
Abstract
BACKGROUND:
The knee is one of the most common sites of injuries among soccer players. The incidence of knee injuries can be reduced by improving the neuromuscular control and core stability.
OBJECTIVE:
This study aimed to evaluate the effectiveness of injury prevention programs that include core stability exercises in reducing the incidence of knee injuries among soccer players.
METHODS:
Data were obtained from different databases (1985–2021). Only randomized controlled trials that used injury prevention programs that include core stability exercise to prevent knee injuries were included. The keywords used during the search were ‘knee injuries’, ‘core stability exercises’, ‘FIFA 11
RESULTS:
The pooled results of 7828 soccer players and 863700 exposure h showed an overall injury reduction of 56% per 1000 h of exposure in the intervention group compared to the control group with an injury risk ratio of 0.44 (95% CI 0.321–0.619;
CONCLUSIONS:
Injury prevention programs that include core stability exercises reduce knee injury rates among soccer players by 56% (46% in male and 65% in female soccer players).
Introduction
Injury is a persistent threat at all levels of competition, and of all injuries, knee injuries hold the greatest fear among athletes of being sidelined for an extended period [1]. Based on the outcomes from Sheffield, the knee is the most frequently injured joint (non-contact episode), with soccer and rugby having the highest risks [1, 2].
Therefore, preventive programs aimed at protecting athletes from this type of injury should be integrated into training sessions. Different injury prevention programs have been proposed to prevent knee and anterior cruciate ligament (ACL) injuries [3, 4]. Such programs include jumps [3], strength [5, 6, 7, 8], and a combination of different exercise training methods [4, 9, 10, 11].
During the last two decades, the importance of core stability for injury prevention and performance enhancement has been popularized. Integrating core stabilization exercises into injury prevention programs, particularly for the lower extremities, indicates decreased injury rates [12, 13, 14]. Core stability is defined as the capacity to maintain vertebral column equilibrium within its physiological limits by reducing displacement from perturbations and maintaining structural integrity [15, 16, 17, 18]. In addition, core stability is the kinetic chain foundation that facilitates the transfer of torque and momentum between the lower and upper extremities during gross motor tasks of sports, exercises, and daily living [19, 20, 21].
The implementation of core stability exercises in injury prevention programs is based on the theoretical framework that any dysfunction in the core musculature/lower extremity kinematics can lead to musculoskeletal injuries; thus, exercises that restore and enhance core stability are linked to injury prevention and rehabilitation processes [22]. One of the main risk factors for ACL injury is poor proprioception [23]. Core stability training improves proprioception by strengthening the core muscles and putting the involved ligaments under stress [24]. Thus, core stability training exercises can help minimize the risk of injuries to lower limbs, especially for ACL injuries.
To date, the ideal component of injury prevention programs could not be identified; however, multifaceted programs incorporating strength, balance, endurance, neuromuscular control of the core and lower extremities muscles are needed to reduce injury rates [12]. Previous studies suggested that an advanced injury prevention program that starts with neuromuscular control, then stabilization exercises followed by dynamic functional activities that require core stability can be successful in reducing injuries [15, 25]. Additionally, Marx [26] recently reported evidence that the risk of injury to the lower limbs can be dramatically decreased by performing an exercise program emphasizing core strength, balance, proprioception, and correct movement patterns. Shi et al. [27] suggested that core stability exercises can improve the rehabilitation of ACL injuries by increasing the motor control of the core. Therefore, the importance of core stability exercises was reported and documented to effectively minimize injury rate for lower limbs, especially for the ACL and during rehabilitation phases.
Several randomized control trials (RCTs) have been conducted to investigate the preventive effect of core stability exercises on ACL injury rates among athletes [28, 29, 30, 31, 32, 33, 34, 35, 36]. One of them studied the effectiveness of neuromuscular exercises, including core stability, in reducing the rate of acute knee injury in 4564 adolescent female soccer players [34]. The neuromuscular warm-up program significantly reduced the rate of ACL injury in the intervention group. Nevertheless, the change in absolute rate did not reach statistical significance, possibly owing to the small number of events. In contrast, a preventive training program that included core stability with a cluster RCT did not significantly decrease ACL injury rates [35]. This is most likely because their compliance with the preventive program in their study was low. In another study [29], a neuromuscular training program that included core stability was protective against injuries in all youth soccer players. A similar reduction in the risk of severe injuries, overuse injuries, and overall injuries was found in a study of female youth soccer players [33]. Meanwhile, an exercise program including core stability exercises called the ‘11’, developed by the Fédération International de Football Association (FIFA), showed no significant difference in the overall injury incidence between the intervention and control groups of adult male amateur soccer players [36].
The FIFA also developed another injury prevention program called the FIFA 11
Given the inconclusive findings [30, 34, 36] in three of the nine studies in the extant literature, there is a need to evaluate the role of injury prevention programs that include core stability exercises in preventing or minimizing soccer-related knee injury in general and ACL injury, using injury incidence rates to calculate its effectiveness. However, none of the previous studies on knee injuries in soccer players separately assessed the effectiveness of prevention programs that include core stability exercises in reducing knee injuries. Thus, this study aimed to conduct a systematic review and meta-analysis of RCTs investigating how knee injury rates are influenced by injury prevention programs that include core stability exercises among soccer players. This would provide evidence-based insights enabling comparison between training programs including core stability exercises and the training programs excluding core stability exercises for soccer players to prevent or reduce knee injuries.
Materials and methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to conduct this systematic review with meta-analysis [37], which was registered retrospectively in the International Prospective Register of Systematic Reviews, PROSPERO (CRD42020186703).
Search strategy
A literature search was performed in PubMed, MEDLINE/EMBASE, CINAHL, PEDro, and summon databases from inception until March 2021. Our literature search was performed using the following search terms: knee injury, core stability exercises, knee injuries, FIFA 11
Criteria for the included studies
Studies were considered for inclusion if the intervention used core stability exercise training to prevent non-contact knee or ACL injuries and if the study outcomes included knee or ACL injury incidence. All studies were RCTs or cluster RCTs. The compliance rate was at least 50% for the inclusion. The duration of the interventions had to be at least four months. Only English-language studies were considered. The only studies that met the inclusion criteria were those involving soccer players. The outcome measures were knee and ACL injury rates in the control and intervention groups. Studies were not excluded based on gender, age group, or skill level.
Criteria for the excluded studies
Studies were excluded if they (1) did not include core stability exercises in the intervention groups program; (2) were review papers, editorials, lectures, commentaries, abstracts, trial design papers, case studies, surgical techniques, and articles that were not peer-reviewed; (3) were designed to evaluate the uptake and adherence of an intervention program and had different exposure groups; (4) reported only physical measurements or performance and not knee and ACL injury rates.
Data collection, extraction, and analysis
Inclusion procedure
At least two authors reviewed all studies to confirm the findings, and a third reviewer helped the group reach a consensus when there were disagreements. After identifying an initial list of studies, reference lists of publications were checked for possible additional studies. References from the included articles were also reviewed to ensure that all articles met the inclusion criteria. In data collection processing, the authors separated studies focused on ACL injuries [32, 34, 35] from studies looking at general knee injuries [28, 29, 30, 31, 33, 36] to avoid misleading in the Results section and be clearer and more specific.
Data extraction
Two investigators independently extracted data from the selected full-text articles. Outcome data elements extracted from each study were the number of knee and ACL injuries (or injury rates), exposure hours, duration of follow-up, and compliance rate.
Methodological quality scores of the included studies
Methodological quality scores of the included studies
1: eligibility criteria; 2: random allocation; 3: concealed allocation; 4: baseline comparability; 5: blinded participants, 6: blinded therapists; 7: blinded assessors; 8: adequate follow-up; 9: intention-to-treat analysis; 10: between-group comparisons; 11: point estimates and variability.
EndNote version X9 was used for storage, collation, and screening of the studies. Primary outcome results from individual studies were extracted and collated in Excel (Microsoft Corp) (Redmond, Washington, USA) before preparation and transfer into Comprehensive Meta-Analysis software, version 3 (CMA.V3) (Biostat, Inc., Englewood, NJ, USA).
Meta-analysis
The extracted data were entered and analyzed for the meta-analysis using the CMA.V3. The injury incidence rate was calculated by dividing the number of incident injuries by the total time at risk and multiplying by 1000, as this accommodates variations in the exposure time of individual athletes. The injury risk ratio (IRR) was determined by dividing the injury rate in the intervention group by the infection rate in the control group. An IRR of less than one indicates a positive intervention effect: for example, an internal rate of return of 0.30 indicates a 70% reduction. In Fig. 2, the individual injury rates, IRR, and CI are shown. The CMA software used for the analysis outputs log IRRs, standard errors, and variance. An invariance random-effects model was used in this meta-analysis, with the assumption that studies used a variety of populations and contexts, included various exercise doses, and evaluated the core stability exercise in various ways. Each study’s sample size and confidence interval were also considered in our analysis.
Publication bias
Standard funnel plots were used to identify the signs of publication bias. Egger test [38] was used to confirm asymmetry, and the ‘trim and fill’ method [39] tests were used to determine whether the overall IRR calculation needed to be adjusted due to missing studies.
Methodological quality assessment
One investigator independently assessed the methodological quality of each study. The quality criteria and risk of bias were evaluated according to 11 criteria, as recommended by Cashin and McAuley [40]. Each item was scored as 1 point or 0 points. Score
Definitions of injury and athlete workload
Knee and ACL injury
An ACL injury was characterized as a first-time or recurring partial or complete rupture of the ligament that occurred alone or combined with other knee joint injuries. According to the recording club medical officer, a non-contact ACL injury occurs when there is no physical contact with another player or entity at the time of injury [41].
Athlete workload
Athlete workload was described as the number of active hours spent by athletes during the study in either training or matches [28].
Results
Trial flow
The initial search from different databases resulted in 3027 articles, of which 2090 were excluded due to duplicates, criticism articles, and review articles. Ten remaining articles were screened after applying the inclusion and exclusion criteria (RCT/CRCT, exercises, compliance, and duration).
The corresponding authors of some articles were contacted for additional information. One study was excluded because the duration of the intervention was
Characteristics and moderators of the included studies
Characteristics and moderators of the included studies
Abbreviations: M, Male; F, Female; RCT, Randomized Controlled Trial; The FIFA11
Injury rates per 1000 hours of exposure in the intervention and control groups of the included studies
PRISMA flow diagram of the systematic steps in articles screening for inclusion.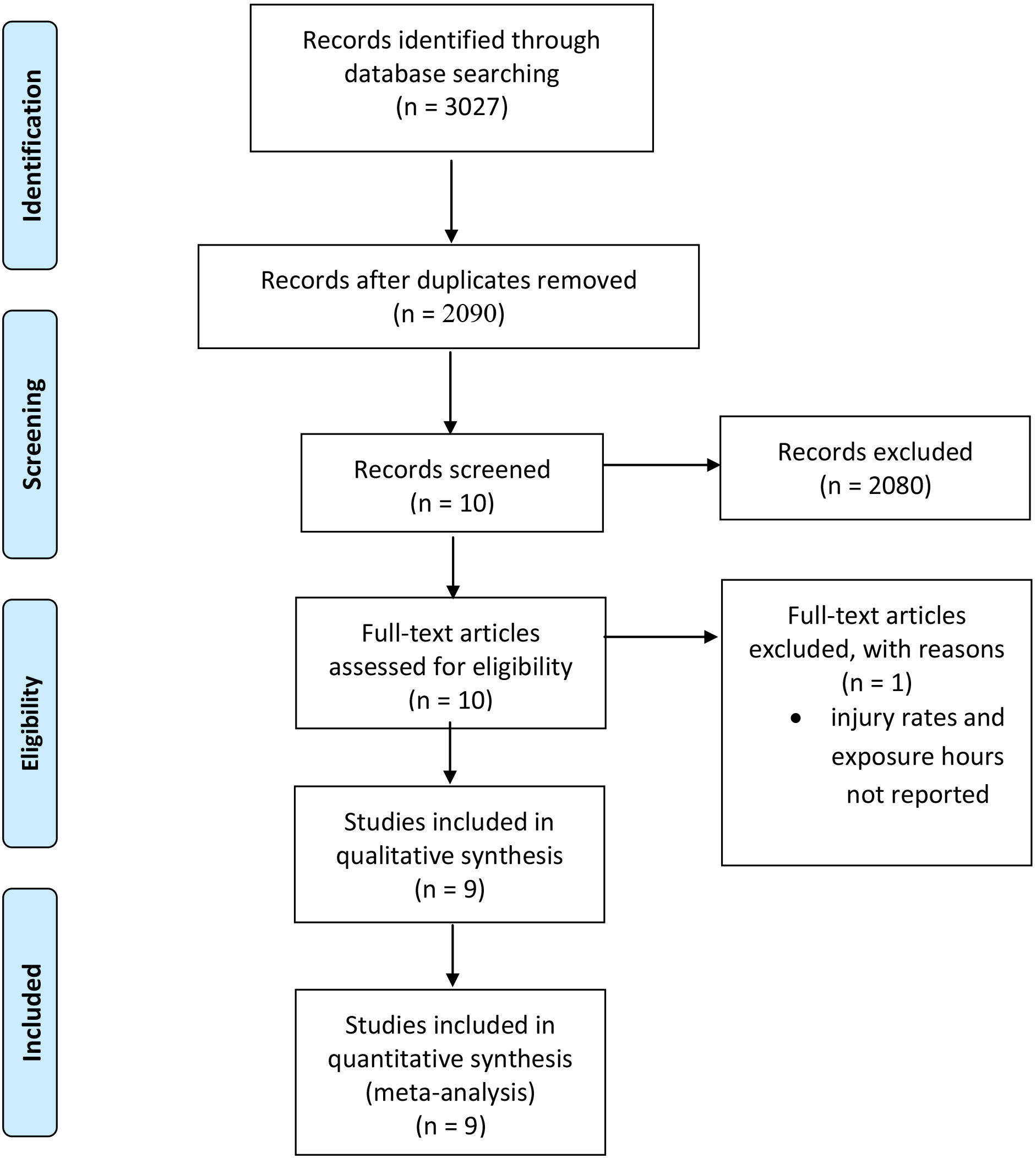
less than four months. Nine studies were included in the analysis. Figure 1 represents the systematic steps in screening articles for inclusion using the PRISMA flow diagram method. Table 2 presents the characteristics of the included studies and shows the methodological quality scores ranging from 4 to 7 (out of 10).
Forest plot illustrating the effectiveness of IPPs that include core stability training versus controls on knee injury risk ratio. IPPs 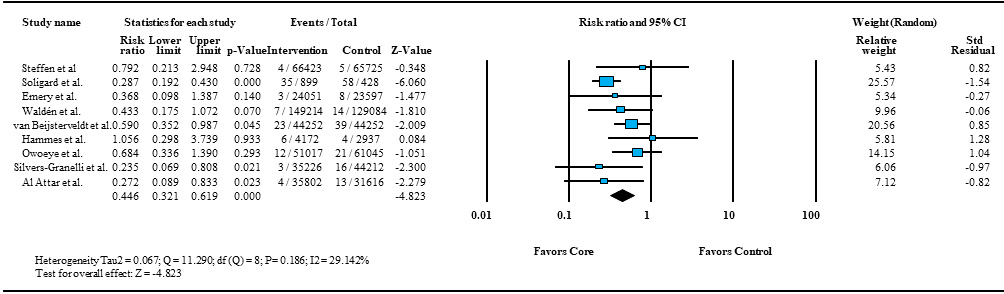
Forest plot illustrating the effectiveness of IPPs that include core stability training versus controls on ACL injury risk ratio. IPPs 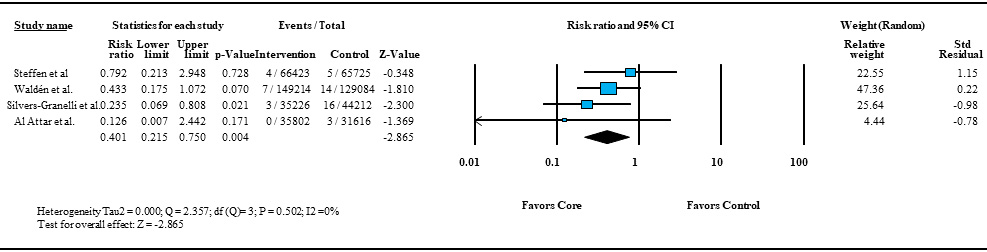
The study characteristics of the nine included studies summarized in Tables 2 and 3 show the injury rate and hours of exposure for both the intervention and control groups.
Pooled injury estimates
The nine included studies collected pooled data of 7810 individuals, 863,700 exposure hours, and 451 knee injuries. The pooled IRR of the intervention and control groups were 5.34 and 8.56 injuries per 1000 h of exposure, respectively (Table 3).
Meta-analysis results
Reduction of knee injuries
The pooled results showed a 55% overall injury reduction per 1000 h of exposure in the injury prevention program group (intervention group) compared to the control group (IRR 0.446; 95% CI 0.321–0.619;
Reduction of ACL injuries
The pooled results showed a 60% overall injury reduction per 1000 h of exposure in the injury prevention program group (intervention group) compared to the control group (IRR 0.401; 95% CI 0.215–0.750;
Reduction of knee injuries subgroup analysis male and female
The pooled results showed 46% knee injury reduction per 1000 h of exposure in males (IRR 0.537; [95% CI 0.355–0.813];
Forest plot illustrating the effectiveness of IPPs that include core stability training versus controls on knee injury risk ratio in (top) males and (bottom) females.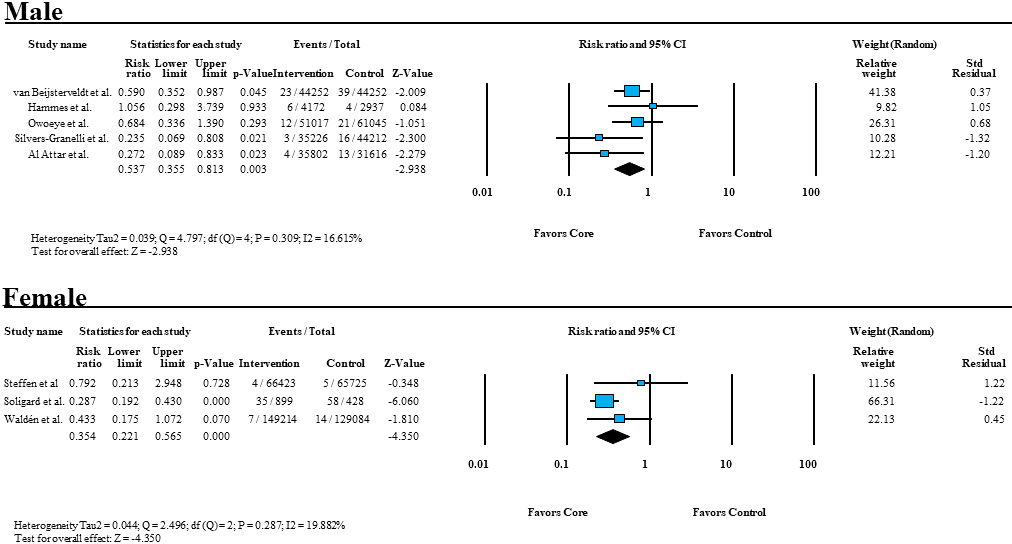
Funnel plot based on the study standard error (y-axis) and log risk ratio (x-axis) to assess publication bias. Circles indicate the study’s estimated point based on the procedure by Duval and Tweedie. The pooled estimate injury risk ratio (IRR) is presented as a diamond with the width corresponding to the CI, and the vertical line (centre of the diamond) is the overall effect. Large studies with higher power are placed toward the top, and lower powered studies are placed toward the bottom. The plot will resemble a symmetrical, inverted funnel in the absence of bias.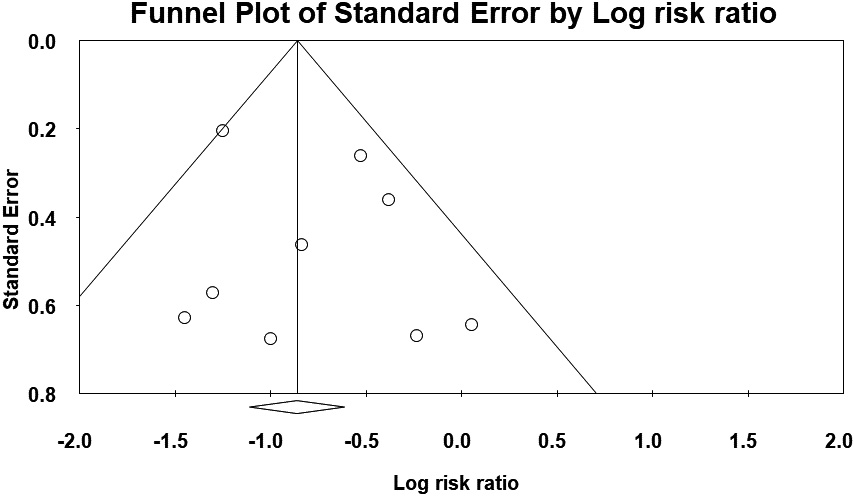
Inspection of the funnel plots showed a slight asymmetry, confirming the absence of publication bias (Fig. 5). The Egger test confirmed symmetry (0.73; 95% CI,
Discussion
This study aimed to investigate the effects of injury prevention programs that include core stability exercises on knee injuries. The study revealed differences between the group who performed core stability exercises and those who did not. To the best of our knowledge, this is the first systematic review and meta-analysis to specifically examine the effects of injury prevention programs that include core stability exercises, especially in preventing knee injuries among soccer players. This systematic review included nine RCTs [28, 29, 30, 31, 32, 33, 34, 35, 36, 41]. Additionally, the present study included male and female athletes with good variation between the ages of 12 and 45 years. This study provides strong evidence that injury prevention programs that include core stability exercises effectively reduce the risk of overall knee injuries and ACL injuries in male and female soccer players.
Several previous studies have concluded that core stability training can alter the biomechanical patterns of the trunk, hip, and knee; thus, it could be appropriate to prevent knee injuries, particularly ACL injuries, which distinguished this study. In addition, neuromuscular control deficits can lead to increased lateral trunk motion, hip adduction, and knee abduction, which may increase strain on the ACL and lead to injury [42, 43]. Moreover, the efficacy of injury prevention programs that include core stability exercises to decrease knee and ACL injury rates has been mentioned in different studies, and this is consistent with the findings of the present study [28, 29, 30, 31, 32, 33, 34, 35, 36, 41]. In a cluster randomized controlled trial of 4564 Swedish players aged 12–17 years, Waldén et al. [35] reported that a neuromuscular warm-up program significantly reduced the ACL injury rate in adolescent female soccer players.
Of the studies included in this systematic review, only one reported that implementing the FIFA 11
Additionally, only one randomized control trial study from the included studies targeted both men and women and found no difference in the effectiveness of neuromuscular training program in reducing all injuries and acute onset injuries in both sexes by using valid injury surveillance and cluster adjusted analysis. This result may be due to the unequal distribution of males and females between the two study groups, and therefore the ability to investigate effect modification was limited [29].
We conducted a sex-based subgroup analysis in our study, as three studies involving female participants and five involving male participants met our inclusion criteria. Male knee injuries were reduced by 46%, while female knee injuries were reduced by 65%. Our results support that injury prevention programs that include core stability exercises effectively reduce knee injuries among soccer players.
Given the present study’s findings, core stability exercises are an important part of any prevention program to decrease the rate of knee and ACL injuries in soccer players; it will also be helpful for both male and female athletes.
Considering previous studies and the results of the current study findings, this will lead to one of the main causes attributed to the importance of comparing training programs including core stability exercises and the training programs excluding core stability exercises for soccer players to prevent or reduce non-contact ACL and knee injuries. In addition, core stability exercises will be effective for both male and female athletes. Moreover, the findings of this study indicate that increasing the frequency of core stability exercises and injury prevention programs per week will enhance muscle strength and neuromuscular control in soccer players. Additionally, we found that a higher compliance rate leads to a reduced incidence of injury among teams/players, which helps to reduce overall injury rates.
This study has some limitations, as most of the studies included in our meta-analysis did not include information about the professional level of play. In addition, there was a lack of data on players between 25 and 35 years of age in most of the included systematic reviews. Differences in the quality scores of the studies may also have affected our results. Moreover, differences in exercise frequency per week and compliance variation between studies would have increased the variation in the study results. Therefore, we suggest setting a frequency of 3–5 times per week in a future meta-analysis.
Based on the findings of this study, we propose several suggestions to improve the quality of findings on the prevention of knee injuries. There is a need to focus more on the professional level of play; moreover, we need to conduct a more systematic review of samples between 25 and 35 years of age. The variation in compliance among studies should be decreased as much as possible to enhance the accuracy of the results. It is also important to ensure that all included studies had high-quality scores. Furthermore, the threshold frequency of the exercise bouts in the intervention programs should be set as an inclusion criterion.
Conclusions
This study explored the effects of injury prevention programs that include core stability exercises on knee and ACL injuries. It was found that exercise programs that included core stability exercises reduced knee injury incidence by 46% in men and 65% in women. Thus, we suggest that core stability exercises should be included in prevention programs to decrease the rate of knee injuries among soccer players. These results indicate the importance of core muscles in preventing contact and noncontact injuries to the lower limbs. Additionally, it was found that a higher compliance rate leads to a higher chance of injury prevention among teams, which will help to reduce the overall injury rates.
In conclusion, athletes who follow any injury prevention program, including core stability exercises, may significantly reduce the rate of knee injuries.
Author contributions
CONCEPTION: Wesam Saleh A. Al Attar.
PERFORMANCE OF WORK: Wesam Saleh A. Al Attar.
INTERPRETATION OR ANALYSIS OF DATA: Wesam Saleh A. Al Attar.
PREPARATION OF THE MANUSCRIPT: Wesam Saleh A. Al Attar, Hussain S. Ghulam, Saud Al Arifi, Amirah M. Akkam, Ahmed I. Alomar and Ross H. Sanders.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Wesam Saleh A. Al Attar, Hussain S. Ghulam, Saud Al Arifi, Amirah M. Akkam, Ahmed I. Alomar and Ross H. Sanders.
SUPERVISION: Ross H. Sanders.
Ethical considerations
This study, as a systematic review and meta-analysis, is exempt from Institutional Review Board approval.
Funding
WSA would like to thank the Deanship of Scientific Research at Umm Al Qura University for supporting his work by Grant Code: (22UQU4331100DSR01).
Footnotes
Acknowledgments
Wesam Saleh A. Al Attar acknowledges the Deanship of Scientific Research, Umm Al Qura University Grant Code: (22UQU4350385DSR01).
Conflict of interest
The authors have no conflicts of interest to report.