
Abstract
Background:
Epidemiologic studies have provided inconclusive evidence for a protective effect of caffeine consumption on risk of dementia and cognitive decline.
Objective:
To summarize literature on the association between caffeine and 1) the risk of dementia and/or cognitive decline, and 2) cognitive performance in individuals with mild cognitive impairment (MCI) or dementia, and 3) to examine the effect of study characteristics by categorizing studies based on caffeine source, quantity and other possible confounders.
Methods:
We performed a systematic review of caffeine effects by assessing overall study outcomes; positive, negative or no effect. Our literature search identified 61 eligible studies performed between 1990 and 2020.
Results:
For studies analyzing the association between caffeine and the risk of dementia and/or cognitive decline, 16/57 (28%) studies including a total of 40,707/153,070 (27%) subjects reported positive study outcomes, and 30/57 (53%) studies including 71,219/153,070 (47%) subjects showed positive results that were dependent on study characteristics. Caffeine effects were more often positive when consumed in moderate quantities (100–400 mg/d), consumed in coffee or green tea, and in women. Furthermore, four studies evaluated the relationship between caffeine consumption and cognitive function in cognitively impaired individuals and the majority (3/4 [75% ]) of studies including 272/289 subjects (94%) reported positive outcomes.
Conclusion:
This review suggests that caffeine consumption, especially moderate quantities consumed through coffee or green tea and in women, may reduce the risk of dementia and cognitive decline, and may ameliorate cognitive decline in cognitively impaired individuals.
INTRODUCTION
Dementia is a clinical syndrome characterized by progressive deterioration of cognitive functions and loss of independence in activities of daily living. App-roximately 50 million people are living with dementia worldwide. This number is continuously rising [1], and in 2017 the World Health Organization listed dementia as a public health priority [2]. A range of neuropathological disease entities may underlie a dementia syndrome, including Alzheimer’s disease (AD), vascular pathology (VaD), Lewy bodies (DLB), Parkinson’s disease (PD), or frontotemporal lobar degeneration [1]. Many factors such as cardio- and cerebrovascular disease, metabolism, psychiatric conditions, lifestyle, and education, potentially contribute to the risk of different types of dementia [3]. Furthermore, recent studies have suggested endo- and neurocrine interactions between gut microbiota and the brain (i.e., the microbiota-gut-brain axis [4, 5]) and that dietary factors such as caffeine intake can thereby influence the risk of dementia [6].
Caffeine is a psychoactive substance that is present in many beverages and some foods. The most widely known and consumed caffeine source is coffee, but caffeine can also be found in tea, energy drinks, car-bonated soft drinks, fruits, and cocoa-containing foods [7, 8]. After caffeine ingestion the substance is absorbed into the bloodstream via the gastrointes-tinal tract. From there, caffeine is distributed throughout the entire body. Caffeine biologically acts as an adenosine A1 and A2A receptor antagonist, and these receptors are widely distributed throughout the central and peripheral nervous system [9]. By blocking adenosine receptors, caffeine is capable of exerting effects on metabolism, the cardiovascular system, the respiratory system, and neuroinflammatory, neuromodulatory, and neuroprotective processes [10, 11]. More specifically, caffeine may stimulate gastric acid secretion and vasoconstriction, elevate the heart rate and blood pressure, increase the respiratory rate, and ultimately decrease neurodegeneration. Caffeine is able to enhance alertness, wakefulness, psychomotor vigilance, and memory, possibly also through an effect on NMDA receptors [12–14]. Furthermore, caffeine may reduce neuroinflammation and afford neuroprotection, through the consecutive lowering of extracellular calcium, glutamate release from the cell, and microglial activation [15]. There are also health risks associated with excessive caffeine consumption, including anxiety, panic attacks, psychosis, mania, tension, nervousness, irritability, restlessness, nausea, palpitations, insomnia, and diuresis [16].
Research in animal models indicates that caffeine can ameliorate cognitive decline [17]. Studies assessing possible mechanisms underlying this effect have suggested that the effects of caffeine on A2A receptors can control abnormal synaptic plasticity and synaptotoxicity [18, 19]. Other studies have posited that caffeine intake may delay or reduce the risk of AD by decreasing hippocampal amyloid-β levels in transgenic mice through A2A receptor blockade [20, 21].
In human epidemiological studies, results for the protective effects of caffeine on cognitive decline and dementia have been mixed. Some studies suggest positive influences of caffeine intake on neurological disorders and dementia [22, 23], while other studies have found no associations between caffeine and de-mentia [24, 25]. The association between caffeine consumption, cognitive decline, and dementia therefore remains inconclusive.
Here, we summarize the available literature on this topic and provide a systematic review. We aimed to address whether there is an association between caffeine and 1) the risk of dementia and/or cognitive decline, and 2) cognitive function in already cognitively impaired individuals (i.e., MCI or dementia). We further aimed to examine the effects of study characteristics (e.g., caffeine source and quantity) and demographic variables of the study sample (e.g., age and sex) on study outcomes.
METHODS
Study selection procedure
We searched the PubMed and Web of Science databases for studies published before June 2, 2020, using the following (combination of) search terms: ‘caffeine’, ‘coffee’, ‘tea’, AND ‘dementia’ OR ‘Al-zheimer(’s)’, AND ‘cognitive’ or ‘cognition’. Only peer-reviewed articles on studies in humans that were published in English, were eligible for inclusion in this pre-determined systematic review. Cross references were additionally assessed for eligibility. We included cognitively unimpaired individuals as well as individuals diagnosed with any type of dementia and/or MCI. The main criteria for article selection were 1) provision of information on the relation between caffeine consumption and the risk of dementia/cognitive decline, and/or 2) assessment of the association of caffeine on cognitive function in individuals with mild cognitive impairment (MCI) or dementia. Because many studies included a mixed sample of persons with dementia and MCI, both groups were taken together and termed ‘cognitively impaired’ subjects. We included any paper that des-cribed original research, regardless of study design, and, therefore, cross-sectional, longitudinal, case-control, controlled trials, cohort, and pilot studies were all assessed in the present review.
Risk of bias assessment
This review was performed according to the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement (Supplementary Table 1) [26]. The risk of bias for each study was assessed using the Cochrane Collaboration’s tool for non-randomized studies for interventions (ROBINS-I) [27]. Several risk of bias domains were evaluated for each study, including bias due to confounding fac-tors, subject selection, classification of intervention, deviation from intended intervention, missing data, outcome measurement and reporting of results. Each domain was rated as ‘low’, ‘moderate’, ‘serious’, or ‘critical’ risk of bias. An overall risk of bias was de-rived from the quality assessment across all domains of the remaining studies. These judgements were performed independently by two authors (A.C. and C.G.) and final assessment was determined by consensus. Our analyses were confined to studies with low and moderate risk of bias, as studies with serious or critical risk of bias were excluded from the analyses.
Data analysis
Relevant data from the included studies were ex-tracted in piloted forms. Outcome measures in the primary examination were based on overall study outcomes regarding the association between caffeine and 1) the risk of dementia and/or cognitive decline and 2) cognitive function in cognitively impaired in-dividuals. Secondary analyses included examination of the effects of caffeine source (coffee, tea, pure caf-feine, or multiple caffeine containing sources), and quantity (frequency and dosage), and possible confounders (e.g., age or sex), on study outcomes. Based on a previous study [28], the quantity of caffeine con-sumption was divided into three categories: low- (<100 mg/d), moderate- (100–400 mg/d), and high caffeine consumption (>400 mg/d). In accordance with the concentrations of caffeine across sources (i.e., 71–220 mg caffeine/150 ml for coffee and 32–42 mg caffeine/150 ml for tea [29]), moderate caffeine consumption will be defined as 1–4 cups of coffee or 3–10 cups of tea per day. Low caffeine consumption will be defined as <1 cup of coffee or <3 cups of tea per day, and high caffeine consumption will be defined as >4 cups of coffee or >10 cups of tea per day. Outcomes were defined as positive (caffeine improved cognition or slowed down cognitive decline), negative (negative association with cognition), or no association (no relation between caffeine and cognition). Study outcomes could also be mixed, for instance when positive effects were only found in a subset of the sample or when study outcomes were dependent on study characteristics, like caffeine source used.
RESULTS
Study selection and characteristics
The identification of relevant studies is illust-rated in a flow diagram (Fig. 1). Through database searches on PubMed, Web of Science, and cross references, we identified a total of 629 records. First, we excluded 522 articles, including 160 duplicates, based on review of the title and abstract. After full-text assessment of the remaining 107 articles, we excluded 44 articles that had highly overlapping study populations (n = 7), incompatible study designs (n = 4), no suitable cognitive outcome measures (n = 12), only non-caffeine effects (n = 11), or combined interventions (n = 10) (Supplementary Table 2). The remaining 63 studies were assessed for risk of bias, which resulted in the exclusion of two studies [30, 31] (see “Risk of bias” section). The final selection (61 studies) comprised 48 cohort studies, nine case-control studies, three randomized controlled trials, and one pilot study.
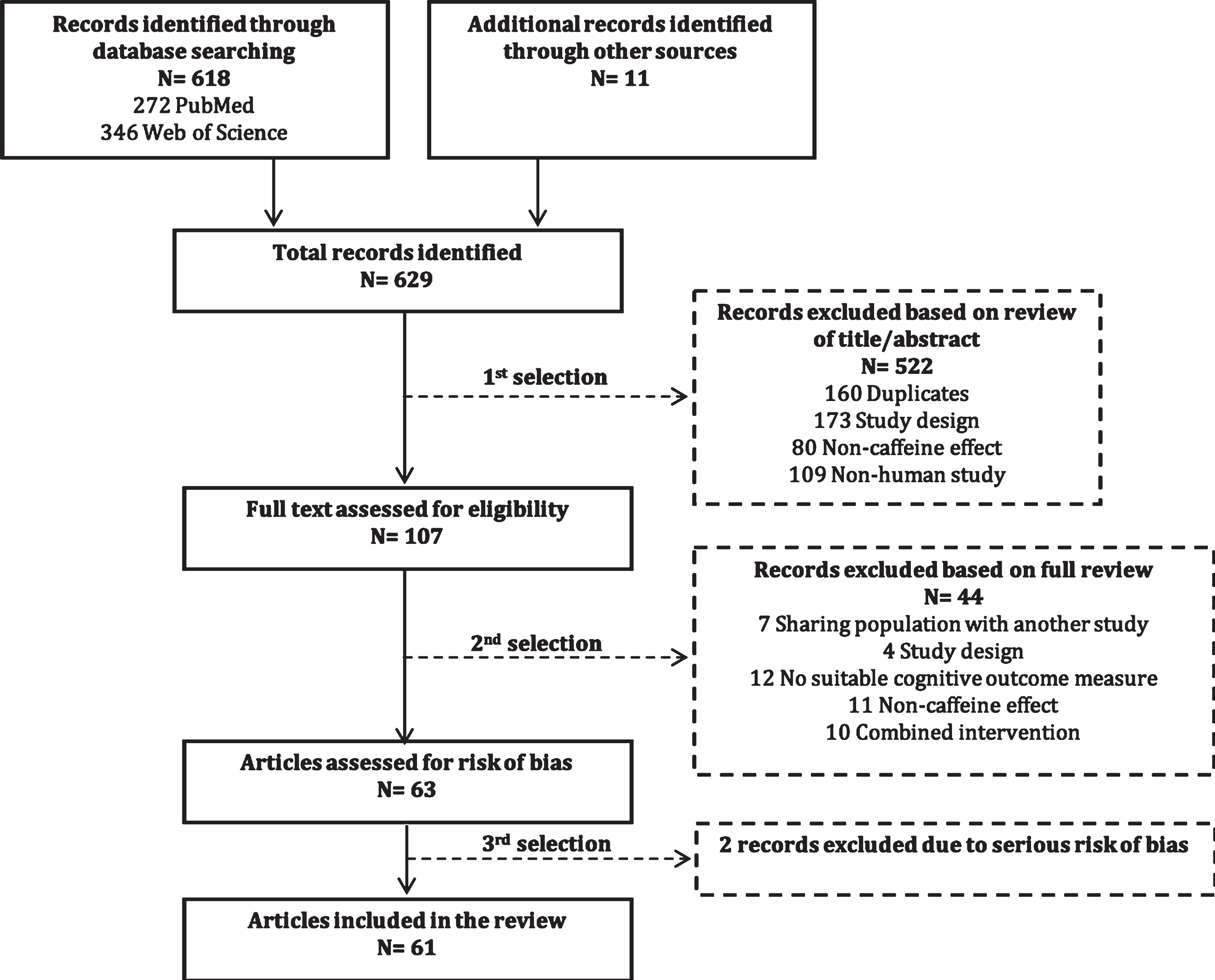
Flow diagram of identification of relevant studies.
The included studies were published between 1990 and 2020, and were executed in 24 different countries (Table 1): United States of America (n = 10) [24, 32–39], Japan (n = 9) [40–48], China (n = 8) [49–56], United Kingdom (n = 4) [57–60], Finland (n = 3) [28, 62], The Netherlands (n = 4) [62–65], Taipei (n = 3) [66–68], Canada (n = 2) [69, 70], France (n = 2) [71, 72], Portugal (n = 2) [73, 74], Singapore (n = 2) [75, 76], Italy (n = 2) [62, 77], Australia (n = 1) [78], Brazil (n = 1) [79], Germany (n = 1) [80], Iran (n = 1) [81], Ireland (n = 1) [82], Jordan (n = 1) [83], Norway (n = 1) [84], Scotland (n = 1) [85], South Korea (n = 1) [22], Spain (n = 1) [23], Sweden (n = 1) [86], and Switzerland (n = 1) [87]. One study [62] was performed in a multi-national collaboration between Finland, Italy, and the Netherlands. The final selection of articles comprised a total of 153,359 subjects (excluding subjects in the control group), which were either cognitively impaired (AD, DLB, PD, VaD, MCI, or undefined dementia) or cognitively unimpaired.
Characteristics of studies included in the review (n = 61)
MCI, mild cognitive impairment; AD, Alzheimer’s disease; PD, Parkinson’s disease; DLB, dementia with Lewy bodies, VaD, vascular dementia; RCT, randomized controlled trial; AMT, Abbreviated Mental Test; MMSE, Mini-Mental State Examination; 3MSE, Modified Mini-Mental State Examination; CERAD. Consortium to Establish a Registry for Alzheimer’s Disease; CASI, Cognitive Abilities Screening Instrument; DSST, Digit Symbol Substitution Test; CFQ, Cognitive Failures Questionnaire; MSQ, Mental Status Questionnaire; TELE, Telephone-Assessment of Cognitive State; TMSE, Tested Thai Mental State Examination; CDR, Clinical Dementia Rating; LDST, Letter-Digit Substitution Task; RAVLT, Rey Auditory Verbal Learning Test; VVLT, Visual Verbal Learning Test; SAT, Shifting Attention Test; SPMSQs, Short Portable Mental Status Questionnaires; NA, not available; NS, non-specified; HR, hazard ratio; OR, odds ratio; RR, relative risk; CI, confidence interval; y, year; mo, month; wk, week, d, day; h, hour, min, minute. Age values represent mean (±SD), unless otherwise indicated. aOverlapping or sharing population but different study design. bSmall number of overlapping population with other included study.
Risk of bias
Using the Cochrane Collaboration tool, an assessment of bias was performed for all included studies, which lead to the exclusion of two studies [30, 31] (Supplementary Table 3). Furthermore, 39/61 studies had low risk of bias and 22/61 studies had moderate risk of bias. Assessment of bias across risk of bias domains revealed predominantly moderate- to low risk of bias for six out of seven domains (Fig. 2). High risk of bias was observed on the ‘deviations from intended interventions’ domain, which could be explained by most studies employing self-reported data.
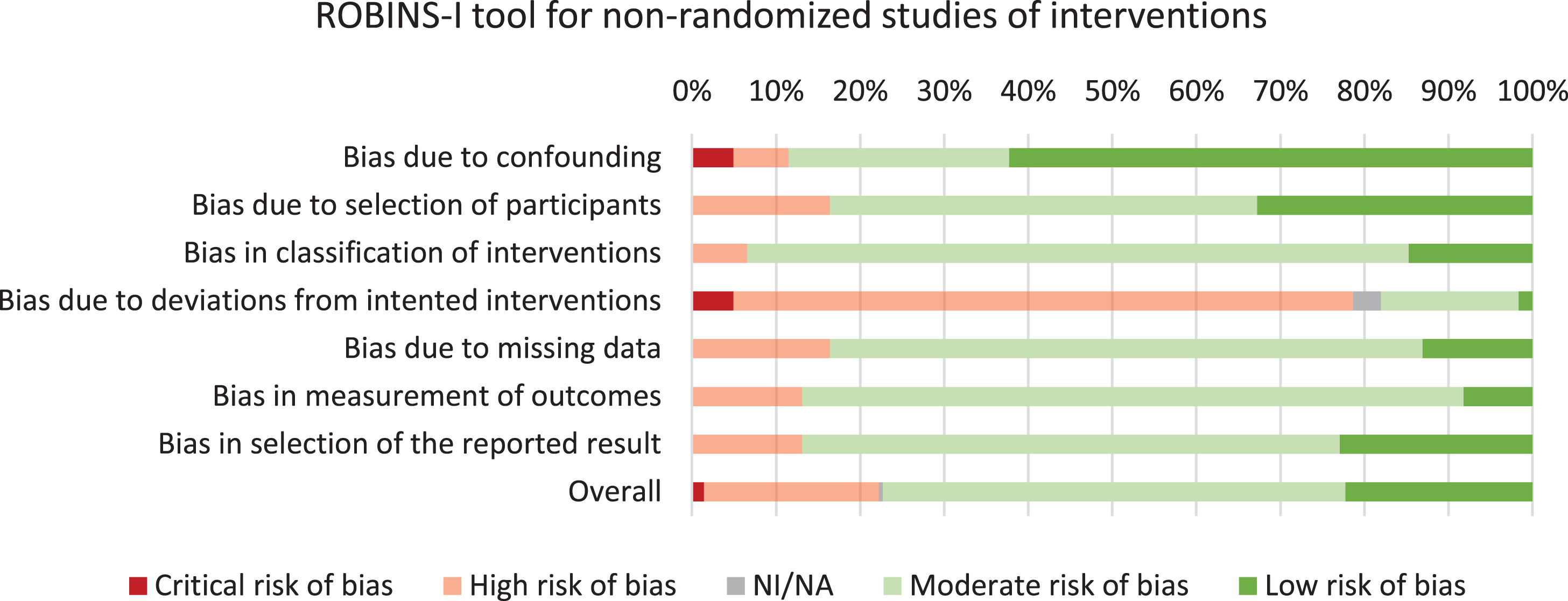
Risk of bias assessment of the included studies.
Associations between caffeine consumption and cognition
Caffeine and the risk of dementia/cognitive decline
Of the 61 articles included in this review, 57 studies with a total of 153,070 subjects, assessed the association between caffeine and the risk of dementia and/or cognitive decline (Fig. 3A, B). Within these studies, 16/57 (28%) studies including 40,707/153,070 (27%) subjects found a positive association for caffeine on the risk of dementia and/or cognitive decline that was independent of study related factors. Approximately half of the studies (30/57 (53%) studies including 71,219/153,070 (47%) subjects) reported positive results that were dependent on caffeine consumption quantity (n = 14), type of caffeine source (n = 11), sex (n = 7), age (n = 4), caffeine consumption duration (short- or long-term effects) (n = 2), and/or adjustments for covariates (n = 3). No association between caffeine and risk of dementia or cognitive decline was found in 11/57 (19%) studies including 41,144/153,070 (27%) subjects.
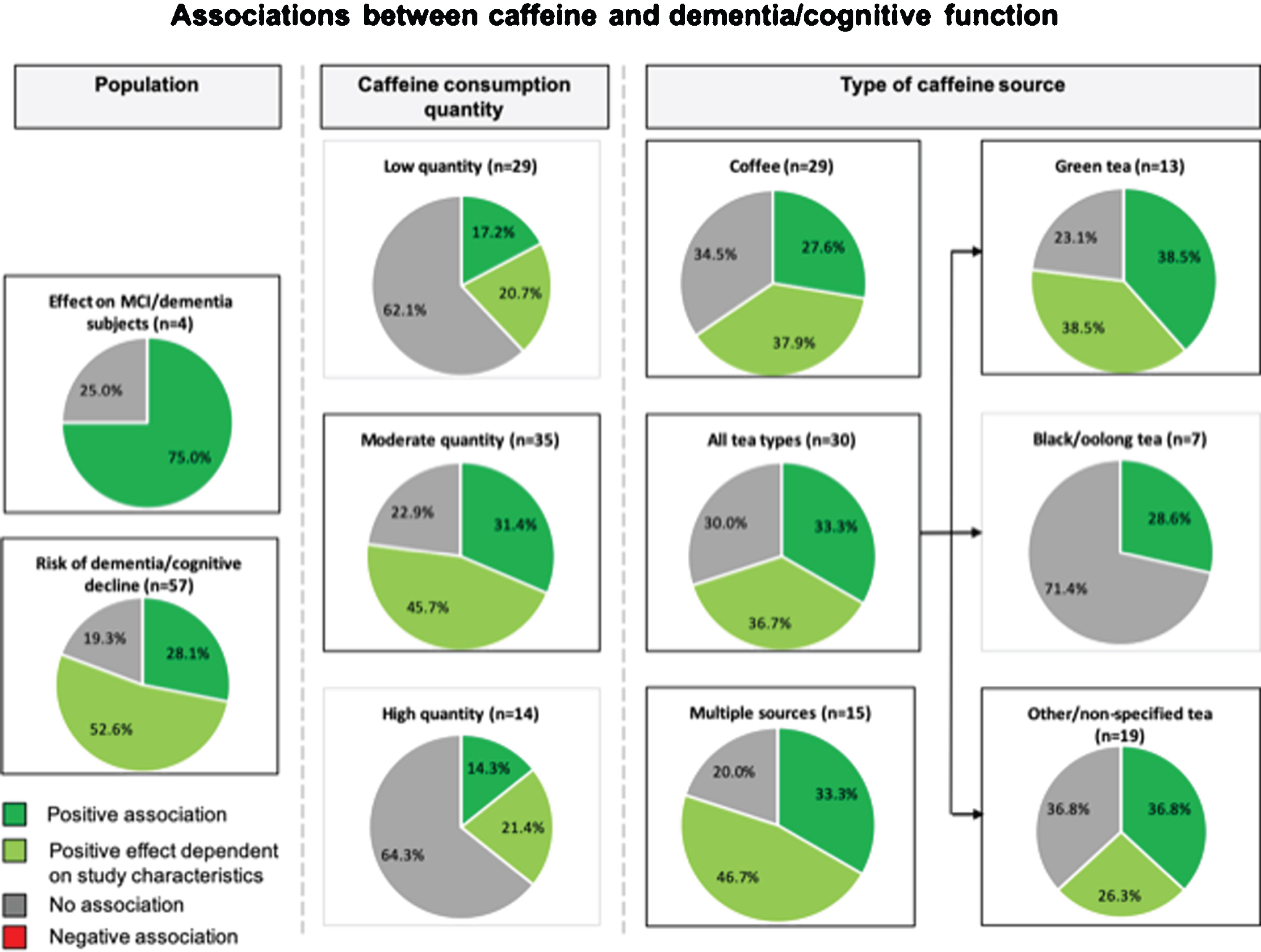
A Study outcomes for the association between caffeine and dementia and/or cognitive function. Pie charts show study outcomes based on population, caffeine consumption dosage and type of caffeine source: positive effect (darker green), positive effect dependent on study characteristics (lighter green), no effect (gray), and negative effect (red [none observed]). Outlined charts indicate a predominant positive outcome.
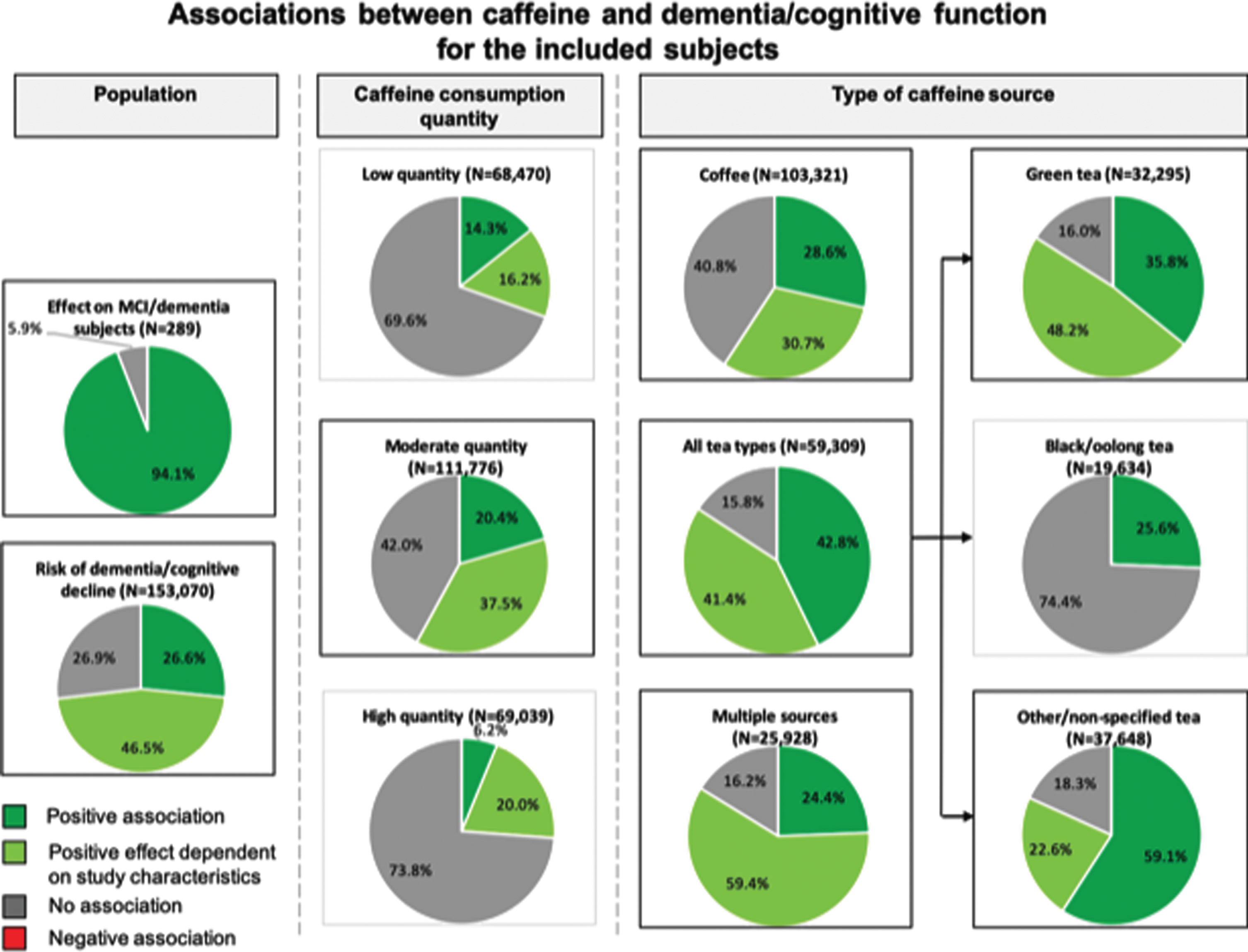
B Study outcomes for the association between caffeine and dementia and/or cognitive function of the included subjects. Pie charts show study outcomes based on population, caffeine consumption dosage and type of caffeine source: positive effect (darker green), positive effect dependent on study characteristics (lighter green), no effect (gray), and negative effect (red [none observed]). Outlined charts indicate a predominant positive outcome.
Caffeine and cognitive function in cognitively impaired individuals
Four studies [22, 41] with a total of 289 subjects assessed the influence of caffeine consumption on cognitive function in cognitively impaired individuals. Cao et al. (2012) [35] assessed concurrent plasma caffeine levels in MCI subjects over a time period of 2–4 years, and observed a reduction in progression to dementia at plasma caffeine levels >1200 ng/ml in this population. Cho et al. (2018) [22] found better global cognitive scores for individuals with PD that consumed coffee, compared to their non-coffee consuming counterparts. Ide et al. (2014) [40] and Ide et al. (2016) [41] both assessed cognitively impaired individuals with AD, VaD, or DLB that consumed green tea powder over a time period of 3 months and 12 months, respectively. Only ‘short-term’ (3 months) green tea consumption was associated with improved cognitive function or reduced progression of cognitive dysfunction.
Taken together, caffeine has a positive effect on cognition in the majority of studies (3/4 (75%) studies including 272/289 (94%) subjects) including cognitively impaired subjects.
Caffeine and study characteristics
Caffeine source
Through categorization of caffeine source that were investigated in each study, we found 29 (48%; 103,321 (67%) subjects) coffee-based studies, 30 (49%; 59,309 (39%) subjects) studies based on tea, 15 (25%; 25,928 (17%) subjects) studies based on multiple caffeinated sources, and 2 (3%; 70 (0.05%) subjects) studies based on pure caffeine (Table 2A–D). Further categorization of tea-based studies revealed 13 (21%; 32,295 (21%) subjects) studies assessing green tea, 7 (11%; 19,635 (13%) subjects) studies assessing black tea and/or oolong tea, and 19 (31%; 37,648 (25%) subjects) studies with other or non-specified tea types (Fig. 3). For the coffee-based studies, we found that 8/29 (28%) studies including 29,515/103,321 (29%) subjects reported a positive association of caffeine consumption on the risk of dementia and/or cognitive decline. Furthermore, 11/29 (38%) studies including 31,681/103,321 (31%) subjects indicated that the outcome was dependent on the quantity of coffee consumed (more positive associations with moderate quantities), sex (more positive for women), age (more positive for older age, 65–74 years), and/or the assessment of short- or long-term association (more protective in the short-term than long-term). The remaining studies on coffee (10/29 (34%); 42,125/103,321 (41%) subjects) reported no association between caffeine and risk of dementia and/or cognitive function. Two studies reported negative associations when long-term effects were assessed [64] or when examining change in habitual consumption [77], but these outcomes shifted toward a positive association when assessing short-term effects and a fixed caffeine consumption frequency and/or concentration over time, respectively.
Association between coffee-based studies (n = 29) and cognitive decline/dementia
Bold studies indicate multiple outcomes.
Association between tea-based studies (n = 30), subdivided into green tea (n = 13), black/oolong tea (n = 7), and other or non-specified tea types (n = 19) and cognitive decline/dementia
Bold studies indicate multiple outcomes.
Association between multiple caffeinated sources (n = 15) and cognitive decline/dementia
Bold studies indicate multiple outcomes.
Association between pure caffeine (n = 2) and cognitive decline/dementia
For tea-based studies, we observed 10/30 (33%) studies including 25,381/59,309 (43%) subjects with positive outcomes, 11/30 (37%) studies including 24,556/59,309 (41%) subjects with mixed outcomes dependent on consumed tea source (more positive for green tea), consumed quantity (more positive with moderate quantities), sex (mixed effects), and/or age (mixed effects), Furthermore, 9/30 (30%) studies including 9,372/59,309 (16%) subjects reported no association between tea intake and cognition. No negative associations were found for tea consumption. By classifying the different tea types, we observed proportionally more beneficial associations for green tea (39%) and other/non-specified tea (37%) compared to black/oolong tea (29%). On the other hand, we found that, across most studies (5/7 (71%) studies including 14,603/19,634 (74%) subjects), black/oolong tea was not associated with dementia/ cognitive decline.
Next, we assessed studies that included more than one caffeine source, including coffee, tea, carbonated soft drinks, energy drinks, and foods. Five out of 15 (33%) studies including 6,325/25,928 (24%) subjects reported a protective association and 3/15 (20%) studies including 4,210/25,928 (16%) reported no association between caffeine consumption and cognitive decline. Mixed results were found for 7/15 (47%) studies including 15,393/25,928 (59%) subjects: these studies revealed a dependency of study outcomes according to consumed quantity of caffe-ine, sex, age, and/or covariates in the models. More positive outcomes were found for women compared to men [71, 74], and more positive associations were found for a moderate or higher caffeine quantity (>62mg/d [74], >200 mg/d [39], >300 mg/d [71]). We also found that in studies with mixed caffeine sources, more positive effects were found at ages >70 years, and particularly over 90 years. We found inconclusive findings for the impact of univariate-/basic adjustments or multiple adjustments on cognitive function [72, 85].
Finally, two studies assessed the association of pure caffeine consumption: Konishi et al. (2018) reported better executive function scores, while Walters & Lesk (2016) reported no significant association on cognitive tests.
Our examination of effects in coffee, tea, mixed sources, and pure caffeine-based studies demonstrates that the study outcomes are highly dependent on the caffeine source. Among these caffeine sources, only black/oolong tea seems not to have a protective effect for dementia/cognitive decline. In addition, our data reveal that evidence of a deleterious effect of caffeine consumption on cognitive function is limited.
Caffeine consumption quantity
We assessed the associations between caffeine qu-antity based on the frequency and/or dosage. Of the 61 studies, 48 provided sufficient information to al-low assessment of these associations (Table 3, Fig. 3). Based on pre-specified criteria, the studies were divided into three quantity categories: low caffeine consumption (<100 mg/d) (n = 29, N = 68,470), moderate caffeine consumption (100–400 mg/d) (n = 35, N = 111,776), and high caffeine consumption (>400 mg/d) (n = 14, N = 69,039). For studies with low- and high quantities of caffeine consumption, we mainly found no impact on risk of dementia or cognitive function: positive associations were only observed for 11/29 (38%) and 5/14 (36%) studies respectively. Interestingly, for moderate caffeine consumption, we mainly found beneficial associations with cognitive function (27/35 (77%) studies, that were either dependent (16/35 (46%) studies) or independent of type of caffeine source and/or other study characteristics (11/35 (31%) studies). By further stratifying studies using moderate consumption according to caffeine sources (Table 3), we found that especially consumption of green tea may reduce the risk of dementia and cognitive decline.
Association between caffeine consumption quantity and cognitive decline/dementia
aCategorization in this group due to different categories used in the study.
Confounding factors
Most studies adjusted for age and sex, and in a subset of studies additional model adjustments were made for factors like hypertension, diabetes mellitus, hyperlipidemia, education, APOE genotype, smoking, alcohol, physical activities, body mass index (BMI), socioeconomic status, and global cognition (MMSE). Some studies reported an impact of confounding factors on outcomes.
For seven studies [32, 74], outcomes were dependent on sex. These studies reported that beneficial associations are predominantly found in women (5/7 studies). In line with these findings, two studies with only female participants [37, 72] reported positive associations and two out of three studies with only male participants [24, 62] reported no associations.
Four studies indicated that positive associations are dependent on age. These studies reported positive associations between caffeine consumption and dementia and/or cognitive function at older ages (65–74 years versus 35–64 years [79], >70 years versus <70 years [33], 90 years versus 70 years [39]). However, two other studies indicated the reverse, an effect at younger age (>60 years versus >70 years [54]) or that effects were particularly found at ages <70 years old [55].
Furthermore, Mirza et al. (2014) [64] and Araújo et al. (2016) [63] found different outcomes depending on the time of follow-up. Short-term follow-up (within 4 years) revealed positive associations, while the association was negative at long-term follow-up (>4 years) [64] and absent in another study implementing a long-term follow-up (5.5 years) [63].
Corley et al. (2010) [85] observed protective associations between caffeine and cognitive function when adjusting for age and sex, but when additional adjustments were made for socioeconomic status or social class and (childhood) IQ, the association did not reach the threshold for statistical significance. Similar results were observed by Iranpour et al. (2020) [81], who reported a positive association in a univariate model but no association in models where adjustments for factors like sex, age, race/ethnicity, education, and marital status, or self-rated health, disease history, and depression were made. Vercambre et al. (2013) [72], on the other hand, only found a positive association when adjusting for alcohol consumption, physical activity, BMI, and smoking, but not when only adjusting for age, education, and diet. Moreover, this study found a more pronounced positive association with caffeine when it was supplemented with vitamin B.
DISCUSSION
In this systematic review, we assessed the association between caffeine and 1) the risk of dementia and/or cognitive decline and 2) cognitive function in individuals with impaired cognition (i.e., MCI or dementia). The number of studies showing positive associations (dependent or independent of study cha-racteristics) was 46/57 (81%) including 111,926/153,070 (73%) subjects, indicating that caffeine has a beneficial effect on the risk of dementia/cognitive decline. We also found more positive results (3/4 (75%) studies including 272/289 (94%) subjects) for studies that included subjects with MCI, or any type of dementia, indicating that caffeine also has a beneficial effect in cognitively impaired subjects. Furthermore, we observed that various study characteristics affect the reported associations of caffeine such that moderate consumption seems to be more beneficial than low- or high quantities, and coffee, green- and other/non-specified tea, and multiple caffeinated sources are more beneficial than other caffeine sources like black/oolong tea. Effects were also found to be more pronounced in women compared to men, and many studies reported mixed outcomes based on other factors like age and follow-up time. Across all studies, we observed only two studies with a negative effect, suggesting that caffeine is unlikely to negatively affect cognition or dementia risk. This review highlights that dietary factors may influence risk of cognitive decline and dementia, and may also aid the future development of caffeine-based intervention studies, which might serve as a cost-effective alternative or add-on to other non-pharmacological or pharmacological treatments against cognitive decline and dementia (e.g., physical activity [88]).
Potential mechanisms
Results from this review suggest that caffeine effects are dependent on the caffeine source and quantity. Several explanations exist for this outcome. First, different types of caffeine sources contain different levels of caffeine [29], and low dosages might be inadequate to convey positive effects while with excessive dosages the negative effects (e.g., anxiety) might outweigh the positive effects. There might also be individual variability in the physiological response to caffeine (e.g., due to genetic factors that influence responsiveness of A2A receptors), which would result in differential effects of the same dose of caffeine across individuals [14, 90]. Furthermore, physiological effects of other substances than caffeine that are contained within the caffeine source (e.g., coffee) may influence or strengthen the caff-eine response, by affecting the kinetics of caffeine in the body and the response of adenosine receptors, or have a caffeine independent effect that influen-ces cognitive performance [91]. For example, various sources of caffeine contain antioxidants, which have been found to play a role in protecting against oxi-dative stress, and may thereby help in preventing cognitive deterioration [92]. Coffee displays antioxidative effects through chlorogenic acid and poly-phenols [93]. Tea displays antioxidative effects through tea catechins and theaflavins, and green tea exhibits higher antioxidative effects than black or oolong tea [94]. Varying antioxidative mechanisms or degrees of antioxidative effects might contribute to the differences in study effects according to caf-feine sources observed in this report (i.e., more effects in green compared to black/oolong tea). However, further research is needed on the effect of antioxidants as studies have also reported no effect of antioxidants on cognitive function, but rather on mood [95]. Caffeine may also lead to better cognitive function and memory indirectly through an increase in alertness and wakefulness [12], and by influencing sleep and impulsivity [14, 96].
Caffeine has also been found to influence neural and vascular activity such as vasoconstriction and reduction in cerebral blood flow (CBF). Reduction in CBF leads to an increased oxygen extraction from the blood to cerebral structures in the brain [97], which, in turn, enhances cognitive performance. It seems possible that a sufficient quantity must be ingested in order to produce this effect. On the other hand, excessive caffeine consumption could lead to (acute) caffeine overdose, which could convey negative effects such as reactive oxygen species formation [98], that outweigh the positive, or indirect negative symptoms that could influence cognitive function such as restlessness, anxiety, agitation, insomnia, and headache [16].
This review revealed incongruent outcomes for other confounding factors such as sex, age, and follow-up time. It seems that caffeine consumption is particularly beneficial for cognitive function in women in comparison with men. In general, inconsi-stent results for women and men might be explained through sex-based biological variations such as tes-tosterone and estrogen hormone levels [99]. Furthermore, four studies reported an outcome that was dependent on age, but it remains to be determined at what age caffeine has the most beneficial effect as some studies reported greater effects in older subjects, while others reported greater effects in younger subjects. Follow-up time was also found to influence outcomes in two studies. These studies both reported beneficial associations at a short follow-up time, while no effects were observed at a long-term follow up. This suggests that the beneficial effects of caffeine might be temporary.
Strengths and limitations
The main strength is that we performed a systematic review and assessed all available studies, regardless of study design. Thereby, we were able to include more studies than have previously been in-cluded in other reviews and meta-analyses [100–103]. However, there are also limitations that need to be considered when interpreting this review. First of all, it is important to highlight that, in the second-ary analysis on cognitively impaired individuals, we were able to assess only four studies, and that these studies included individuals with different types of cognitive impairments, various caffeine sources and different study designs. Also, one out of four studies included patients with PD, for which the degrading underlying mechanisms are different compared to patients with dementia or MCI. Secondly, our app-roach of providing this systematic review did not allow us to perform formal statistical analyses to assess the effects of caffeine quantitatively, or stati-stically assess modifying effects. This lack of quantitative assessments means our findings were based exclusively on overall study outcomes. Thirdly, our interpretation of the included studies relied on data provided in the paper, and we did not contact the authors to provide additional information because of the wide inclusion timeframe of this review (1990–2020). As a result, not all studies could be included when assessing study characteristics. For example, accurate information on caffeine quantity was not al-ways provided. Furthermore, many studies employed self-reported caffeine consumption data resulting in a high risk of bias due to deviations from the intended intervention. Finally, information on reporting of funding sources and conflicts of interests were not considered as possible confounders in the analyses.
Conclusion
Our findings indicate that caffeine beneficially affects cognitive function and risk of dementia and that this effect is dependent on the type of caffeine source (e.g., more effects for coffee and green tea), quantity (more effects with moderate quantities), and sex (more effects in female subjects). Furthermore, we found that other factors such as age and follow-up time might influence effects and it is important for future studies to examine, and account for, these confounders. Ideally, future investigation should implement a randomized-controlled trial design, which would allow for quantitative assessme-nts of effects across studies. Future studies including various dosage levels could additionally help to extend our findings regarding the most beneficial caffeine dosage by accurately determining the optimal caffeine quantity to effect cognitive decline and risk of dementia. Furthermore, it would be interesting to map genetic factors that influence response to caffeine (e.g., A2A receptor haplotype) in future studies, as differences in responsiveness to caffeine could influence effects of caffeine on cognition. These in-sights may help in tailoring cost-effective lifestyle interventions, and possibly even aid in the development of pharmacological interventions that combat cognitive decline and dementia.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/20-1069).