parameter to monitor mental health and psychiatric disease-associated conditions. SARS-CoV-2 has neurotrophic properties which cause various CNS manifestations including psychiatric diseases [56]. There has been growing evidence of patients suffering from psychiatric diseases possibly due to COVID-19 [57]. In view of this, the involvement of GABAgeric neuronal dysfunction in psychiatric disorders and associated mechanism has become an active area of research. Many studies have shown heterogeneous results while measuring the GABA level in patients with psychiatric disorders [58]. The level of GABA for some patients has increased while the GABA level remained unaltered for other patients. Hence, a longitudinal follow-up study can also be performed to correlate the GABA level with psychiatric problems.
All the above-discussed antioxidants and neurotransmitters have potential implications for psychiatric disorders in COVID-19 affected patients. Implementation and validation of imaging and spectroscopy technologies (MRI and MRS) can help in finding out structural as well as metabolic changes in the brain [59]. Literature describing the neurologic symptoms of COVID-19 infection is increasing rapidly. Despite this, there are only a few published sources that demonstrate the findings based on neuroimaging techniques to monitor neurological infection in COVID-19 patients [29]. Researchers are analyzing the hyperintensities from FLAIR images and metabolites information from single-voxel MRS which indicates the changes in structure and the level of metabolites in the brain, respectively [60, 61]. Based on the prior knowledge, we are proposing a scheme for examining the GSH, glutamatergic systems in the hippocampal and dorsolateral prefrontal cortex area of the brain. Additionally, a neuropsychological evaluation is also likely to help in diagnosing the mental health problems in COVID -19 survivors [62].
CONCLUSION
In this COVID-19 pandemic situation, worldwide intense efforts have helped to detect the pathology of the SARS-CoV-2 virus in humans and determined the post-recovery effects of the virus on their mental health. A variety of case studies and reports have suggested a probable relationship between the viral infection due to SARS-CoV-2, oxidative stress, and neurological symptoms. The possibility of gradual damage to the brain and indistinct neurologic clinical manifestation requires further investigation to determine its long-term neurologic consequences. The non-invasive imagining-based strategy supported by psychiatric and neuropsychological evaluation could be a combined initiative in the direction of finding a correlation between the alteration in antioxidant’s and neurotransmitters’ concentration besides the structural changes in the brain to quantify the neurological impact caused by the virus on the mental health of COVID-19 survivors. This manuscript is a sincere attempt to highlight the impact of the SARS-CoV-2 for neurological and neuropsychiatric manifestation to make a top research priority. We have initiated cohort study specifically focused on mental health monitoring using brain structural and neurochemical data by MRI/MRS and behavioral data analysis longitudinally.