
Abstract
An estimated 47 million people live with Alzheimer’s disease (AD) and other forms of dementia worldwide. Although no disease-modifying treatments are currently available for AD, earlier diagnosis and proper management of the disease could have considerable impact on patient and caregiver quality of life and functioning. Drugs currently approved for AD treat the cognitive, behavioral, and functional symptoms of the disease and consist of three cholinesterase inhibitors (ChEIs) and the N-methyl-D-aspartate receptor antagonist memantine. Treatment of patients with mild to moderate AD is generally initiated with a ChEI. Patients who show progression of symptoms while on ChEI monotherapy may be switched to another ChEI and/or memantine can be added to the treatment regimen. In recent years, putative disease-modifying therapies have emerged that aim to slow the progression of AD instead of only addressing its symptoms. However, many therapies have failed in clinical trials in patients with established AD, suggesting that, once developed, disease-modifying agents may need to be deployed earlier in the course of illness. The goal of this narrative literature review is to discuss present treatment algorithms and potential future therapies in AD.
INTRODUCTION
Alzheimer’s disease (AD) is a slowly progressive neurodegenerative disorder and the leading cause of dementia [1]. Approximately 50 million people live with AD and other forms of dementia worldwide, and the number of cases is estimated to quadruple by 2050 [2, 3]. Reflecting the overall aging of the global population, a Canadian population health modeling study for neurological diseases projected a 2-fold increase in the number of people living with dementia by 2031 [4]. AD has a sizable public health impact, and it is estimated that patients with dementia cost the healthcare system over 300% more than their cognitively intact peers in the same age group [5]. Furthermore, the impact of this disease has increased considerably during the past 2 decades; AD was the sixth leading cause of death in 2012 in the United States [5, 6]. In addition to causing disability and health problems for patients, AD may also place a substantial burden on caregivers [3].
There is a need for improved identification of individuals who may be developing AD. Most patients with AD routinely see their primary care physician, but most practitioners lack practice models to identify and treat patients with AD [7]. As few as 20% of Americans with AD are diagnosed with the condition, and 50% are exposed to inappropriate medications, with only 7% receiving cholinesterase inhibitors (ChEIs) [8–10]. Although there are no available disease-modifying treatments for AD, the currently approved therapeutic agents show benefits on measures of cognition, behavior, and daily function and include three ChEIs and one N-methyl-D-aspartate (NMDA) receptor antagonist [11]. However, even though these treatments are currently available, results from a recent real-world retrospective analysis of treatment patterns in the United States showed that approximately 57% received anti-dementia treatment after initial AD diagnosis, and approximately 52% of those initiating monotherapy with one of these agents continued treatment during the follow-up time period with approximately 22% discontinuing and remaining untreated [12]. A study assessing the effects of drug coverage policy on persistence and risk of discontinuation of ChEIs in new (post-policy change) versus old (pre-policy change) patients with dementia or AD in British Columbia found that persistence was significantly prolonged in new patients after the government began covering the cost of these agents [13]. Discontinuation rates were also lower for new versus old patients. Although it is unknown whether this positive change resulted from lower out-of-pocket fees, or new policy mandated follow-up visits and physician education programs, the finding demonstrates that healthcare policy changes can be beneficial in increasing drug utilization in patients with dementia [13].
The objective of this narrative review is to discuss current treatment algorithms and potential future therapies for the treatment of AD.
CHOLINESTERASE INHIBITORS
The three ChEIs currently approved for the treatment of AD in the United States are donepezil [14], galantamine [15], and rivastigmine [16] (Table 1). Tacrine, the first ChEI approved for the treatment of AD [11, 17], has been discontinued in the United States because of an association with hepatotoxicity and is not included here [18]. The currently approved indications and dosage information for ChEIs are listed in (Table 1).
Currently approved therapies for AD
AD, Alzheimer’s disease; AE, adverse event; BID, twice daily; BuChEI, butyrylcholinesterase inhibitor; ChEI, cholinesterase inhibitor; ER, extended release; HBr, Hydrobromide; HCl, Hydrochloride; NMDA, N-methyl-D-aspartate; ODT, orally disintegrating tablet; PD, Parkinson's disease; QD, once daily; TD, Transdermal.
Decreased cholinergic function is linked to cognitive impairment in patients with AD [11, 19]. ChEIs function by restoring the cholinergic pathway via their binding to, and inhibiting, acetylcholinesterase (AChE), and to a lesser extent butyrylcholinesterase (BuChE), thereby increasing the levels of acetylcholine at the synapse and presumably prolonging its physiological effect [11, 21].
Donepezil is a reversible, noncompetitive ChEI that was approved in 1996 in the United States [14]. It is metabolized in the liver and has the longest half-life of the ChEIs (approximately 60 hours in young volunteers and >100 hours in elderly patients) [22]. Donepezil is currently approved for mild, moderate, and severe AD and is available as regular and orally disintegrating tablets; donepezil oral solution was discontinued in the United States [14]. More recently, a higher-dose donepezil formulation (23 mg/day) was approved for the treatment of moderate to severe AD based on a large, randomized, double-blind study (N = 1,434) that demonstrated significantly greater improvements in cognition with donepezil 23 mg versus 10 mg at week 24, without improvement in measures of global status [23]. Adverse events (AEs), mostly gastrointestinal, were also reported at a higher frequency in the 23 mg group than in the 10 mg group [23].
Rivastigmine is an intermediate-acting, pseudo-irreversible, noncompetitive ChEI that inhibits BuChE with similar potency [19, 20]. It was approved by the United States Food and Drug Administration (FDA) in 2000 and is indicated for the treatment of mild, moderate, and severe Alzheimer-type dementia [16]. Unlike donepezil and galantamine, rivastigmine is not metabolized by the liver, making it more suitable for patients with renal or hepatic impairment [11]. Rivastigmine is available as an oral capsule (1.5, 3, 4.5, and 6 mg), oral solution (2 mg/mL), and transdermal patch (4.6, 9.5, and 13.3 mg/24 h; Table 1) [16, 24]. The 9.5 mg/24 h patch and the 6 mg twice-daily oral dose provide similar exposure, although fluctuations in maximum concentration (Cmax) and minimum concentration (Cmin) are less for the patch than with the oral formulation, which may result in a more favorable safety and tolerability profile with the patch [24–26]. Exposure is highest when the patch is applied to the upper back, chest, or upper arms; plasma exposure is approximately 20% to 30% lower when applied to the abdomen or thigh [27].
Galantamine is a short-acting, reversible, competitive ChEI that was approved in 2001 in the United States for mild to moderate AD [11, 20]. Galantamine is available in three formulations, extended-release (ER) capsules, tablets, and oral solution, which differ slightly in their pharmacokinetics [15]. The ER capsules and tablets are bioequivalent for the area under the concentration-time curve from 0 to 24 h and Cmin; however, Cmax of the ER capsule is 25% lower, and time to Cmax occurs in 4.5 to 5.0 h after administration compared with 7.0 to 8.0 h with the tablets [11, 15]. The bioavailability of the tablet formulation is equivalent to the oral solution formulation [15].
Mean difference between ChEIs, memantine, and placebo in cognitive, global, functional, and behavioral outcomes from meta-analyses of clinical trials
AD, Alzheimer’s disease; ADAS-cog, Alzheimer’s Disease Assessment Scale cognitive subscale; CDR, Clinical Dementia Rating scale; ChEI, cholinesterase inhibitor; CIBIC-Plus, Clinician’s Interview-Based Impression of Change Plus caregiver input; ND, not determined; NPI, neuropsychiatric inventory; SIB, Severe Impairment Battery. Functional outcomes based on various measures, including Alzheimer’s Disease Cooperative Study-Activities of Daily Living, Bristol Activities of Daily Living Scale, and Progressive Deterioration Scale. *p < 0.05; **p < 0.01; ***p < 0.001; npNo p value provided. aMean doses: donepezil 10 mg, galantamine 24 mg, and rivastigmine 8.5–10.4 mg. bRange of mean difference in individual studies. cDose range in individual studies: donepezil 5–10 mg, galantamine 16–32 mg, and rivastigmine 6–12 mg.
Evidence regarding time to institutionalization is mixed. Long-term use of ChEIs resulted in delayed nursing home placement in three observational studies, whereas no difference versus placebo in time to institutionalization or progression of disability was noted in the randomized controlled AD2000 study of donepezil [34–37]. Long-term treatment with donepezil (1 year) was also associated with reduced risk of functional decline versus placebo [38]. Furthermore, a long-term study in patients with possible or probable AD demonstrated that a 1-year delayed start of donepezil treatment resulted in greater global deterioration and significantly worsened cognitive function compared with earlier treatment [39].
Gastrointestinal disturbances are the most common AEs associated with ChEIs [28, 29]. A meta-analysis demonstrated that all three drugs significantly increased the risk of dizziness, nausea, anorexia, vomiting, and diarrhea versus placebo; donepezil and rivastigmine also significantly increased the risk of headache over placebo [28]. Agent-specific AEs considered very common (>10%) included diarrhea, headache, and nausea with donepezil; nausea and vomiting with galantamine; and diarrhea, dizziness, anorexia, nausea, and vomiting with oral rivastigmine [40]. Other commonly reported AEs (1% – 10%) included abdominal pain/disturbance and fatigue with all three ChEIs; anorexia, dizziness, and insomnia with donepezil and galantamine; and asthenia, headache, and somnolence with galantamine and oral rivastigmine [40]. Use of ChEIs may also be associated with urinary incontinence and subsequent initiation of urinary anticholinergic medications; use of urinary anticholinergics can decrease the efficacy of ChEIs and should be avoided in favor of alternative treatments for urinary incontinence [41]. Other possible side effects include muscle cramps, bradycardia, rhinitis, and vivid dreams [40, 42]. The rivastigmine oral and patch formulations differ slightly in the type and frequency of AEs, and the patch is associated with lower incidence of gastrointestinal AEs [25, 40]. Commonly reported AEs (1% – 10%) with the rivastigmine patch include anorexia, anxiety, abdominal pain, and application site reactions such as dermatitis, erythema, and irritation [40].
N-METHYL-D-ASPARTATE RECEPTOR ANTAGONIST
The voltage-dependent NMDA receptor antagonist memantine was approved in 2003 for the treatment of moderate to severe AD [43]; results from mild AD trials did not show consistent or robust benefit [44]. The currently approved indications and dosages for memantine are listed in (Table 1). Memantine may block the effects of excessive glutamate stimulation at the NMDA receptor, thereby preventing an excess of downstream calcium influx and oxidative stress [11, 45]. Elevated tonic glutamate levels in AD are thought to result from inefficient removal mechanisms at the synaptic cleft [11]. The abnormal buildup of glutamate leads to overactivation of NMDA receptors, with the resulting chronic excitotoxicity possibly contributing to neuronal loss and cognitive impairment [11, 45].
Individual clinical trials examining the benefits of memantine on cognitive, global, and functional outcomes have reported mixed results [28, 46–55], but the overall evidence has been sufficient to gain approval for treating patients with moderate to severe AD and not for milder disease stages. In the pivotal phase III clinical trials, memantine provided benefit (e.g., overall global change, activities of daily living, cognitive performance) in patients with moderate to severe AD when used as monotherapy [52] or in addition to donepezil [53]; however, another monotherapy trial in patients with moderate to severe disease failed to achieve statistical significance in primary or secondary endpoints [54]. In trials in patients with mild to moderate AD, the same extent of benefit has not been seen consistently with memantine (alone or as add-on therapy) [48–51, 55]. The efficacy of memantine therapy has been examined in meta-analyses that demonstrate significantly improved cognitive outcomes (as measured by the Severe Impairment Battery, ADAS-cog, Mini-Mental State Examination [MMSE], or Standardized MMSE in the individual trials) in patients with mild to severe AD (standardized mean difference versus placebo, – 0.27; p < 0.0001) [46] and in patients with mild to moderate AD (mean difference versus placebo, – 1.29; p < 0.01) [28]. Memantine therapy was also associated with beneficial effects on global and functional outcomes compared with placebo in patients with mild to severe AD in two meta-analyses [46, 47].
Findings from meta-analyses of memantine’s effects on behavioral outcomes have been inconsistent [28, 47]; as with ChEIs, clinicians often assess empirically whether memantine confers clinical benefit before considering use of psychotropics. Although the data presented here are not conclusive, they are encouraging, as memantine treatment appeared to be associated with lower costs, longer time to institutionalization, gains in quality-adjusted life-years [56], and significantly lower incidence of agitation compared with placebo in some studies [46, 47]. Encouraging results from studies on the effectiveness of memantine for reducing agitation may allow for reduced antipsychotic medication use in some patients [57–59]; however, there is currently no Level 1 evidence supporting the use of memantine for agitation.
Memantine is generally well tolerated [60]. Two-fold or higher incidences of headache, confusion, and somnolence with memantine versus placebo have been reported [48, 49]. Overall, the most common AEs (1% – 10%) included constipation, dizziness, headache, hypertension, and somnolence [40]. Because oral clearance is lower and elimination half-life is longer in patients with severe renal impairment, dose reduction in these patients is recommended [61, 62].
COADMINISTRATION OF CHOLINESTERASE INHIBITORS AND N-METHYL-D-ASPARTATE RECEPTOR ANTAGONIST
Coadministration of memantine and ChEIs has been evaluated in several trials [51, 63–66] and is proposed to have a synergistic effect [19]. A fixed combination of memantine and donepezil in a capsule form was approved in 2014 for moderate to severe AD (Table 1) [67]. The recommended dose of the combination treatment is 28 mg memantine XR and 10 mg donepezil once daily. The use of memantine and donepezil in combination is bioequivalent to coadministration of individual memantine ER capsules and donepezil [67].
Generally, current evidence suggests but does not definitively prove significant benefits with memantine and ChEI combination therapy over ChEI monotherapy (Table 2) [68–70]. A meta-analysis conducted by the European Academy of Neurology (EAN) found evidence supporting combination therapy over monotherapy in patients with moderate to severe AD [69]. Significant benefits were observed for behavior and mood (standardized mean difference, – 0.19; p = 0.002), cognitive function (– 0.27; p = 0.00001), and global outcomes (– 0.20; p = 0.0004), but not for activities of daily living (– 0.08; p = 0.12). Similar results were observed in a meta-analysis of seven trials in patients with mild to severe AD that demonstrated small but significant improvements in behavior (standardized mean difference, – 0.13; p < 0.03), activities of daily living (– 0.10; p < 0.02), and global outcomes (– 0.15; p < 0.04) with combination therapy versus ChEI monotherapy [68]. There were nonsignificant improvements in cognitive function (– 0.13; p < 0.06) [68], although these results were not confirmed in a meta-analysis of 14 trials in patients with mild to severe AD [71]. Combination regimens may also delay nursing home admission [72] and be more cost-effective than ChEI monotherapy [73]. A long-term observational study suggested that a combination of memantine and ChEI slowed cognitive and functional decline compared with ChEI monotherapy [74].
CURRENT TREATMENT ALGORITHMS
The current treatment guidelines for AD as established by the American Psychiatric Association (APA), the EAN, and the 4th Canadian Consensus Conference on the Diagnosis and Treatment of Dementia are listed in (Table 3) [33, 76]. Of note, the latest recommendations by the American Academy of Neurology (AAN) were published in 2001 [77], before the approval of memantine or the memantine/donepezil combination, and thus are mentioned only briefly in this review.
Practice guidelines for the treatment of AD
AD, Alzheimer disease; AE, adverse event; APA, American Psychiatric Association; CCCDTD4, 4th Canadian Consensus Conference on the Diagnosis and Treatment of Dementia; ChEI, cholinesterase inhibitor; EAN, European Academy of Neurology; MOA, mechanism of action; PK, pharmacokinetics; SSRI, selective serotonin reuptake inhibitor. *Formerly known as European Federation of Neurological Societies and European Neurological Society.
Therapy should be considered at the time of initial diagnosis of AD (Fig. 1) [76]. In general, the current treatment guidelines recommend the use of ChEIs for mild to moderate symptoms and memantine or memantine/ChEI combination therapy for moderate to severe symptoms (Table 3) [33, 75–77]. With the approval of the single, once-daily combination formulation of donepezil/memantine, this treatment regimen has become simpler, although the use of memantine and donepezil as two separate prescriptions is still an option. Memantine can also be coadministered with other ChEIs, although clinical trial data are limited [51, 78].
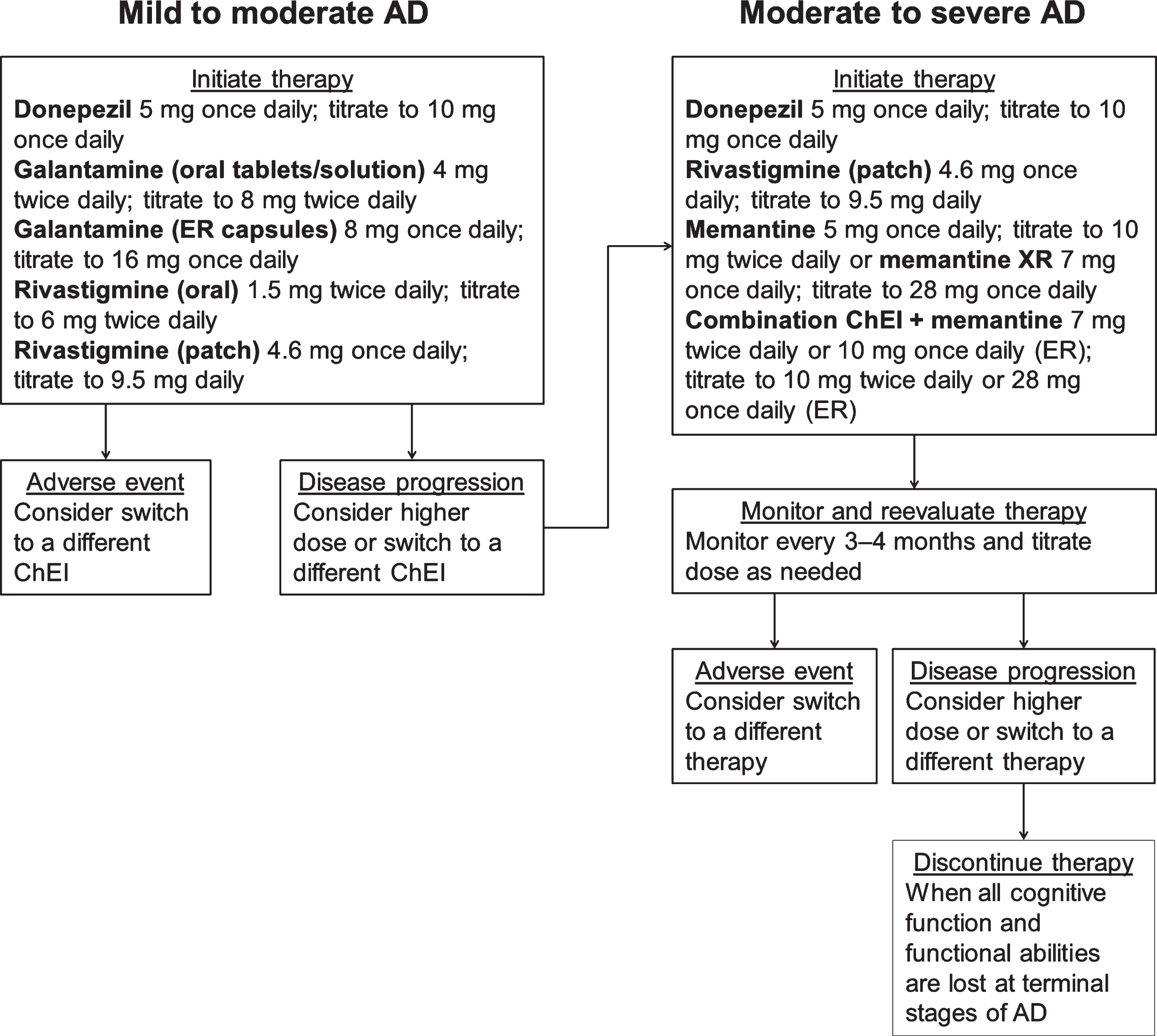
Treatment algorithm for Alzheimer’s disease based on severity of symptoms. AD, Alzheimer’s disease; ChEI, cholinesterase inhibitor; ER, extended release; XR, extended release.
Overall, in patients who show a progression of symptoms while on ChEI monotherapy, consideration should be given to either increasing the dose of their current therapy (if applicable), switching the patient to another ChEI, or adding memantine [79]. Information regarding dosage increases is conflicting. According to the APA 2014 guidelines, there was insufficient evidence to show clinically meaningful advantages of administering higher doses of donepezil [33], although clinicians may consider this on a case-by-case basis provided that close monitoring is performed. However, higher doses of a rivastigmine patch may be associated with greater benefit than lower doses [33]. A 24-week, prospective, randomized, double-blind study in patients with severe AD found superior effects on cognition and function at weeks 16 and 24 with the 13.3 mg/24 h rivastigmine patch compared with the 4.6 mg/24 h patch [80]. AEs and discontinuations were similar between the groups [80]. Similarly, patients who were switched to the 13.3 mg/24 h patch performed significantly better on functional outcomes compared with those who stayed on the lower 9.5 mg/24 h patch [81]. Although randomized, placebo controlled trials of cholinesterase inhibitors have shown benefit in regards to cognition, behavior, and daily function, as well as a slower rate of decline compared with untreated patients [82], no studies to date of ChEIs or memantine have shown significant reductions in time to conversion to AD in patients with mild cognitive impairment. This finding is reflected in the recent AAN practice guidelines wherein they recommend that if a clinician chooses to use these agents in a patient with mild cognitive impairment then they must first discuss the lack of clinical efficacy evidence with their patients [83].
Decisions about duration of treatment and therapy discontinuation should be made with care and take into consideration patient needs, comorbidities, presence of AEs, adherence, and effectiveness [75, 79]. In mild to moderate disease, lack of efficacy or presence of AEs should prompt consideration of a switch in therapy [79]. The presence of hallucinations and delusions before discontinuation of ChEIs may predict clinical deterioration [84]. Discontinuation of ChEIs may also be associated with cognitive decline [85–87]; however, antidementia drugs should be discontinued when patients with AD reach the terminal stage of the disease [75, 79], at which time they usually become eligible for hospice. At this stage, consideration should be given to stopping most, if not all, nonpalliative therapies.
RECOMMENDATIONS FOR THERAPIES FOR NEUROPSYCHIATRIC SIGNS AND SYMPTOMS
Treatments for neuropsychiatric features are an integral part of AD management. Estimates are that over time, >90% of patients with AD will develop behavioral/psychiatric changes [88, 89]. Although no agent is currently approved to treat these symptoms in the United States, antidepressants and antipsychotics are commonly used off label in patients with AD. In general, the use of antidepressants (e.g., selective serotonin reuptake inhibitors [SSRIs]) for the treatment of depressive symptoms associated with dementia is recommended (Table 3), although the available evidence is mixed [33, 75–77]. Similarly, treatment with antipsychotics should be undertaken with caution and only used for moderate or severe agitation, aggression, and psychosis that create significant distress or danger [33, 75–77]. The use of antipsychotics in frail elders with dementia is associated with serious complications, including cerebrovascular AEs and mortality [33, 75]. The mortality rates vary among first-generation (typical) and second-generation (atypical) antipsychotics, and 6-month mortality rates of up to 20% have been reported in patients with dementia (haloperidol, 20%; olanzapine, 13%; risperidone, 13%; quetiapine, 9%) [90]. Thus, the potential benefits with antipsychotic treatment should be weighed against risks [91].
The SSRI citalopram has shown treatment benefits at doses of 30 mg/day or greater [92, 93]. In patients with probable AD, citalopram significantly reduced agitation compared with placebo [92]. However, citalopram 30 mg/day was associated with QT interval prolongation, and patients older than 60 should not exceed a daily dose of 20 mg per FDA safety warning, which limits the use of citalopram among patients with AD [92, 94]. A recent study reported that citalopram (60 mg) reduced the amyloid-β concentration in cerebrospinal fluid in healthy adults and blocked the growth of amyloid plaques in an animal model, suggesting that it may have a disease-modifying role in AD [93]. Additionally, evidence suggests, but does not prove, possible behavioral benefits of donepezil and memantine [47, 95]. Further studies are needed to confirm these research findings and address their potential clinical relevance.
ALTERNATIVE THERAPIES
In general, there is insufficient evidence to support the routine use of other agents, including anti-inflammatory drugs, gingko, vitamin E, selegiline, estrogens, pentoxifylline, or statins, for the treatment of AD [33, 77]. A meta-analysis of dementia treatment strategies performed by Laver et al. reported that selegiline and ginkgo biloba showed statistically significant positive effects across seven studies each; however, the quality of these studies was low (due to risk of bias and inconsistency of results) and very low (due to very serious risk of bias and inconsistency of results), respectively [96]. In contrast, a large, randomized, placebo-controlled study did not show a cognitive or functional benefit for ginkgo biloba in patients with mild to moderate AD; however, the placebo group demonstrated little cognitive or functional decline and, consequently, may have reduced the likelihood of detecting a treatment effect [97]. The aforementioned meta-analysis by Laver et al. also reported that statins had no statistically significant effect across three studies with high-quality evidence [96]. A recent study indicates that statins may prove more effective in individuals with the ApoE4 allele of the apolipoprotein E gene [98], but further evidence is needed to support this finding. Data regarding postmenopausal hormone therapy have been mixed, with a large clinical trial demonstrating an increased risk of cognitive decline with hormone therapy and a 2013 meta-analysis of seven studies finding no overall effect of estrogen therapy on AD [99, 100]. Although research continues into the effects of non-steroidal anti-inflammatory drugs in preventing and treating AD, a meta-analysis demonstrated that the evidence does not support the use of these drugs to improve cognition or reduce AD severity [101]. The AAN 2001 guidelines recommended the use of vitamin E to slow progression of AD, but the more recently updated APA 2014 and EAN 2010 guidelines do not support this recommendation [33, 77]. Furthermore, there may be some safety concerns with high-dose (≥400 IU/day) vitamin E supplements [102], although the results of a more recent Veterans Administration (VA) study suggested that vitamin E (2000 IU/day) in combination with a ChEI was well tolerated and effective in slowing functional decline in older men with mild to moderate AD [55].
THERAPIES IN THE PIPELINE
In recent years, drugs that target the pathobiological processes involved in AD have emerged [103]. These putative disease-modifying therapies aim to slow the progression of AD instead of only addressing its symptoms [103]. Therapies currently in phase III trials that target the amyloid cascade include agents aiming to decrease amyloid-β production (β-secretase 1 inhibitors or γ-secretase modulators) or increase amyloid-β clearance (anti–amyloid-β antibodies or active immunotherapies) [103]. However, to date, all completed phase III trials that have tested these agents (e.g., bapineuzumab, solanezumab, verubecestat) have failed to meet their primary endpoints [104–106]. The failure of anti–amyloid-β drugs in AD has led to the hypothesis that such agents may need to be deployed earlier in the course of illness, before the brain is ravaged, possibly even before symptoms are manifest. Several clinical trials in individuals “at risk” for AD or with preclinical or prodromal AD are now under way.
In addition to drugs that target the amyloid cascade, drugs that target the tau pathway (tau aggregation inhibitors or anti-tau antibodies), as well as other targets (e.g., tyrosine kinase inhibitor, receptor for advanced glycation end-products inhibitor) are being investigated [103, 107]. Recently, phase III clinical trials of idalopirdine, a serotonin (5-HT6) receptor antagonist, failed to meet the primary efficacy endpoint of improving cognitive performance [108]. Targeting multiple pathologic pathways with different drug classes may be required for optimal disease management; this strategy is commonly used for hypertension, diabetes, cancer, and acquired immunodeficiency syndrome treatments [109]. Examples in AD management include an ongoing study of ALZT-OP1, which is a combination of the antiamyloid agent cromolyn and the anti-inflammatory agent ibuprofen [110], and a recent trial of solifenacin as an add-on to donepezil therapy [111]. The combination of solifenacin and donepezil increased tolerability versus donepezil alone and may allow for more optimized dosing of donepezil by overcoming AE-related dosing limits [111]. Similarly, repurposing existing drugs that are licensed for other indications, but have the potential to work in AD, may offer viable candidates for disease modification. However, development of future therapies and optimizing treatment may be a challenge until there is a better understanding of underlying disease mechanisms. If one or more disease-modifying therapies become available, we predict that there will still be a strong rationale for use of symptomatic therapies. It is unlikely that disease-modifying therapies will prevent symptoms altogether or that disease-modifying therapies will be used exclusively. Because the AD developmental pipeline changes frequently, we have only presented a relatively brief list of therapies. It was our intention to just provide the reader with a sense of the direction as to where this field was headed. Moreover, we believe that the treatments included provide an adequate representation of the many therapeutic approaches that are currently in various phases of development.
CONCLUSIONS
The current treatment algorithm for AD is based on the use of ChEIs for mild, moderate, and severe disease and adding memantine for moderate to severe disease. Treatment should be initiated at the time of diagnosis of AD dementia, the earlier the better, and patients should be monitored for disease progression. Future therapies may optimize currently available drugs and slow the progression of AD symptoms or even AD pathology. There is also the possibility that future therapies could delay or even prevent emergence of AD symptoms in those who are at high risk for the disease.