
Abstract
Background:
A key focus for dementia risk-reduction is the prevention of socio-demographic, lifestyle, and nutritional risk factors. High sodium intake is associated with hypertension and cardiovascular disease (both are linked to dementia), generating numerous recommendations for salt reduction to improve cardiovascular health.
Objective:
This systematic review aimed to assess, in middle- and older-aged people, the relationship between dietary sodium intake and cognitive outcomes including cognitive function, risk of cognitive decline, or dementia.
Methods:
Six databases (PubMed, EMBASE, CINAHL, Psych info, Web of Science, and Cochrane Library) were searched from inception to 1 March 2020. Data extraction included information on study design, population characteristics, sodium reduction strategy (trials) or assessment of dietary sodium intake (observational studies), measurement of cognitive function or dementia, and summary of main results. Risk-of-bias assessments were performed using the National Heart, Lung, and Blood Institute (NHLBI) assessment tool.
Results:
Fifteen studies met the inclusion criteria including one clinical trial, six cohorts, and eight cross-sectional studies. Studies reported mixed associations between sodium levels and cognition. Results from the only clinical trial showed that a lower sodium intake was associated with improved cognition over six months. In analysis restricted to only high-quality studies, three out of four studies found that higher sodium intake was associated with impaired cognitive function.
Conclusion:
There is some evidence that high salt intake is associated with poor cognition. However, findings are mixed, likely due to poor methodological quality, and heterogeneous dietary, analytical, and cognitive assessment methods and design of the studies. Reduced sodium intake may be a potential target for intervention. High quality prospective studies and clinical trials are needed.
INTRODUCTION
Dementia is a severe condition characterized by cognitive deficits and loss of independence. It is associated with a wide range of poor outcomes including increased frailty and mortality [1–4]. Aging is one of the most important risk factors for cognitive decline and dementia and the rapid shifts in global demographic trends are contributing to the projected increase in dementia cases over the next decades [5].
Currently, dementia is incurable and pharmacological treatments for symptom management are modest [6]. There have been numerous calls for research directed at the identification and testing of preventative strategies to minimize, or arrest the onset of cognitive decline and reduce the rate of conversion to clinical dementia in high risk individuals [7]. Observational studies suggests that in some cases the pathological processes underlying dementia might be influenced by dietary components [8]. Excessive consumption of dietary sodium (or salt) has been associated with adverse health outcomes [9, 10], including hypertension, stroke, and coronary heart disease [11, 12]. A sustained drop in salt intake of about 4.0 g/day could result in a 4.2 mmHg reduction in blood pressure [15]. Hypertension is a known risk factor for dementia for people in midlife to late life [11]. While there is consensus on the need to reduce sodium consumption for the prevention and treatment of hypertension [12, 13], the evidence on an association between sodium consumption, cognitive impairment, and dementia risk remains limited.
Animal studies have demonstrated that high dietary salt is associated with neurotoxicity (increased amyloid aggregates) [14] and effects systemic and cerebral blood vessels [15, 16], all of which have been linked to cognitive impairment and dementia. More recent findings in animal studies have also suggested that the effect of salt on cognition may occur via a gut-mediated pathway [17]. A high sodium diet in mice leads to an adaptive immune response in the gut which then reduces blood flow to the brain, and promotes neurovascular and cognitive impairment [17]. Therefore, salt reduction may reduce dementia risk via its benefits on cardio-metabolic health and inflammation, both of which have been found to contribute to dementia risk [18–20]. In humans, healthy dietary patterns with low sodium levels, such as the Mediterranean diet (MD) [21, 22] or the Dietary Approach to Stop Hypertension (DASH) diet [23, 24], have been associated with better cognitive function.
The aim of this systematic review was to summarize the current evidence on the association between dietary sodium intake, cognitive function and dementia risk. The findings will be important for informing the development of new intervention and prevention strategies targeting cognitive function. Indeed, being able to reduce the global burden of disease associated with impaired cognitive function and dementia will have significant personal, social and economic consequences.
METHODS
Protocol registration
This review was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses statement [25]. The review protocol was registered on PROSPERO (CRD4201914632).
Search strategies and study selection
A systematic search for eligible publications was performed in six electronic databases (Pubmed, Embase, CINAHL, Psych info, Web of Science, and Cochrane Library) from inception to 1 March 2020. The search terms were salt, sodium, natrium, intake, consumption, feeding, old age, elderly, aged, geriatric, people, adults, population, cognitive, memory, mental, impairment, function, decline, dementia, Alzheimer. The detailed search strategy is described in Supplementary Table 1. Titles and abstracts of the identified studies were screened for inclusion by two authors (KHY and YCS). Studies that were not relevant were excluded. Full papers were sought for all studies meeting the inclusion criteria and final selections were made by two authors (DM and KHY). Articles were included if they were 1) human studies of middle and older aged adults (aged 45 years and above); 2) original research articles published in peer reviewed scientific journals; and, 3) studies presenting data on cognition and sodium or salt intake with the following study designs: prospective cohorts, cross-sectional studies, clinical trials and case control studies. There were no restrictions on baseline cognitive function. Only English articles were considered. Studies were excluded if there was insufficient information to allow for a critical evaluation of the strength and direction of the results. Specifically, eligible studies had to include information on measurement of dietary sodium or salt intake, cognitive function, and/or dementia and report details on the association between dietary sodium intake with dementia risk and cognitive decline.
Data extraction and quality assessment
Data was extracted by one investigator (KHY)using a standardized electronic template. Data entries were then independently checked for completeness and inconsistencies by a second investigator (DM). Any discrepancies were resolved by consensus. Extracted data included study design, country, study population characteristics, sample size, sodium or salt intake classification, details of dementia status and cognitive function, methods of assessment of sodium or salt intake, cognitive function or dementia risk, and summary measures of the association between salt or sodium intake with risk of dementia, cognitive decline, or cognitive impairment. Further details of potential confounders including age, sex, race, education, body mass index (BMI), health-related comorbidities, physical activity, alcohol intake, and total energy intake were also recorded. In this paper, we have considered the terms salt and sodium as equivalent. However, when extracting the data, the specific measurement of salt or sodium intake is reported as in the original manuscript.
Risk of bias assessments were performed using the National Heart, Lung, and Blood Institute (NHLBI) assessment tool [26]. Studies were rated as “good” (low risk of bias), “fair” (intermediate risk of bias), or “poor” (high risk of bias). Quality was assessed by one reviewer (KHY) and double checked by a second reviewer (YCS). Disagreements were resolved by consensus or by consulting a third reviewer (DM).
Synthesis of results
Due to heterogeneity in study design and large differences in the assessment of salt/sodium intake and cognitive function, it was not possible to pool results in a meta-analysis. Therefore, we have presented the results stratified by cognitive domains (including global cognition, memory, executive function, processing speed and other). The results for the association between sodium or salt intake with mild cognitive impairment (MCI) or dementia are also reported separately.
RESULTS
Study selection
From the electronic search, 725 articles were identified; of which 156 were duplicates and therefore removed. After title and abstract screening 542 papers were excluded leaving 27 for full text review. From the full text review, 15 studies fulfilled the inclusion criteria and were included in the review (see Fig. 1).
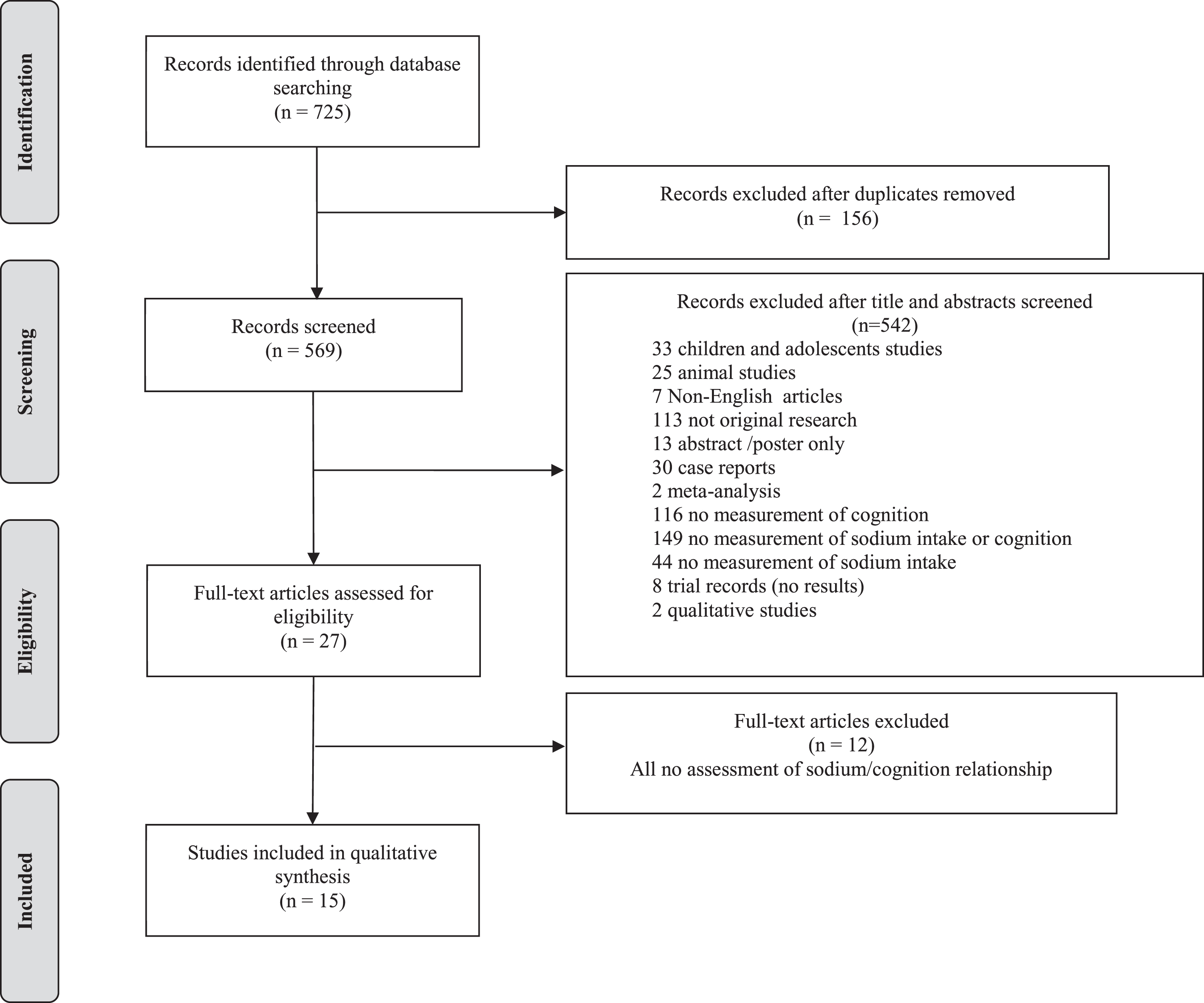
Flow diagram of study selection.
Study characteristics
This review includes data from one clinical trial [27], six longitudinal cohort studies [28–33] (of which three studies only reported results of cross-sectional analyses [30, 33]) and eight cross-sectional studies [34–41] (Table 1). Six of the studies were conducted in the United States of America (USA) [27–29, 39], two studies were conducted in Australia [33, 36], and one study each was conducted in Canada [30], Turkey [34], Korea [37], Poland [35], Scotland [38], Ireland [40], and China [41]. The only clinical trial included 160 participants who had subjective memory complaints, objective cognitive impairment (as assessed with the Montreal Cognitive Assessment [MoCA]), and at least one cardiovascular risk factor [27]. Mean age was 65.4 years (SD = 6.8) with a follow-up time of six months. The six [28–33] cohort studies had sample sizes ranging from 1,194 [29] to 6,426 [28] participants. Age ranged from 40 to 96 (only one study [32] included participants aged 40 years and above, with the mean age of participants higher than 45 years old). Follow-up time ranged from three to 36 years. The remaining eight [34–41] cross-sectional studies had sample sizes ranging from 44 [40] to 402 [35] participants with ages ranging from 50 to 85 years. Thirteen studies included both men and women, with two studies only including post-menopausal women [28, 35].
Characteristics of reviewed studies
3MS, The Modified Mini-Mental State Test; AD, Alzheimer’s disease; DASH, Dietary Approaches to Stop Hypertension diet; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders (fourth edition); FFQ, Food frequency questionnaire; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; PCA, Principal Component Analysis; SD, standard deviation
A total of 55 independent analyses examining the association between sodium or salt intake and cognitive outcomes were extracted from the 15 studies; out of which 26 analyses adjusted the results for confounding factors.
Risk of bias/Quality assessment
Based on the NIHLB assessment tool four studies were rated as “good” [27–30], five were classified as “fair” [31–34, 37], and six studies were rated as “poor” [35, 38–41]. The main issues across the studies included poorly defined study populations, non-reporting of participating rate, large proportion of missing data, and no adjustment for confounding factors.
See Supplementary Tables 2 and 3 for the rating of each study.
Assessment of sodium and salt intake
Sodium or salt intake was assessed using a wide variety of methods and four studies used more than one assessment of sodium intake [29–31, 34]. Seven studies [27–31, 40] assessed sodium or salt intake with food frequency questionnaires (FFQs), five studies [27, 39] used food diaries, two studies [28, 34] used 24-hour urinary sodium excretion, two studies used single self-reported salt-intake questions [32, 41], and one study used two self-reported salt-intake questions [33]. Two studies [29, 37] used sodium/potassium intake ratios (Na/K) to assess sodium intake.
Assessment of cognitive function, MCI, and dementia
There were large differences in how cognitive function was assessed. The most frequently used tests included the Mini-Mental State Examination (MMSE) (six studies [31, 40]), modified Mini-Mental State Examination (3MS, two studies [29, 30]), Verbal Fluency Test (two studies [31, 36]), and the Trail Making Test (two studies [27, 36]). Only one study used the Telephone Interview for Cognitive Status Modified (TICS-m) [41]. Three studies combined cognitive measurements to derive composite scores of cognitive performance [27, 38]. Seven studies used more than one measure of cognition [27, 35–38].
Two studies [28, 32] assessed clinical status, including MCI or dementia (all-cause). Dementia was diagnosed using the criteria from the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV). MCI was diagnosed if the participant scored in the 10th or lower percentile in at least one area of cognitive function on modified neuropsychological tests established by the Consortium to Establish a Registry for Alzheimer’s Disease or if the participant was reported to suffer from some functional impairment but still performed well in basic activities of daily living as reported by a reliable informant [28]. A study by Li et al. [32] additionally used the criteria from National Institute of Neurological Disorders and Stroke and the Association Internationale pour la Recherche et l’Enseignementen Neurosciences (NINDS–AIREN) for the diagnosis of vascular dementia.
Global cognition
Eight studies [29–31, 39–41], with sample sizes ranging from 44 [35] to 1,262 [30], reported associations between sodium intake and global cognitive function measured using single tests including the MMSE, 3MS, or the TICS-m (see Table 2). Only one study was analyzed prospectively [29], the others were cross-sectional [31, 39–41]. Overall, the results were mixed. In studies using the MMSE or 3MS, four [29, 40] showed that higher dietary sodium was associated with poor global cognitive function, one study showed that lower dietary sodium preference was associated with better cognitive function [41], and one study showed that higher sodium was associated with better MMSE scores [31]. The remaining two studies reported no associations [37, 39].
The only study utilizing the TICS-m reported no association in the total study sample and mixed associations when the analyses were stratified by sex [33]. Men who reported they “usually” add salt during cooking had poorer cognitive function than men who reported “never”. In contrast, women who reported they “sometimes” add salt after cooking had better cognitive function than women who reported “never”. Two studies [35, 38] using a composite of tests to derive a global cognition score both reported no association between sodium intake and cognitive function (see Table 2).
The association between sodium intake and global cognition (measured by screening tools)
3MS, The Modified Mini-Mental State Test; ANOVA, Analysis of Variance; BMI, body mass index; CI, cognitive impairment; CVD, cardiovascular disease; GEE, generalized estimating equation; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; Na, sodium; Na/K, sodium/potassium ratio; r, correlation coefficient; SBP, systolic blood pressure; SD, standard deviation; OR, odds ratio, C-MMSE = Chinese MMSE; TICS = Telephone Interview for Cognitive Status modified.
Four studies [27–30] were rated as “good” quality, five studies [31–34, 37] were rated as “fair”, and six studies [35, 38–41] were rated as “poor”. When restricting the analysis to high quality studies only (n = 2 studies [29, 30]) the results were consistent; Nowak et al. [29] showed that a higher Na/K ratio was associated with cognitive decline (OR = 2.02, 95% CI: 1.01–4.03) and Fiocco et al. [30] showed that higher sodium intake was associated with cognitive decline in older subjects with low physical activity.
Memory
Four cross-sectional studies, with sample sizes ranging from 44 to 189, reported associations between sodium intake and memory [35–38] (see Table 3). Eleven different memory tests were used and two studies [35, 38] created composite scores including more than one test. One study [37] was rated as “fair” while the remaining three studies [35, 38] were rated as “poor” quality. The only statistically significant association between sodium intake and memory function was found in the study conducted by Hwang and Kim [37]. This study analyzed the relationship between Na/K quartiles with memory function in heart failure patients and observed that the lowest and highest quartiles of Na/K ratio were associated with poorer memory scores compared to the second and third quartiles of Na/K ratio.
Association between sodium intake and memory
ANOVA, Analysis of Variance; FFQ, Food frequency questionnaire; M, mean; Na/K, sodium/potassium ratio; r, correlation coefficient; SD, standard deviation.
Executive function
Five studies [27, 35–37] with sample sizes ranging from 44 to 925 reported associations between sodium intake and executive function (see Table 4). Twelve types of tests were used to assess executive function with the Trail Making Test the most commonly used (n = 3 studies [27, 36]). Only two studies reported significant associations between sodium and executive function, but the results were mixed [27, 31]. The clinical trial, which had a low risk of bias, reported that a lower sodium intake was associated with improved executive function measured using a neuropsychological battery including the Trail Making Test [27]. In contrast, the cross-sectional study by Rush et al. [31], which was rated as fair, reported that higher sodium intake was associated with better performance on the Trail Making Test. The remaining three cross-sectional studies reported no association [35–37].
Association between sodium intake and executive function
ANOVA, Analysis of Variance; CVD, cardiovascular diseases; FFQ, Food frequency questionnaire; GLM, generalized linear model; M, mean; MoCA, Montreal Cognitive Assessment; Na/K, sodium/potassium ratio; r, correlation coefficient; SD, standard deviation.
Processing speed
Only two cross-sectional studies [35, 38], with sample sizes ranging from 189 to 402, examined associations between sodium intake and processing speed using different cognitive assessments. No significant association was reported in either study (see Table 5). Both studies were rated as “poor” quality.
Association between sodium intake and processing speed
r, correlation coefficient.
Dementia and MCI
Only two prospective studies [28, 32] reported associations between sodium intake with risk of MCI or dementia (see Table 6). The follow-up period for each study was a median of 9.1 years [28] and 36 years [32]. The first study with low bias of risk [28] stratified participants (n = 6426) by different levels of sodium intake (FFQ sodium level adjusted for 24 h urinary levels).They concluded that for women in the sodium intakes tratum of 2,300 mg to 3000 mg per day, hypertension was associated with greater risk of probable dementia/MCI in (HR = 1.28, 95% CI: 1.08–1.51) compared to non-hypertension. The study also concluded that for women in this stratum of sodium intake, those on antihypertensive medication were at a higher risk of probable dementia or MCI compared to those not on antihypertensive medication (HR = 1.25, 95% CI:1.06–1.48).These associations were not significant in other two strata of sodium intake (less than 2300 mg/day and more than 3000 mg/day). Formal tests of interaction were also not significant. The second study [32] found no significant association between sodium intake and risk of incident dementia (OR = 1.64, 95% CI: 0.95–2.83; n = 2461).
Association between sodium intake and diagnosis of dementia or MCI
3MS, The Modified Mini-Mental State Test; CI, cognitive impairment; CVD, cardiovascular; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders (fourth edition); HPT, hypertension; HR, hazards ratio; OR, odds ratio; MCI, mild cognitive impairment; Prob Dem, probable dementia; WHI, Women’s Health Initiative (study).
Other cognitive domains
Additional cognitive domains were tested in three cross-sectional studies included “general” [38], “neurocognition index” [35],“attention” [35], “cognitive flexibility” [35], “psychomotor speed” [35], “reaction time” [35], and “language” [36] (Table 7). Overall, studies had a small sample size (ranging from 47 [36] to 189 [38] participants) and were of low quality. None reported significant associations between sodium intake and performance on these cognitive domains (see Table 7).
Association between sodium intake and other cognitive domains
r, correlation coefficient.
DISCUSSION
This is the first review, to our knowledge, to synthesize the current evidence on the association between sodium intake and cognitive outcomes. In total, fifteen studies were identified of which over 60% (n = 10 studies [27–31, 41]) reported significant associations. However, mixed results were found regarding whether dietary sodium intake is associated with cognitive function. Of the eight studies with significant results, five [27, 41] reported a positive association, one reported a negative association [31], one reported a mixed association [33], one reported a j-shaped association [37], and the remaining study reported that moderate sodium intake is associated with cognitive impairment [28]. Even though the overall evidence was mixed, higher quality studies generally reported that lower sodium intake was associated with better cognitive function [27, 30]. A positive association between high sodium intake and cognitive decline points to the possible role of low sodium diets to prevent cognitive decline. However, a lower sodium intake might also be associated with poor cognitive performance which adds to the complexity of this topic.
With regard to specific cognitive domains, there appeared to be some evidence that high salt intake is associated with poor global cognitive function assessed using the MMSE/3MS. Indeed, four studies [29, 40] reported a significant positive association, one study [31] reported a significant negative association, and two studies [37, 39] reported no association. In contrast, the results for memory, executive function and processing speed, while mixed, generally reported no significant association. The three studies with significant associations that assessed global cognition were longitudinal in nature [29, 30] and/or had large sample sizes (n = 1194 [29], n = 1262 [30], n = 925 [31]). The remaining two studies with significant associations that assessed global cognition were cross-sectional with small sample sizes (n = 119 [34], n = 44 [40]), but had significant risk-of-bias issues. Of the six studies that examined memory [35–38], executive functioning [27, 35–37], and processing speed [35, 38], only three studies reported significant associations; one study for memory [37] and two studies for executive functioning [27, 31].
Generally, the studies with significant associations were of low to intermediate risk-of-bias. These studies also ranged from health community living adults to more specific populations of higher risk groups. For instance, Hwang et al.’s [37] study population comprised of heart failure patients which can be considered a higher risk group due to the cardio-metabolic risk being associated with dementia [18–20]. This increases the chances of detecting a link between sodium intake and cognitive function. Even though the sample size in Hwang et al.’s study was small (n = 91), statistically significant results were still found in sodium intake’s relationship with memory. On the other hand, even if the study population was of higher-risk, the limited spectrum of cognitive function observed in a cross-sectional setting would limit the chances of observing any significant association. For example, in Bojar et al. [35], even though participants were higher-risk (e.g., post-menopausal women; defined as high risk given that a decline in estrogen has been previously linked to increased risk of cardiovascular diseases and dementia [42, 43]), the results were null. This is likely because the study only included participants on the higher spectrum of cognitive performance (i.e., MoCA≥26) and was cross-sectional. More high-quality longitudinal studies in both healthy adults and high-risk groups across wider cognitive spectrums are needed to illuminate and test the mechanism of the sodium-cognition continuum.
With regard to incident MCI and dementia, the results were mixed. In one study [28], moderate sodium intake in hypertensive post-menopausal women was found to be associated with an increased risk of dementia (either alone or combined with MCI). In another study, that focused on incident dementia in healthy older adults, no association was found [32]. The differing results may be due to study population characteristics. For Haring et al. [28], the study population comprised of only post-menopausal women, and focused on hypertension as the main exposure of interest. Li et al. [32] on the other hand, focused on healthy men and women with sodium intake as the exposure of interest.
The methods used for the analysis of the studies may also have contributed to the differing results. Haring et al. [28] performed separate analysis for each strata of sodium levels, instead of conducting analyses in the whole sample, reducing the statistical power. In fact, to assess the association of sodium and cognitive decline, it would have been more appropriate to use the sodium intake levels as a predictor variable. In Li et al. [32], the follow up time was for a sufficiently long period of time (36 years). However, the imprecise measurement of sodium intake with just a single question (yes/no to whether the participant was on a low-salt diet) at a single point in time, may have affected the results. Analyses of data from prospective studies with accurate assessments of dietary sodium intake over time cognitive status and dementia incidence are needed to confirm whether excessive sodium consumption is associated with impaired cognition and dementia risk.
To a certain extent, the findings from this review support that higher sodium intake have bearings on the cognitive health of middle and older aged individuals. The missing link in all the studies included in this review would be the inclusion of factors that may allude to the different mechanisms of how sodium intake affects cognition. So far, most studies that adjusted for confounders typically targeted factors associated with cardiometabolic health and inflammation such as stroke, diabetes, hypertension or blood pressure readings, and BMI. Given the potential mechanism via a gut mediated pathway [17], it would be interesting to observe the effects of sodium intake and its interaction with cardiometabolic health and inflammation (rather than just controlling for confounding) to also tease out the effects (if any) of the gut mediated pathway hypothesis.
As the range of cognitive assessments is wide and largely context dependent, more objective indications of cognitive function or decline should be considered. Future studies can include cerebrospinal fluid, neuroimaging, or blood biomarkers of dementia and cognitive decline. There are robust biomarkers of dementia which are known to correlate with pathological progression (especially in the case of Alzheimer’s dementia) [44]. For example amyloid-β levels and hippocampal volumes using magnetic resonance imaging have been shown to have different trajectories across cognitive stages [45]. In the case of vascular related dementia and cognitive decline, neuroimaging and blood-based biomarkers (inflammatory markers) may also have the potential to further increase the accuracy of determining cognitive status [46] and contributing to mechanism related information.
This study has a number of strengths. To provide a comprehensive and unbiased review of the existing literature, a wider search strategy was used by including studies with different designs (i.e., observational and randomized clinical trials) and outcome measures (i.e., cognitive function, cognitive decline, and incidence of MCI and dementia). This approach also took into consideration the limited number of studies published in this area of research. Never the less, there are some limitations. The included studies are characterized by large heterogeneity in design, sampling frame, cognitive assessment methods, assessment of sodium intake, and analytical methods. This making it difficult to compare results. Further, sodium intake was mainly assessed using self-report tools including FFQs [27–31, 40], food diaries [27, 39], or a single question with binary responses probing the individual level of sodium intake [32, 41]. Therefore, there is risk of under-reporting or over-reporting and this could explain the lack of significant results and the mixed unexplainable results. Only two studies collected urine samples for objective measurement of sodium excretion; one on a sub-set of participants [28] and the other on total study population [34]. However, there are numerous difficulties with 24 h urine collection including feasibility in population-based setting, cost, and the need for logistical support (i.e., storage and analysis). One option to increase the validity and accuracy of FFQ would be to adjust sodium levels derived from FFQs with sodium values from 24 h urine samples collection from a subset of the study population. This is similar to the methods used by Haring et al. [28]. In that way, less resources would be used, yet the study would have a more accurate estimation of sodium intake from the adjustment. Last, only studies in English were included. Only seven studies [47–53] were excluded based on this criterion. Moreover, one of the results of the excluded study (from the abstract which was in English) alluded to the association of dementia with high-salt diet [47]. The other six non-English articles (abstracts were in English) also fit other exclusion criteria (five studies did not measure cognition and/or sodium intake levels [48, 51–53], one study was a review [50]) that were set for this study. Therefore, the exclusion of the non-English articles was unlikely to influence the overall interpretation and validity of the results.
Conclusions
The studies in this review reported heterogeneous findings on the association between sodium consumption and cognitive function in humans. Overall, the strength of the evidence is modest, which could be largely attributed to between-study differences in design, dietary, analytical, and cognitive assessment methods. Robust longitudinal analyses are needed to evaluate the association of different levels of sodium intake with cognitive decline to minimize the potential influence of residual confounding and reverse causality on the associations. Different target populations are needed including people with and without chronic vascular related conditions such as hypertension, heart disease, or kidney disease, to the add to the evidence base on the possible mechanisms on how the sodium-cognition pathway works, e.g., the gut mediated or vascular inflammatory pathway. The results from these further studies can then inform the design of targeted sodium-reducing nutritional and lifestyle interventions.
Footnotes
ACKNOWLEDGMENTS
This research was funded by the National Institute for Health Research (NIHR) (16/137/62) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care. The authors acknowledge the support of NIHR DePEC (Dementia Prevention and Enhanced Care) team members in this study.