
Abstract
BACKGROUND:
Reduced mobility of upper and lower limbs has been associated with injuries in athletes. The Combined Elevation Test (CET) and the Weight-Bearing Dorsiflexion Lunge Test (WBDLT) are frequently used in clinical and research settings in face-to-face evaluations. However, some situations require physical distancing, and it is unknown whether those tests via telehealth are reliable.
OBJECTIVE:
To evaluate the intra-rater reliability, the Standard Error of Measurement (SEM), and the Minimum Detectable Change (MDC) for considering a real change on the CET and WBDLT were calculated for healthy athletes via telehealth.
METHODS:
67 athletes (25 years, 73 kg, and 1.75 m on average) participated in this study. 37 athletes performed the CET and 50 performed the WBDLT (20 performed both tests). Reliability was assessed through two online evaluations (7 to 15-days apart).
RESULTS:
ICC
CONCLUSIONS:
Telehealth-based findings relating to CET and WBDLT are reliable in healthy adult athletes and can be used to screen this population when face-to-face evaluations are not feasible.
Background
Mobility tests are frequently used to assess athletic and non-athletic populations, either in healthy individuals as part of injury prevention programs, or in those undergoing post-injury rehabilitation to assess changes after a treatment and the likelihood of return to sports practice [1, 2, 3].
The Combined Elevation Test (CET) is a mobility test that assesses the active range of motion of the trunk and shoulders, including thoracic extension and elevation of the arms against gravity [3, 4, 5]. The CET was developed to assess swimmers, but it has been also used to assess different athletic or non-athletic populations due to the association between shoulder pain and reduced mobility of the thoracic spine and glenohumeral joint [2, 3, 6].
The Weight-Bearing Dorsiflexion Lunge Test (WBDLT) assesses the ankle weight-bearing dorsiflexion range of motion [7, 8]. It is widely used to access athletes of several sports modalities, such as cutting/pivoting sports [2, 9, 10, 11, 12, 13, 14], cricket [15], volleyball [16], running [17], judo [18], and artistic gymnastic [19]. The reduced ankle dorsiflexion range of motion has been associated with several lower limb injuries [9, 11, 15, 20, 21], so the WBDLT is considered a key component of periodic health evaluation using screening tests and is frequently used as outcome measure of clinical trials [7, 20, 21, 22].
The CET and the WBDLT are easily assembled and performed using inexpensive materials often used in face-to-face evaluations. Furthermore, those tests do not need a specific clinical environment and they can be applied in situations when face-to-face evaluations are disrupted or discontinued.
Recently, the COVID-19 pandemic required social distancing and showed that the assessment and periodical health evaluations of athletes may be a challenging situation. In this context, there was a need for alternative ways of continuing evaluating athletes for prevention or for rehabilitation of musculoskeletal injuries. So, the assessment via telehealth emerged to replace face-to-face assessments when they were not secured. Besides the pandemic context, telehealth has the advantage of assuring the screening and clinical follow up with no need for clinic time and space, diminishing the costs for the clinician and also reducing time and money spent on the transportation of the patient to the clinic [23, 24].
Some psychometric properties of the CET and the WBDLT have been investigated previously using a face-to-face assessment [2, 3, 6, 7, 16, 20, 25]. However, the circumstances that the measurements are taken might influence the psychometric properties of an instrument. With regard to telehealth assessments, data referring to reliability, measurement error, and minimum detectable change have not yet been presented. Therefore, the aim of this study was to evaluate the intra-rater reliability, error measurement and minimum detectable change of these two mobility tests performed via telehealth assessments with healthy athletes.
Methods
Subjects
Sixty-seven asymptomatic athletes (86.5% amateurs; 25 years, 73 kg and 1.75 m in average) were recruited through online advertisements posted in social media between January and July of 2021. Athlete’s demographic characteristics and level of training/competition are shown in Table 1, according to the test performed. 37 athletes (19 males) performed the CET and 50 athletes (24 males) performed the WBDLT. In total, 20 athletes performed both tests, so their demographic characteristics were duplicated for each test.
Characteristics of the athletes that performed the combined elevation test and the weight-bearing dorsiflexion lunge test
Characteristics of the athletes that performed the combined elevation test and the weight-bearing dorsiflexion lunge test
kg: kilogram; m: meters. Values expressed in Mean
Athletes were included if they: 1) presented at least two years of experience in any sports modality; 2) were classified as “physically active” according to the Brazilian Portuguese version of the International Physical Activity Questionnaire – Short Form [26, 27]; 3) were enrolled in a sports club or team; 4) participated in sports competitions in the last two years and 5) did not present history of surgery or bone fracture in the previous twelve months or joint dislocations. Athletes who missed an evaluation or reported pain/injury during the study period were excluded.
A questionnaire was sent via Google
This study was approved by the Human Research Ethics Committee of the Federal University of São Carlos (No. 4.365.562), São Carlos, SP, Brazil. All athletes received explanations about the study and those who agreed to participate signed an online informed consent via Google
The athletes interested in participating in this study answered an online form (via Google
Three independent raters (GVG, HRFF, and MTMJ) contacted, screened, and conducted the standardized online evaluations with the athletes, supervised by three experienced physiotherapists (DHK, GMB, and LBC). All raters participated in a standardized training before the beginning of the study, and the whole procedure of recruiting, contacting, checking for eligibility, and both online evaluations of each athlete was made by the same rater. Inter-rater reliability was not assessed in this study L134-6.
Each athlete participated in two 20-min real-time evaluations via Google
In both assessment sessions and before the mobility tests, all athletes performed a warm-up consisting of aerobic exercises (skipping and jumping jacks) for 3-min with moderate intensity, according to the Modified 1–10 Rating of Perceived Exertion Scale [34]. Then, the athletes performed the CET or WBDLT, according to their sport modality. The athletes of overhead, water, combat, and racket sports performed the CET. The athletes of modalities that involve jumping, running, combating, and change of direction abilities performed the WBDLT. When the sport modality involved movements in both upper and lower body, the athlete was invited to perform both tests.
Combined elevation test (CET)
The CET assesses the combined active range of motion of the thoracic extension and arm elevation against gravity [3, 4, 5]. Prior to the assessment session, the athletes received instruction to build a simple device using paper and masking tape. The athlete folded the paper and attached it to a masking tape that was vertically placed on the wall. The folded paper was supposed to slide up on the vertical tape while the athlete performed the test, enabling the athletes to measure the test’s outcome (Fig. 1).
Device made for assessing the combined elevation test.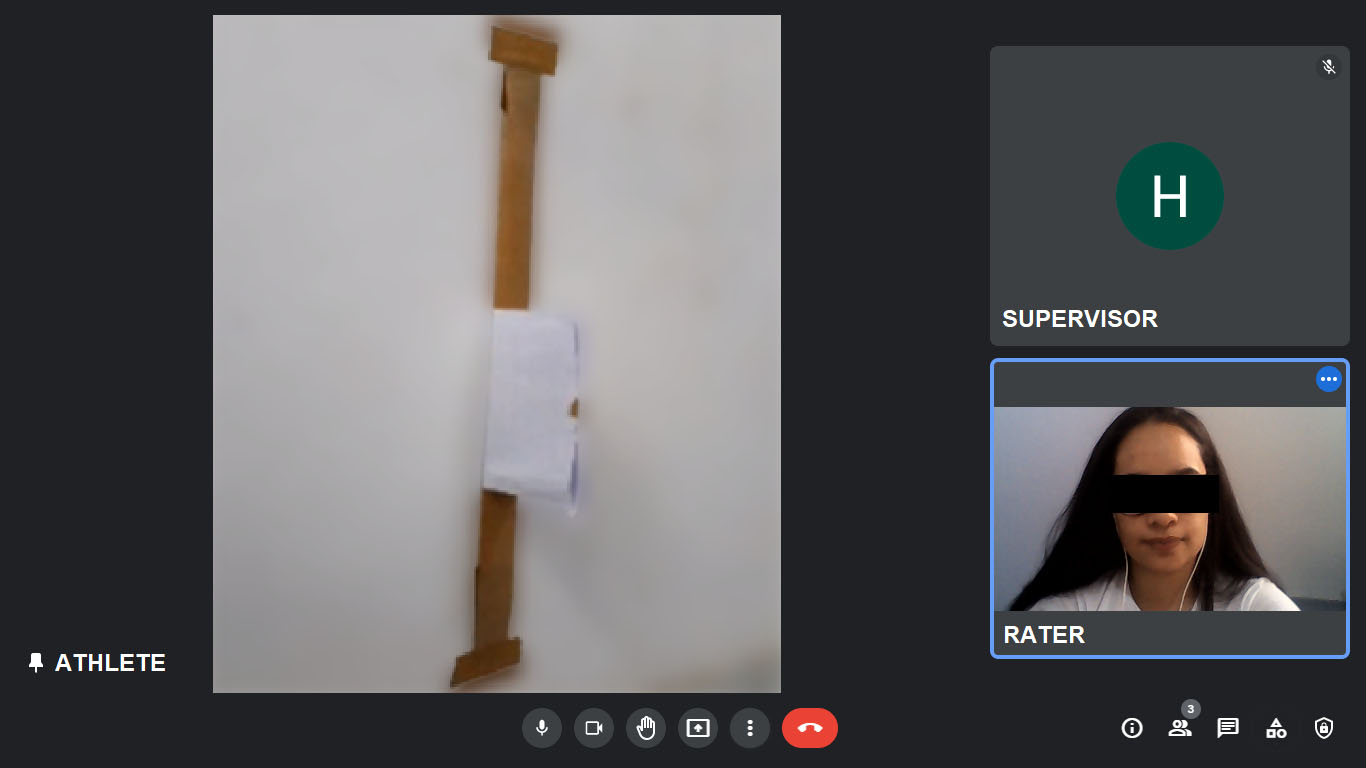
Starting position for the combined elevation test assessment.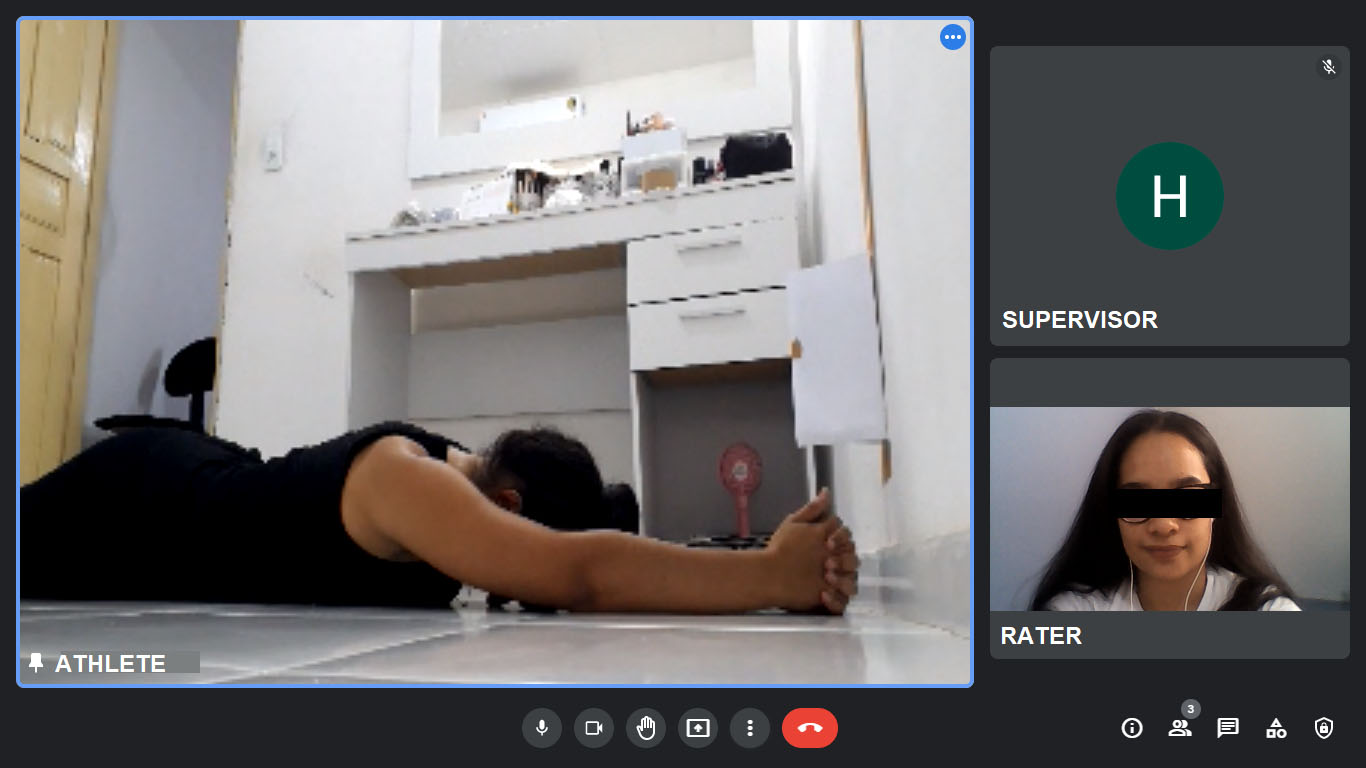
The laptop/smartphone camera was positioned laterally, providing the rater a view of the device and the athlete’s torso. Then, they were instructed to lie prone on the floor, with the forehead in contact with the floor, upper limbs positioned above the head (approximately 180 degrees of shoulder flexion), elbows fully extended and fingers intertwined with the thumbs pointing to the ceiling (Fig. 2) [1, 3]. During the test, the athletes deeply breathed in and raised their upper limbs off the floor, reaching the maximum height they could while sliding up the folded paper with their intertwined fingers [1, 3]. The forehead and torso should remain in contact with the floor during the test (Fig. 3). If the forehead lost contact with the floor or the device did not work properly, a new trial was performed. No words of encouragement were given during the test [1, 3].
Final position for the combined elevation test assessment.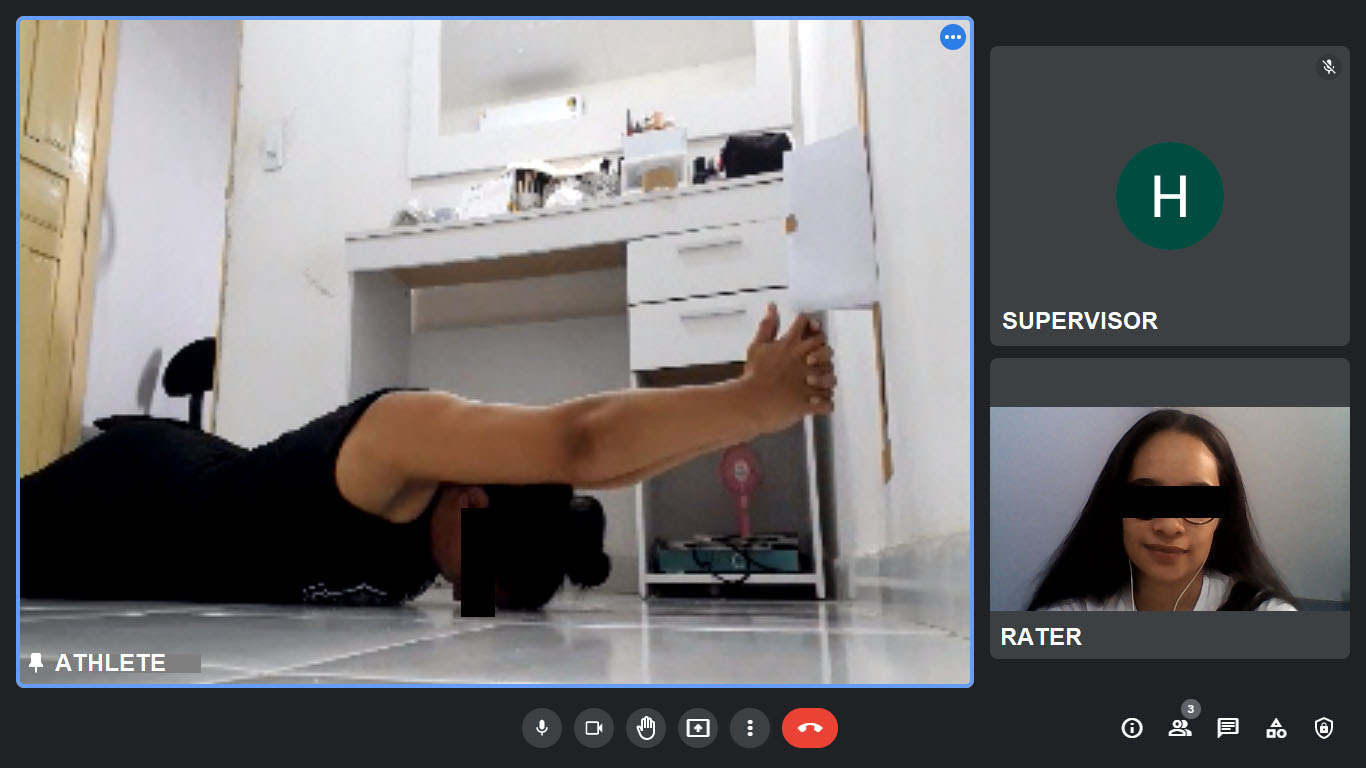
In both sessions, a familiarization trial was allowed before the athlete performed three maximum efforts, with 20-s rest period between them. The perpendicular distance between the inferior border of the folded paper and the floor was measured (in cm) and the mean value of the three trials was considered for the analysis.
The WBDLT was used to assess the range of motion of the ankle during weight-bearing dorsiflexion [7, 8]. To determine the order of assessment, dominant and non-dominant limbs were randomized in the first assessment session and the order was repeated in the second assessment session. To guide the alignment of the lower limb during the test (foot, leg, and hips), the athletes were instructed to place a 40 cm length masking tape line on the floor. Then, they placed a 70 cm length vertical tape on the wall, aligned with the tape on the floor (Fig. 4).
Set-up for the weight-bearing dorsiflexion lunge test assessment.
The athlete assumed the lunge position while facing the wall, with the foot to be assessed in front. The second toe and the heel of the foot to be assessed should be aligned with the tape on the floor, while the contralateral limb could be freely positioned. To maintain balance, the hands should be placed on the wall [7, 8].
The laptop/smartphone’s camera was positioned close to the wall and laterally to the assessed ankle, providing the rater a view of the athlete’s lower limb during the test. Then, the athlete was instructed to lunge forward and touch the patella against the masking tape placed on the wall, while keeping the knee in line with the second toe and the heel on the ground. The test aimed to obtain the maximum distance between the tip of the second toe and the wall, keeping the heel on the floor (i.e. maximum dorsiflexion angle) (Fig. 5) [7, 8].
The Weight-bearing dorsiflexion lunge test assessment.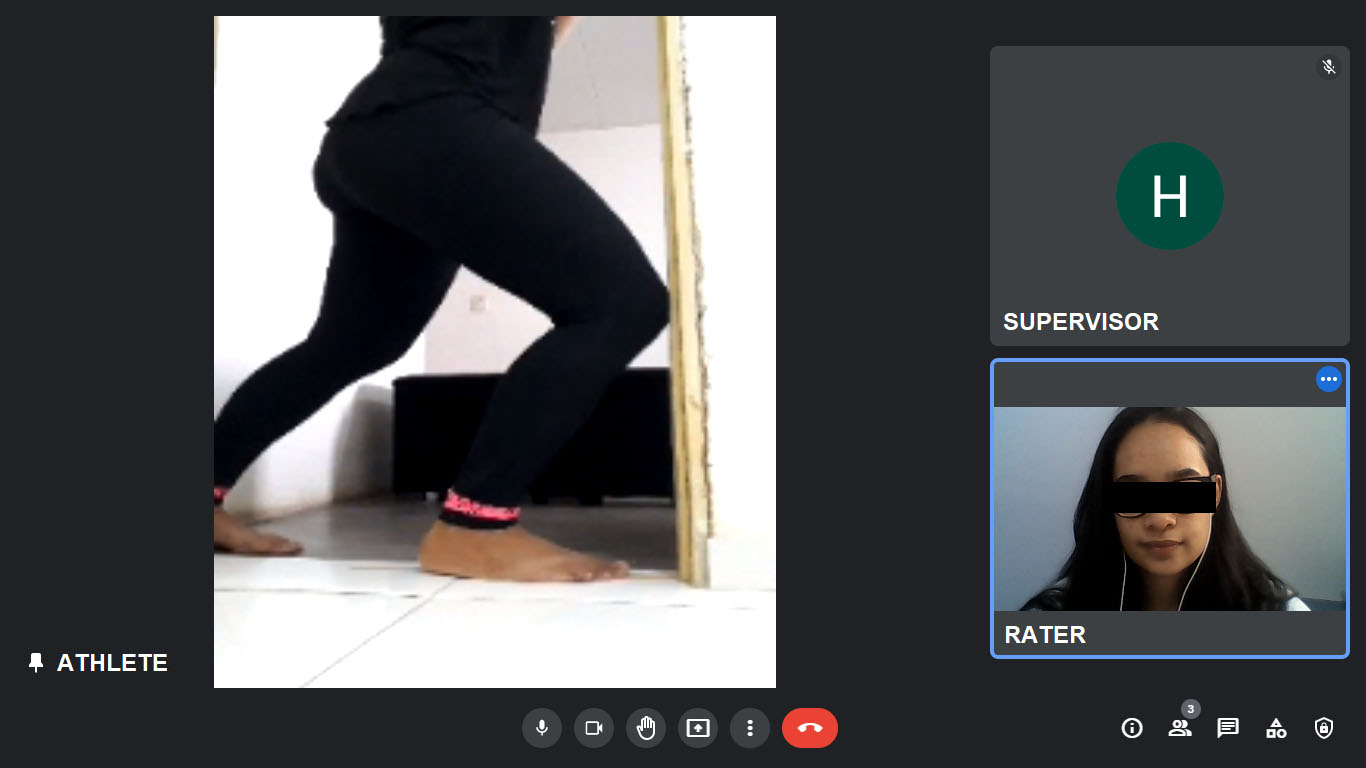
Sports modalities of the athletes that performed the combined elevation test
Sports modalities of the athletes that performed the weight-bearing dorsiflexion lunge test
Each lower limb was alternately tested twice, with no rest between trials. No familiarization trial was necessary and the number of lunge attempts for reaching the maximum dorsiflexion angle was not restricted. The athlete was instructed to measure the distance between the tip of the second toe and the wall (in cm) when the maximum distance was reached keeping the heel on the floor. The mean value of the two trials of the dominant and non-dominant limbs was considered for the analysis.
Descriptive data was presented as mean and Standard Deviation (SD). Data normality was verified by Kolmogorov-Smirnov’s test. The intra-rater reliability was measured with the Intraclass Correlation Coefficient (ICC) and with a 95% Confidence Interval (95%CI). The intra-rater reliability was analyzed with an ICC
The IBM
Results
The predominant modalities of the athletes that performed the CET were handball/beach handball (48.6%), rugby (13.5%), and water sports (13.5%) (Table 2). For those who performed the WBDLT, handball/beach handball (36%), rugby (14%), and athletics (10%) were the most common modalities (Table 3).
Results of the intra-rater reliability for the total sample
Results of the intra-rater reliability for the total sample
SD: Standard Deviation; ICC: Intraclass Correlation Coefficient; 95%CI: 95% Confidence Interval; SEM: Standard Error of Measurement; MDC
Values of mean, SD, ICC, SEM, and MDC
Table 4 shows the data analysis by sex. For the CET, men presented excellent intra-rater reliability (ICC
The aim of this study was to evaluate the intra-rater reliability of two mobility tests (WBDLT and CET) applied in healthy athletes via telehealth assessment. Our findings indicated good-excellent intra-rater reliability for the CET and the WBDLT considering the total sample. In addition, SEM and MDC
CET
The CET measures active trunk and shoulder mobility and has been widely applied to athletes of different ages, sports modalities, and levels of competition [2, 5, 36]. Previous studies showed excellent intra-rater reliability for the CET applied face-to-face in healthy adolescents [3], young cricket athletes [6], and elite soccer athletes [2]. The results of this study indicated that CET applied via telehealth presents similar reliability to face-to-face assessments.
The SEM and MDC of the present study were also similar to previous face-to-face studies. The CET via telehealth showed approximately 7% of error, which is low and equivalent to the error observed in face-to-face evaluations with healthy adolescents [3] and cricket athletes [6]. In this study, the CET presented a MDC
WBDLT
In accordance with the results obtained in this study, several studies also presented excellent intra-rater reliability for the WBDLT for young and healthy cricket athletes [6], elite soccer players [2], volleyball athletes [16], and adults with and without a history of ankle injuries/disorders [7, 20, 25]. Similarly, these studies also used the toe-to-wall distance as the test’s measure, once it is easier to assess and has equivalent reliability to the assessment in degrees [7].
In the present study, the WBDLT presented a mean SEM of 7%, which was similar to other studies that showed SEM values ranging from 4 to 6% [7, 25] in healthy adults and 5% in healthy females volleyball athletes [16]. Furthermore, a study assessing subjects with ankle dysfunctions observed a SEM of 4% [20]. Apparently, the WBDLT applied via telehealth presents higher SEM values compared to face-to-face assessments, but still, they can be considered small.
Furthermore, this study’s results showed that smaller changes than 2 cm should not be considered relevant for the WBDLT applied via telehealth. This finding is in accordance with previous studies that assessed subjects with and without ankle disorders history using face-to-face modalities of assessment and showed MDC
Clinical implications
Carrying out physical evaluations through real-time video calls has become a common alternative when social distancing between athletes and clinicians is necessary or preferable. Considering this context, this study showed that applying two mobility tests through real-time video calls and using low-cost materials that are easily available is reliable and can be used for screening athletes beyond the clinical environment. Nevertheless, we faced some specific challenges related to telehealth assessments, such as poor internet connection and losses in the video/audio quality due to problems with the camera, poor light, noise, and/or limitations of electronic equipment. However, these problems did not negatively impact the reliability of the tests.
Limitations of the study
The sample of the present study is composed of healthy athletes of 18–40 years old and, so the results should not be generalized for other populations such as injured adults, children or teenagers, or the non-athletic population. The sample was also heterogeneous in terms of sports and competition levels. Finally, the present results should not be generalized to inter-rater assessments.
Suggestions for future studies
Further studies should assess reference values, inter-rater reliability, validity, and responsiveness of the WBDLT and CET applied via telehealth. Although WBDLT and CET showed satisfactory reliability, it is unknown whether the telehealth assessments would present similar results in comparison to the same tests assessed face-to-face. Also, future studies should investigate the reliability, SEM, and MDC according to the sports modalities and competition, age, and presence of injuries.
Conclusion
The findings of this study showed that both CET and WBDLT via telehealth are reliable in healthy adult athletes and can be used to screen this population when face-to-face evaluations are not feasible. Assessing a patient via telehealth diminishes the costs for the clinician and also reduces time and money spent on the patient’s transportation. Knowing the reliability, SEM, and MDC values of these outcome measures makes them more trustworthy.
Author contributions
CONCEPTION: Letícia B Calixtre, Danilo H Kamonseki and Germanna M Barbosa.
PERFORMANCE OF WORK: Hilmaynne RF Fialho, Gustavo V Gonçalves, Maycon TM Jales, Letícia B Calixtre, Danilo H Kamonseki and Germanna M Barbosa.
INTERPRETATION OR ANALYSIS OF DATA: Hilmaynne RF Fialho and Letícia B Calixtre.
PREPARATION OF THE MANUSCRIPT: Hilmaynne RF Fialho and Letícia B Calixtre.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Danilo H Kamonseki and Germanna M Barbosa.
SUPERVISION: Letícia B Calixtre, Danilo H Kamonseki and Germanna M Barbosa.
Ethical considerations
The present study was approved by the Human Research Ethics Committee of the Federal University of São Carlos (No. 4.365.562), São Carlos, SP, Brazil. All athletes received explanations about the study and those who agreed to participate signed an online informed consent. The present study is in accordance to the declaration of Helsinki for experiments involving humans.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors would like to acknowledge the athletes who volunteered to participate in this study.
Conflict of interest
The authors have no conflicts of interest to report.