
Abstract
BACKGROUND:
Lumbar radiological abnormalities (LRA) and trunk muscle weakness are major causes of the low back pain (LBP). We reported that the prevalence of LRA was approximately 90% in middle- and heavyweight-judokas, independent to the occurrence of LBP. However, the trunk muscle weakness, especially the rotators, plays a key role in occurrence of LBP in heavyweight judokas.
OBJECTIVE:
To examine the trunk muscle strength (TMS) and LRA impact on LBP occurrence in lightweight judokas.
METHOD:
The strength of the trunk extensors, flexors, and rotators was measured in 32 lightweight male judokas. LBP and LRA were identified using a questionnaire, X-ray, and MRI.
RESULTS:
The occurrence rate of LBP and LRA were 40.6% and 62.5%, respectively, without any significant correlation. Among judokas without LRA, TMS of those with LBP were significantly lower than those without LBP (
CONCLUSION:
Weak trunk musculature may be a co-factor in the occurrence of LBP in lightweight judokas without LRA.
Introduction
Judo is a traditional Japanese grappling martial art and is widely known as an Olympic sport. In competitive settings, judokas are divided into seven weight categories (under 60 kg, 60–66 kg, 66–73 kg, 73–81 kg, 81–90 kg, 90–100 kg, and over 100 kg). Weight category-dependent sport specificity exists between each weight category, such as techniques, speed, strength, flexibility, reaction time, and others. The characteristics of judo-related injuries differ according to body weight, favorite technique, judo history, etc. [1, 2, 3].
In our study regarding ongoing low back pain (LBP), 30%–40% of elite judokas experienced LBP regardless of the weight categories [4]. Although the pathogenesis of LBP is very complicated, trunk muscle weakness is strongly implicated in LBP [5, 6, 7, 8]. Trunk muscle strength (TMS) is an essential component of judo, and muscle weakness may increase the risk of injury [9]. Furthermore, anatomical changes in the lumbar spine detected as lumbar radiological abnormalities (LRA) are another major cause of LBP. A previous study reported a high prevalence of LRA related to LBP in judokas [10].
We have previously reported that LRA occurred in 65.5% of judokas in the lightweight, 90.3% in the middleweight, and 90.9% in the heavyweight categories [4]. LBP accompanied by LRA was observed in 50%, 100%, and 88.9% of judokas in the lightweight, middleweight, and heavyweight categories, respectively. Therefore, almost all LBPs occurring in middle- and heavyweight judokas were accompanied by LRA; however, half of the LBPs in lightweight judokas were not. Therefore, there is a possibility that LBP in lightweight judokas has different characteristics from those in the two heavier weight categories.
Our previous study showed low extension and rotation strength only in the heavyweight category judokas with LBP [11]. However, we did not assess such association of LBP among lightweight judokas. Iwai et al. added LRA as a factor associated with LBP to clarify the relationship between LBP and lower TMS in collegiate wrestlers. Moreover, wrestlers with LBP but no LRA had more severe LBP and lower TMS [12]. The average body weight of these wrestlers was 68.7 kg, which is close to those of lightweight judokas. Therefore, it is vital to evaluate TMS by considering the LRA for LBP in lightweight judokas.
We hypothesized that the relationship between LBP and TMS would become clearer when we limit participants to lightweight judokas without LRA. Therefore, this study aimed to investigate the relationship between LBP and TMS, including rotators in elite lightweight judokas, and to define LBP with or without LRA using a lumbar radiological examination. Moreover, we investigated the correlation between the severity of LBP and TMS to clarify the different relationships between judokas’ LBP and TMS.
Methods
Participants
Approval was obtained from the Ethics Committee of Nippon Sport Science University (009-G002; date of approval: Jan 29, 2010), while the study conformed with the tenets of the Declaration of Helsinki [13]. We recruited all the judokas belonging to the university judo club who could participate in the present study. All participants provided a written informed consent. All participants and their coaches were informed of the purpose and potential risks of the study. The participants were 32 male collegiate lightweight judokas in 60 and 66 kg categories. The participant characteristics are presented in Table 1. All participants practiced judo for 3 hours a day, with two sessions a day, and 6 days a week.
Physical characteristics of 32 male collegiate lightweight judokas consisted of under 60 kg and 66 kg categories
Physical characteristics of 32 male collegiate lightweight judokas consisted of under 60 kg and 66 kg categories
Data are presented as mean
The osaka city university test for LBP severity
LBP, low back pain. LBP is defined as a total of 1 or more points. Modified from Kuroki and Tajima [14].
The presence of LBP was evaluated using a questionnaire developed by Osaka City University (OCU test) modified by Kuroki and Tajima [14]. The OCU test comprises of 10 questions about LBP-related activities of daily living (ADL) (Table 2): lying face up with an extended leg, rising from bed in morning, washing the face in morning, wearing and removing trousers and socks while standing, using a Japanese-style toilet, sitting on a chair, standing, walking, going up and down stairs, and lifting or holding heavy objects. The participants graded each question according to the following criteria: possible without pain (0 points), possible with pain (1 point), and impossible (2 points); consequently, we grouped the judokas into non-LBP and LBP groups when they scored 0 and 1 or more points, respectively [4]. The sum of the points from all 10 items (range 0–20) rated the LBP severity, with a higher value indicating a more severe LBP in the OCU test [12].
Radiological examination
Two experienced orthopedic surgeons examined the plain film radiographs and magnetic resonance imaging (MRI, Hitachi Medical Corporation, Tokyo, Japan) to determine abnormalities of the lumbar vertebrae and intervertebral discs. The radiographic films were obtained with anteroposterior, lateral, and right and left anterior oblique views. MRI was performed with a 0.3-T unit using surface coils with a body coil in the supine position. T2-weighted fast spin-echo was used to obtain sagittal images of the lumbar spine and lumbar intervertebral discs. We modified the definitions of LRA presented by Iwamoto et al. [15] MRI-detected LRA, such as lumbar intervertebral disc degeneration and disc protrusion, were added to the definitions (Table 3) [4]. Some congenital abnormalities, such as transitional vertebra and spina bifida occulta, were excluded because they were not caused by engaging in sports activities. The spinal instability was excluded because it indicated malalignment of the lumbar spine during trunk flexion and extension and not anatomical changes in the lumbar vertebrae. Image assessment to determine the presence of a LRA was independently performed by two orthopedic surgeons without the knowledge of individual LBP status. Disagreements were resolved by consensus between the two orthopedic surgeons in event of a discrepancy in the presence of LRA. LRA was present when an athlete exhibited at least one abnormal finding [4].
Definitions of lumbar radiological abnormalities (LRA)
Definitions of lumbar radiological abnormalities (LRA)
Modified from Iwamoto et al. [15].
A Biodex System 3 dynamometer equipped with Flexion/Extension and torso rotation attachments (Biodex Medical Systems, Inc. Shirley, NY, USA) was used. Peak concentric moments of the trunk extensor, flexor, left rotation, and right rotation muscles were measured at 60, 90, and 120
For measuring extension-flexion cycle of the trunk, the participants were placed in a semi-standing posture with their knees flexed at 15
Statistics
All experimental designs are shown in Fig. 1. Based on the evaluation of LBP, we classified judokas into two groups: the non-LBP group (
We compared the peak moment (PM, in Nm) and their respective ratios between non-LBP and LBP groups, and non-LRA and LRA groups. Subsequently, we compared non-LBP (
The correlations between LBP severity and TMS in judokas with and without LRA were analyzed using Spearman’s rank correlation coefficient (r). LBP severity was calculated from the OCU test scores, which is the sum of the total points related to the ADL (range 0–20, higher the values more severe the LBP). The level of significance was set to 5%. All analyses were performed using IBM SPSS Statistics version 25 (IBM Corporation, Armonk, NY, USA). The effect size (ES) for each parameter was calculated according to Cohen’s d effect sizes (G power, Heinrich-Heine University of Dusseldorf) with 0.2, 0.5, and 0.8 considered small, medium, and large, respectively.
Results
Prevalence and LBP severity
The prevalence of LBP was 40.6% (13/32), and that of non-LBP was 59.4% (19/32) (Table 4). The mean
Prevalence of LBP and LRA in the lightweight judokas
Prevalence of LBP and LRA in the lightweight judokas
LBP, low back pain. LRA, lumbar radiological abnormality. Lightweight, under 60 kg, and 66 kg judokas.
Experimental design.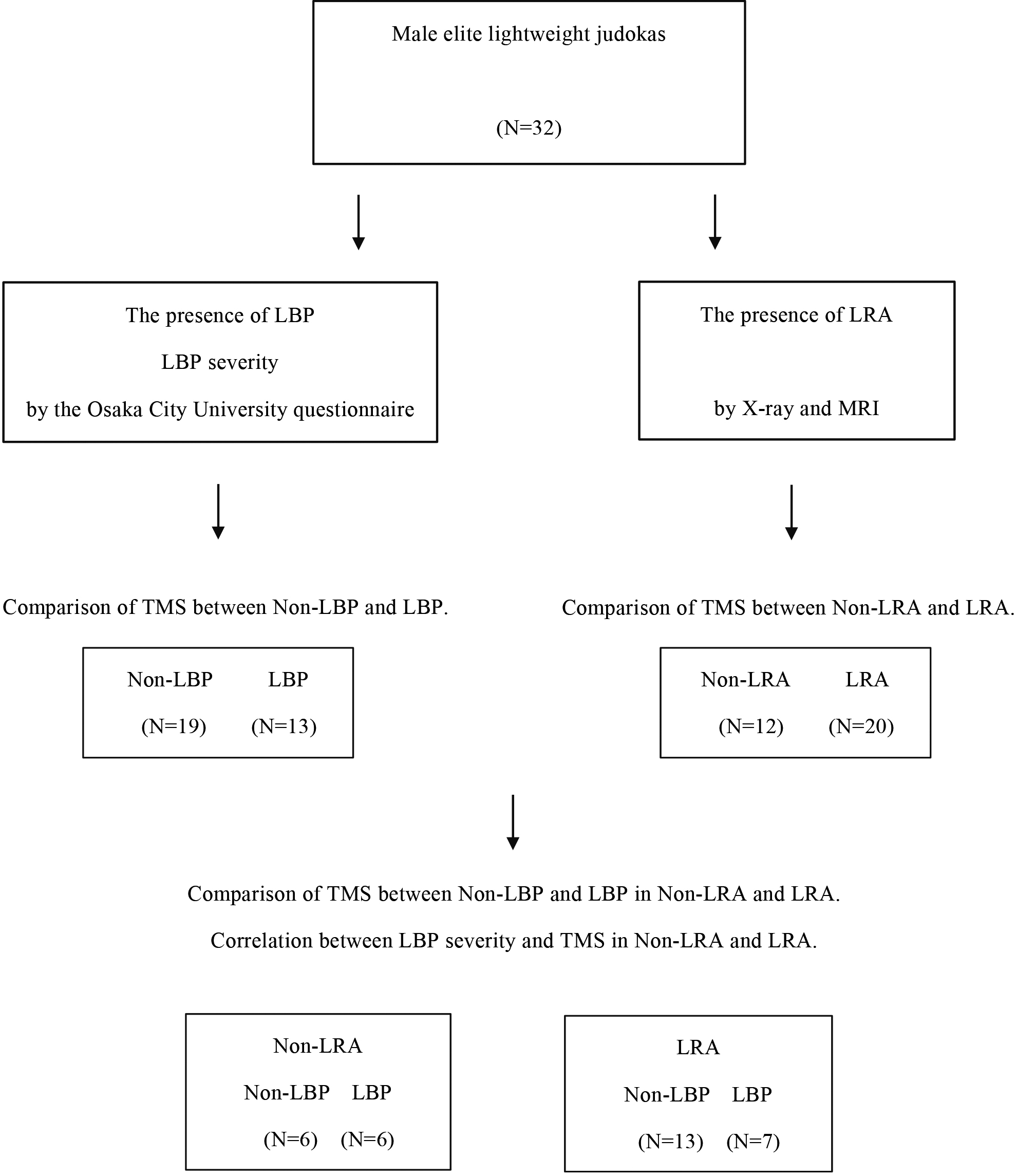
The prevalence of LRA was 62.5% (20/32), and that of non-LRA was 37.5% (12/32) (Table 4). Spondylolysis and lumbar intervertebral disc degeneration were frequently observed, and the prevalence was 40.6% (13/32) and 31.3% (10/32), respectively. Other LRA included balloon disc in 12.5% (4/32), limbus vertebrae in 6.3% (2/32), spurring in 3.1% (1/32), and disc space narrowing in 3.1% (1/32) participants.
Prevalence and LBP severity with and without LRA
The prevalence of LBP in judokas with LRA was 35.0% (7/20), and that of non-LBP – 65.0% (13/22) (Table 4). In judokas without LRA, the prevalence of LBP was 50.0% (6/12), and that of non-LBP – 50.0% (6/12) (Table 4). The LBP severity (score on the OCU test, mean
Comparison of TMS
There was no significant difference in TMS between judokas with and without LBP (Table 5) and between judokas with and without LRA (Table 5).
Comparisons of peak moments of the trunk muscles between the lightweight judokas with and without LBP and LRA
Comparisons of peak moments of the trunk muscles between the lightweight judokas with and without LBP and LRA
Data are presented as mean
Comparisons of peak moments of trunk muscles between the lightweight judokas with and without LBP in those with and without LRA
Data are presented as mean
Correlations between LBP severity and peak moments of the trunk muscles in lightweight judokas with and without LRA
LBP, low back pain. LRA, lumbar radiological abnormality.
However, there were significant differences in TMS between judokas without LRA (Table 6) but not in those with LRA (Table 6). Judokas without LRA had significantly lower TMS than those without LBP (
The correlations between LBP severity (score on the OCU test) and TMS in all judokas and judokas with LRA (Table 7) were negligible and non-significant. In judokas without LRA, there were significant negative correlations between LBP severity (score on the OCU test) and TMS (
Discussion
In our previous study, we reported that almost all middle and heavyweight judokas with LBP, LRA was present in 100% and 88.9% of the participants, respectively [4]. However, no more than 50% of LBP in lightweight judokas was accompanied by LRA [4]. Therefore, in present study, we used lumbar radiological examination to detect LRA and eliminate the influence of LRA on LBP, and to investigate the relationship between LBP and TMS in lightweight judokas. Moreover, participants were categorized as lightweight who did not reveal any LBP factors such as LRA and TMS in our previous studies [4, 11]. Although these factors and experimental procedures may be essential to analyze trunk conditions related to judokas’ LBP, to date no study has examined a relationship between LBP, LRA, and TMS in judokas.
Some moderate correlations were found between LBP and TMS in lightweight judokas without LRA against negligible, at best, correlations in judokas with LRA. Regarding those without LRA, lightweight judokas with LBP had weaker TMS than those without LBP. Significant differences were observed in all directions i.e., extensor, flexor, dominant rotator, and non-dominant rotator of TMS. Moreover, judokas with more severe LBP without LRA exhibited lower TMS, especially for extensors and dominant rotators, while only the dominant/non-dominant rotator ratio demonstrated a significantly lower value with LBP severity. Despite previous conflicting studies [17, 18] an association was found between LBP and TMS due to strict participant selection, namely lightweight judokas, and using the lumbar radiological examination. These results are largely consistent with those reported by Iwai et al. involving wrestlers [12].
The rates of LBP and LRA were 40.6% and 62.5%, respectively, while for judokas with and without LRA, the rates of LBP were 35.0% and 50.0%, respectively. These values are close to those reported in our previous study [4]. Therefore, half of the lightweight judokas’ LBP were not accompanied by LRA. Notably, most middle and heavyweight judokas with LBP have LRA [4]. Judokas take load in their lumbar region from their own and from their opponents’ body weight. Thus, the load on the lumbar region in lightweight judokas should be lower than that in middle-and heavyweight judokas. Moreover, our previous study [11] indicated that the TMS per unit body weight of lighter-weight judokas was higher than that of heavier-weight judokas. These might be associated with a lower prevalence of LRA in lightweight judokas’ than heavier weight judokas. The range 1–5 of LBP severity (score on the OCU test) obtained in the present study ranges from slight LBP with only one painful ADL to LBP with 1/4th of all the ADLs painful. These values indicate the LBP severity at which judokas can continue to practice judo.
Additionally, differences in judo movement can influence the occurrence of LRA. In judo competitions, there are many movements, such as grasping opponents’ judo-gi, which means a competitive jacket and swerving the opponent’s posture. In an offensive situation, judokas use throwing techniques. Moreover, in defensive situations, they react against opponents’ movements and rapidly escape or defend against opponents’ offenses. Furthermore, weight-category-dependent characteristics of activities certainly exist [19, 20]. Lightweight judokas usually move more and faster than heavier-weight judokas [20]. Moreover, their movements are multidirectional and sometimes highly flexible. All these characteristics of lightweight judoka may also be related to the lower prevalence of LRA in lightweight judokas than in heavier weight judokas. Furthermore, the prevalence of lumbar disc intervertebral degeneration and spondylolysis differed between lightweight judokas in the present study and middle and heavy weight judokas in our earlier study. In that study, the prevalence of lumbar intervertebral disc degeneration was overwhelmingly high, and spondylolysis was the next most prevalent LRA in middle and heavy weight judokas [4]. On the other hand, in the present study pertaining to lightweight judokas, lumbar intervertebral disc degeneration (31.3%) was the second most prevalent LRA following spondylolysis (40.6%). Thus, such differences in the order of prevalence of lumbar intervertebral disc degeneration and spondylolysis depending on the weight category certainly exist. This may be associated with the difference in stress on the lumbar region depending on the weight categories.
Lightweight judokas with LBP without LRA had lower TMS in all movement directions, although this was not observed at all moment speeds. On the other hand, those with LRA did not show the same tendency. The ES scores for 60
As an additional finding, lightweight judokas suffering from more severe LBP had lower TMS, especially for the extensor and rotator in the absence of LRA. Iwai et al. investigated the extensor and flexor strength in wrestlers [12]. This previous report confirmed that wrestlers with severe LBP had weak extensors. Moreover, we previously reported that rotator strength was more crucial for judokas than for wrestlers [22]. Taken together, these findings are similar to the results of the present study. We believe that the trunk extensor and rotator are particularly important for judo movements because judokas move their trunk extensionally and rotationally on many occasions. Thus, the relationship between low extension and rotation strength and LBP is more robust in lightweight judokas without LRA. Judokas with LRA might have factors other than TMS that are related to LBP severity.
Asymmetry is considered a factor in sports injuries [23, 24]. The asymmetry in trunk muscle strength is significantly higher on the dominant side than on the non-dominant side, depending on the sports [25]. This may be attributed to asymmetrical differences in movement patterns in sports. Asymmetry of the trunk muscles certainly exists in combat sports, including judo [23]. However, its association with LBP remains unclear. In the present study, we examined trunk rotational strength, which plays an important role, especially in judokas, to determine the laterality of the lumbar region. Only in the judokas without LRA, judokas having LBP showed a significantly lower dominant/non-dominant rotator ratio than that of judokas not having LBP. Moreover, LBP severity in lightweight judokas without LRA was significantly and negatively correlated with dominant rotator strength and dominant/non-dominant rotator ratio. In lightweight judokas without LRA, the weakness of dominant rotator strength has a strong association with LBP severity. However, the dominant/non-dominant rotator ratio was close to 1.0, with more severe LBP; thus, rotational asymmetry was not associated with LBP severity, especially for lightweight judokas without LRA. Instead, the problem may have rested with the weakness of the dominant rotator. For lightweight judokas without LRA, trunk rotational asymmetry depending on strong dominant-rotator strength would not be associated with LBP and would be appropriate to compete in high-level matches. However, this tendency decreased more in judokas with severe LBP. In the present study, we limited participants to lightweight judokas and LRA revealed TMS characteristics of lightweight judokas, whose load to the lumbar region causing LBP were smaller than those of heavier weight categories.
In terms of the limitations to this study, the division of the judokas’ LBP into LRA groups and the focusing on lightweight athletes resulted in a small sample size for each subgroup. Moreover, this was a cross-sectional study and not an intervention study. Thus, it was impossible to decide whether strengthening of the trunk muscles can improve and/or prevent LBP. Additionally, the LRA history could be important, and if it occurred recently, its effect could be more robust.
Conclusion
LRA greatly impacts LBP in almost all judokas although the relationship between low TMS and LBP is more robust in lightweight judokas only in the absence of LRA. Moreover, judokas with a more severe LBP have lower TMS, especially for the extensors and dominant rotator. This tendency may be based on lightweight judokas’ athletic specificity, as they move rapidly and multi-directionally with great flexibility.
Author contributions
CONCEPTION: Takashi Okada, Kazunori Iwai and Koichi Nakazato.
PERFORMANCE OF WORK: Takashi Okada.
INTERPRETATION/ANALYSIS OF DATA: Takashi Okada.
PREPARATION OF MANUSCRIPT: Takashi Okada and Takayoshi Hakkaku.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Kazunori Iwai and Koichi Nakazato.
SUPERVISION: Koichi Nakazato.
Ethical considerations
This study was approved by the Ethics Committee of Nippon Sport Science University (009-G002; date of approval: Jan 29, 2010) and met the conditions of the Helsinki Declaration. All participants provided written informed consent before participating in the study. Furthermore, all participants and their coaches were informed of the purpose, detailed information about the testing procedure, and potential risks of the study.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors thank Yosuke Yamamoto, Professor (Nippon Sport Science University, Faculty of Sport Culture) for his valuable assistance.
Conflict of interest
The authors have no conflicts of interest to report.