
Abstract
BACKGROUND:
The focus of exercises for restoring the imbalance between scapular upward rotator muscles – upper trapezius (UT), serratus anterior (SA), and lower trapezius (LT) – commonly aims to increase SA and LT activities while not increasing UT activity.
OBJECTIVES:
The purpose of this study was to compare the activity of the UT, SA, and LT muscles during scapation and protraction exercises, which are two traditional exercises, and during a newly designed scapular upward rotation (SUR) exercise.
METHODS:
A total of 29 healthy young adult men performed all three exercises with maximum isometric contraction. The electromyographic activities of the UT, SA, and LT were recorded.
RESULTS:
UT demonstrated the highest activity during scapation. SA activity was the lowest during protraction. However, no difference was found in SA activity during the performance of scapation and SUR. The SA/UT ratio was the highest during scapation.
CONCLUSIONS:
SUR is a new exercise that can be performed at moderate intensity for shoulder rehabilitation to restore scapular upward rotator muscle imbalance.
Introduction
Scapular upward rotation (SUR) is one of the three-dimensional movements of the scapula that accompanies elevation of the arm under normal conditions [1, 2]. Muscles primarily involved in the SUR movement include the upper trapezius (UT), serratus anterior (SA), and lower trapezius (LT) [3]. In particular, coordination of these three muscles is essential in maintaining the correct scapulohumeral rhythm during an arm elevation [1, 4, 5]. Because the UT is attached to the lateral 1/3 of the clavicle, its role is to elevate and retract the scapula from the SC joints while elevating the arm [6]. The SA is attached to the ribs from the medial border and inferior angle of the scapulae to link the scapula to the thorax. Therefore, the SA is responsible for the upward rotation and posterior tipping motion of the scapula during an arm elevation [7]. Moreover, because the LT is attached to the spine of the scapula from the spinous process of T6-12, it rotates upwardly and depresses the scapula [8]. Particularly, LT also contributes to the posterior tilt and external rotation of the scapula while elevating the arm [9].
The scapulohumeral rhythm or scapular alignment can be disturbed by various conditions, including muscle fatigue, muscle length alteration, insufficient activation of the scapular muscle [10, 11, 12]. Moreover, an imbalance in muscular activities among these three scapular upward rotator muscles causes certain diseases, such as rotator cuff tendinitis and shoulder impingement syndrome [13, 14, 15, 16]. Sahrmann reported that shoulder pathology and deterioration of scapulohumeral rhythm or scapular alignment may be more associated with muscle activity imbalances rather than scapulothoracic muscle weakness. Although the imbalance of muscle activity cannot be defined as a quantitative ratio or numerical value, the pattern of scapular muscle activity imbalance was previously described. Cools et al. found that LT activity in subjects with shoulder pain due to shoulder impingement during abduction was significantly lower than in normal subjects while the ratio of UT:LT muscle activity was significantly higher than in the latter [14]. Ludewig and Cook found relatively increased UT muscle activity and decreased SA activity in patients with shoulder impingement syndrome compared to healthy controls [13]. As such, shoulder pathology including shoulder impingement syndrome can be caused by an imbalanced muscle activity between reduced SA and LT activity and excessive muscle activity in the UT to compensate for SA and LT [13, 15, 18].
Therefore, several studies have been conducted on exercises to strengthen the SA or LT and restore the coordination or balance among the scapular upward rotators [14, 18, 19, 20]. In addition, studies on exercise that induces high muscle activity in the SA or LT have also been conducted [9, 19, 21]. To strengthen each muscle of the scapular upward rotators, the shoulder shrug motion was used for maximum activity of UT [22]. Shoulder scapation motion is generally used to enhance the muscle strength or induce relatively high muscular activities of the scapular upward rotators including the UT, SA, and LT [8, 19]. To restore balance among scapular upward rotator muscles, scapular protraction and push-up plus are used to induce higher muscle activity in SA relative to other scapular upward rotator muscles [18, 19].
These exercises have been proposed to restore the imbalance among the scapular upward rotators and increase muscle activities of the SA and LT while avoiding the excessive activity of UT [18, 23]. Therefore, exercising without elevating the humerus to more than 90
This study aimed to compare the muscle activity of UT, SA, and LT during two representative exercises used to strengthen SA using a newly designed SUR exercise. In addition, the difference in the SA to UT ratio and LT to UT activation is determined during these exercises. The potential benefit of the SUR exercise is that it is performed in the SUR direction and therefore will have relatively low UT activity as compared to scapation exercises, which require arm elevation in a vertical direction. In addition, since the SUR is performed with an arm raised
Methods
Participants
This study was a cross-sectional research conducted from July 2019 to June 2020. Based on a pilot study, the required sample size was calculated using G*Power 3.1 software (G*Power Software Inc., Kiel, Germany. Based on an effect size of 0.25 an
A total of 29 healthy university students participated in the experiment. All of them were right-handed. Participants in the study had healthy shoulders and completed a self-report to determine the presence of orthopedic or neurological disorder in the shoulder. Moreover, participants had a scapular inferior angle that reached the midline of the axilla when the arm was raised to the maximum [11]. Participants were excluded from this study if the following conditions were observed: (1) a dislocated or traumatic history of the shoulder complex or (2) a history of shoulder surgery within the previous 6 months. All participants received explanations for this study and agreed to participate by signing a consent form. This study was approved by the Yonsei University Wonju Institutional Review Board (approval number: 1041849-201906-BM-097-01).
EMG recording and data processing
The EMG of the UT, SA, and LT was measured using TeleMyo 2400T (Noraxon USA, Inc., Scottsdale, AZ) and analyzed using MyoResearch software (XP Master Edition 1.07; Noraxon USA, Inc.). Before attaching the electrodes, the skin was shaved and gently rubbed with sandpaper to reduce skin impedance. To measure scapular upward rotator muscular activity, one electrode was placed at the upper crest of the shoulder, halfway between the C7 spinous process and the acromion [32]. Another surface electrode was placed to the SA parallel to the muscle fibers, below the axilla, anterior to the latissimus dorsi, and posterior to the pectoralis major [32]. Another electrode was placed next to the medial edge of the scapula at a 55
Experimental procedure
All participants performed all three exercises. During the exercise, UT, SA, LT activities were recorded. During the three exercises, a metronome was used to represent the sound signal. All participants were instructed to practice for 5 min for each exercise to familiarize themselves. Each exercise was repeated three times. Participants maintained each trial for 5 s, 1 min of rest was given between repetitions, and 5 min of rest was given between three exercises to prevent muscle fatigue. These three exercises were performed randomly for each subject, so that the order effect did not occur.
Scapation exercise
Participants were placed in a sitting position with both arms on the side and their thumbs facing the ceiling. The dominant arm performed the scapation up to 120
Protraction exercise
The muscle activity during protraction was measured as suggested by Liebenson. Participants lay on a table and the trunk was straightened. The chest region was fixed using an orthopedic belt to prevent thorax rotation during the protraction exercise; the shoulders were flexed at 90
Participants characteristics
Participants characteristics
Abbreviations: SD, standard deviation.
Electromyographic activation for each exercise
Abbreviations: UT, upper trapezius; SA, serratus anterior; LT, lower trapezius; SCT, scapation; PRT, protraction; SUR, scapular upward rotation.
Shoulder exercises for scapular upward rotator muscles. (a) Scapation. (b) Protraction. (c) Scapular upward rotation.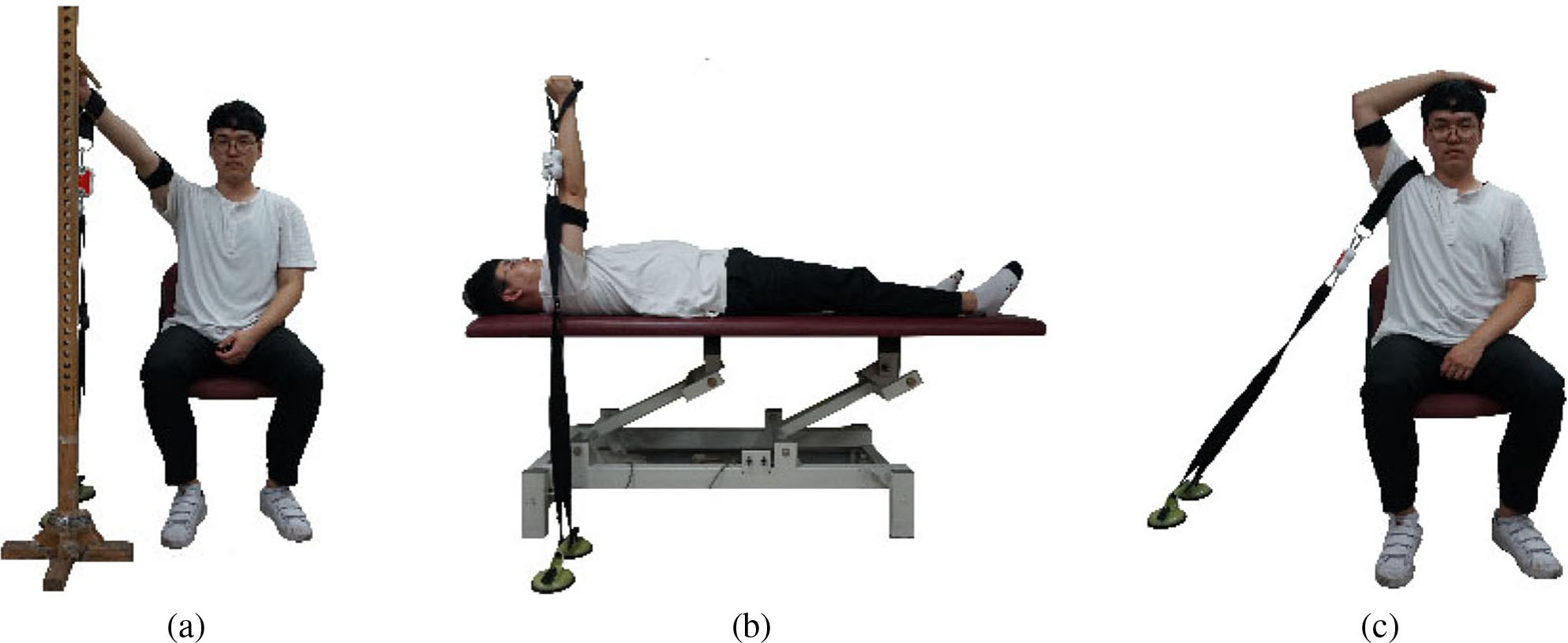
The participant was placed in a sitting position and placed the palm of the dominant hand on the top of head. The scapula was then fixed to the floor using an orthopedic belt. At this time, the angle between the fixed part of the ground and the fixed part of the shoulder was set to 45
Statistical analysis
Variables were normally distributed, as determined by Kolmogorov–Smirnov tests; thus, parametric statistics was used. Data of this study were expressed as mean
Results
Upper trapezius
A significant difference in UT activity was observed among scapation, protraction, and SUR exercises (F (1.758, 49.213)
Multiple comparisons among exercises
Multiple comparisons among exercises
Abbreviations: UT, upper trapezius; SA, serratus anterior; LT, lower trapezius; SCT, scapation; PRT, protraction; SUR, scapular upward rotation.
A significant difference in SA activity was observed during scapation, protraction, and SUR exercises (F (2, 56)
Lower trapezius
A significant difference in the LT muscle activity was observed during the scapation, protraction and SUR exercises (F (1.662, 46.531)
Serratus anterior/upper trapezius activity ratio
A significant difference in the SA/UT muscle activity ratio was observed during scapation, protraction, and SUR exercises (F (1.010, 28.286)
Ratio of muscle activity for each exercise
Ratio of muscle activity for each exercise
Abbreviations: UT, upper trapezius; SA, serratus anterior; LT, lower trapezius; SCT, scapation; PRT, protraction; SUR, scapular upward rotation.
Multiple comparisons among exercises
Abbreviations: UT, upper trapezius; SA, serratus anterior; SCT, scapation; PRT, protraction; SUR, scapular upward rotation.
The LT/UT ratios were not significantly different during the scapation, protraction, and SUR exercises (F (1.107, 30.991)
Discussion
This study investigated the difference in muscle activity of the scapular upward rotators during the scapation, SUR, and protraction exercises. In addition, this is the first study to compare the difference in SA/UT and LT/UT ratios during these three exercises.
Previous studies have shown that humeral elevation angle increases as the UT activity increases, which results in SUR [9]. Moreover, previous studies also reported that as the humerus elevation angle increases, SA activity also increases [9, 36]. Particularly, SA activity is close to maximum at 120–150
The SA/UT ratios of these three exercises were significantly different, and the ratio was highest when performing the protraction exercise. The protraction exercise was designed to induce the relatively higher activity of the SA among the SUR muscles [19, 31]. Martins showed UT/SA ratios of 0.14 and 0.43, respectively, when performing a protraction on stable and unstable surfaces [37]. The values given above are 7.14 and 2.32, respectively, calculated as the SA/UT ratio. In this study, the SA/UT ratio during the protraction exercise was 5.8, i.e SA activity was 5.8 times higher than that of the UT during protraction.
Although the protraction exercise showed the lowest UT muscle activity when compared to SA, this exercise may not sufficiently increase the SA muscle strength. Our study, like previous studies, showed that SA activity showed the minimum activity level for muscle strength enhancement when performing the protraction exercise [9, 21, 29, 30]. Exercises that maximize SA activity were scapation and SUR. However, the ratio of SA/UT muscle activity during scapation was
The LT/UT ratio when performing the scapation, protraction, and SUR exercises was 0.82, 0.90, and 0.56, respectively, in our study; however, no significant difference was noted. Michener et al. investigated the ratio of UT and LT activity to those with normal and subacromial syndrome by performing a scapation exercise with a dumbbell of 1.4–2.3 kg. UT/LT ratios of muscle activity between 90
The important thing to consider in shoulder rehabilitation is not only restoring muscle strength but also coordination among the scapular upward rotator muscles [39, 40]. When the precise coordination between these muscles is achieved, the SUR can be performed correctly during arm elevation [20, 41, 42]. Based on these results, the protraction movement will be a useful exercise for SA muscle strengthening independently in the early stages of symptoms or disease due to excessive UT activation. Moreover, even if LT activity is lower than in the scapation exercise, the SUR can prevent the excessive activity of the UT and promote SA activity to a level similar to the scapation exercise; hence, it may be a useful exercise before performing functional movement such as the scapation.
This study has some limitations. First, only young men participated. Therefore, our results cannot be applied to women or the elderly population. In addition, since this study was conducted on healthy subjects, the type of muscle activity required for patients with shoulder disorders such as rotator cuff tendinitis and shoulder impingement syndrome cannot be determined.
Conclusion
The SUR may be proposed as a new exercise for shoulder rehabilitation related to SUR motion. It is associated with significantly lower UT activity as compared to the scapation exercise, but without significant variation in SA activity. Therefore, during the SUR exercise, the UT/SA activity ratio is significantly higher compared to the scapation exercise. Moreover, SA activity during the SUR exercise is significantly higher compared to that during the protraction exercise contributing to a more effective enhancement of SA strength.
Author contributions
CONCEPTION: Jun-hee Kim and Oh-yun Kwon.
PERFORMANCE OF WORK: Sun-hee Ahn and Gyung-tae Gwak.
INTERPRETATION OR ANALYSIS OF DATA: Ui-jae Hwang and Sung-hoon Jung.
PREPARATION OF THE MANUSCRIPT: All authors.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: all authors.
Ethical considerations
The present study approved by the Institutional Review Board of Yonsei University (Seoul, Korea) (approval no. 1041849-201906-BM-097-01). The study protocol was registered with the Clinical Research information Service (KCT0005050). The participants were then asked to sign a written informed consent. The informed consent was made in two identical copies that the participants could retain one.
Conflict of interest
The authors declare that they have no potential conflicts of interest with respect to the research, authorship, and publication of this article
Funding
None.
Footnotes
Acknowledgments
None.