
Abstract
BACKGROUND:
Abnormal foot mechanics in foot over-pronation has an identified relationship with mechanical low back pain (MLBP).
OBJECTIVE:
To explore the use of short foot exercises (SFEs) as a standalone treatment for MLBP with foot over-pronation.
METHODS:
Forty-six patients with MLBP (PwMLBP) presenting with and foot over-pronation were analyzed. They were randomized into the SFE (short foot exercise), SFE plus traditional physical therapy treatment (SFE
RESULTS:
The CSA of the AbdH and VAS scores improved significantly (
CONCLUSION:
SFEs, with or without TPT may offer an effective treatment for PwMLBP with foot over-pronation.
Keywords
Introduction
Mechanical low back pain (MLBP) is one of the most frequent complaints worlwide. Approximately 60–80% of the general population experiences MLBP at least once in their lives [1]. MLBP is a musculoskeletal back pain that does not include nerve root encroachment or devastating spinal diseases. Its prevalence is profoundly evident in young and active adults and is usually caused by acute traumatic issues as well as additive trauma [2].
Ankle and foot disorders could be recognized as one of the possible etiologies for low back pain (LBP) due to a defect in the kinetic chain that connects the foot with the back. Therapists in rehabilitation fields should shed light on ankle and foot problems, especially when the traditional treatment of LBP fails [3]. Impairment in foot mechanics and functions, such as low-arched and pronated feet have been considered as precipitating factors for developing LBP [4]. The predominance of foot pronation occurs in youth by 48% to 78% [5], while in adults it ranges from 2% to 23% [6]. The hallmark of foot overpronation is the loss or decrease of the medial longitudinal arch (MLA) and is concurrent with diminished ankle dorsiflexion, heel valgus, mild subtalar joint subluxation, forefoot supination, and displacement of the calcaneus laterally. Any disorders that occur in the MLA, such as pes planus and foot overpronation, may contribute to the increased reaction force from the ground to the feet, which consequently predisposes patients to complications such as knee and hip pain, sacroiliac pain, and even LBP [7].
In addition, based on the anatomy trains model, the transfer of energy goes through direct fascial connections that link the muscular structures inside the fascial system. These are four anatomy trains: the superficial back and front lines, the lateral line, and the spiral line. Abnormalities in the MLA or plantar surface of the foot, which consists of the superficial back line, could participate in many foot problems and, as a result, may affect the upper part of the anatomy trains causing tightness of the hamstring muscle, hyperextension of the knee joint, decreased lumbar lordosis and increased cervical lordosis [8].
Furthermore, foot overpronation causes excessive medial rotation of the tibia and hip, tilting of the pelvis anteriorly, and ipsilateral pelvic drop. These changes can lead to mechanical problems in the lower back, resulting in LBP [9]. Abnormal foot mechanics occurring in foot overpronation have an identified relationship with LBP because of increased vertical ground reaction forces, loading rates, diminished ankle dorsiflexion, and increased navicular drop (ND) [10]. A previous study concluded that the ground reaction force (GRF) components were elevated in patients LBP with a pronated foot, as compared to those having only a pronated foot without LBP. The study stated that the increased GRF components in the foot induced a compressive load on the lumbar discs [11]. Many biomechanical problems found in the lower back could have resulted from the overpronated foot; however, without notable effects on the functional level of LBP patients [12].
It was found that weakness of the intrinsic foot muscles leads to the development of foot overpronation measured by ND. The overpronated foot requires either specific passive treatment (orthotics) or active treatment (strength training) [13]. Strength training (short-foot exercises) for intrinsic foot muscles helps to regain the average height of the medial longitudinal arch of the foot and correct ND [14]. A recent study revealed that 6-weeks of short-foot exercises could correct foot overpronation in terms of reduction of pain and ND [15]. Short foot exercises augment the MLA by connecting the head of the first metatarsal bone to the heel without causing excessive toe extension. Additionally, short-foot exercises activate the abductor hallucis muscle, which in turn maintains navicular stability [16]. Little is known about the direct effect of strengthening exercises of short foot exercises (SFEs) in treating MLBP associated with foot overpronation. We hypothesized that SFEs could be used as a standalone treatment in patients experiencing MLBP with foot overpronation. Therefore, the present study investigated whether SFEs can improve MLBP associated with foot overpronation in terms of decreasing MLBP, improving the functional disabilities and the cross-sectional area (CSA) of the abductor hallucis (AbdH) muscle, changing the foot posture, and reducing ND.
Methods
Participants
A total of 76 men, aged between 35 and 60 years, experiencing MLBP [17] with foot overpronation, were referred by an orthopedic specialist. The patients were recruited from Prince Sattam Bin Abdulaziz University Hospital and King Khalid Hospital, Saudi Arabia. They were allocated and randomized into three groups: a control group (CG), short foot exercise group (SFE), and short foot exercises plus traditional physical therapy treatment group (SFE
Participants were included in the study with the following inclusion criteria: (1) pain in the lower back for more than 3 months and scored more than 3 on the visual analog scale (VAS), (2) ND
Flowchart of patient’s dropouts and withdrawals.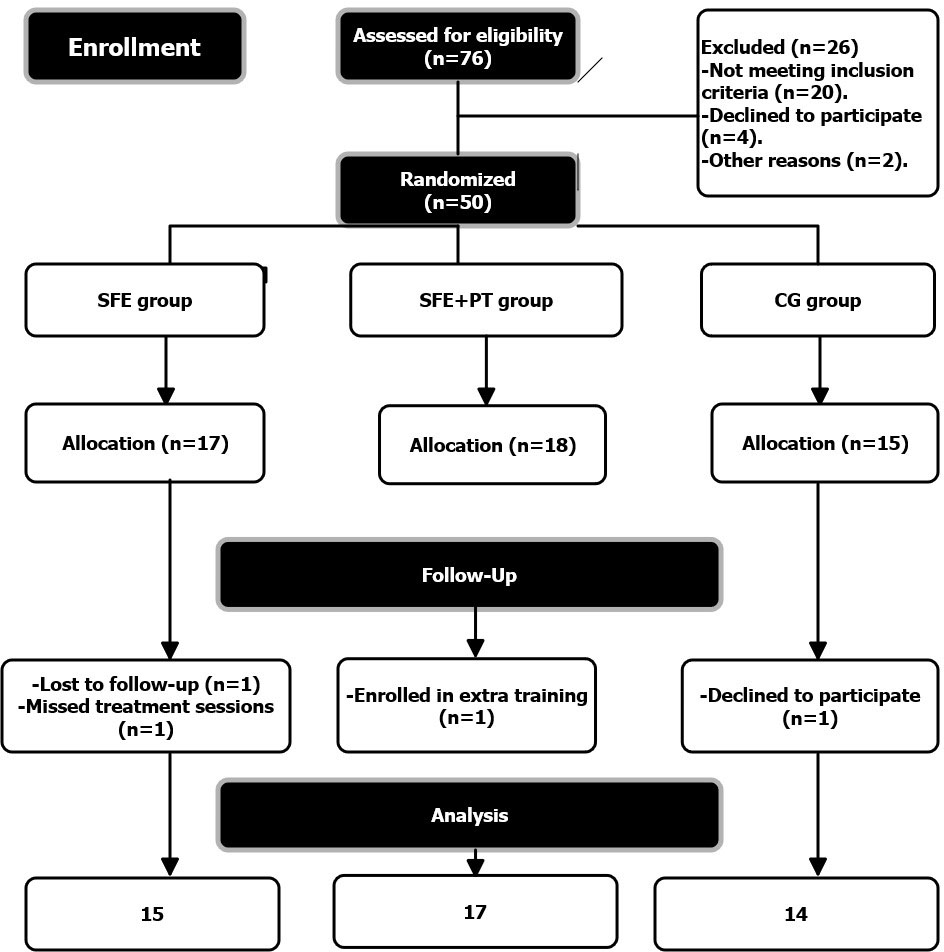
The estimated sample size was based on the calculated effect size in a previous study [23], giving (
This was a randomized, triple-blind controlled trial, following the CONSORT guidelines, conducted between July 2020 and February 2021 with concealed allocation. The study was conducted at the physiotherapy outpatient clinic of the College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Saudi Arabia. Before beginning of the study, details and procedures were described to all participants following the ethics of the Declaration of Helsinki. All patients agreed to participate in the study after signing the consent form. Ethical approval for this study was granted by the Research Ethics Committee (No. RHPT/021/016) of the Health and Rehabilitation Sciences Department, College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Saudi Arabia.
Randomization
Seventy-six MLBP patients were eligible for the study, considering the inclusion criteria. Subsequently, each patient was assigned a number. An assistant researcher, who was not included in the study, performed the randomization process using non-transparent envelopes. Fifty envelopes were arranged, and each patient chose an enclosed envelope to determine whether the patient was allocated randomly to the SFE group (
Study plan
Patients in the SFE and SFE
Assessment procedures
Functional disabilities
The ODI was used to evaluate the functional disability status of patients with MLBP. The questionnaire consisted of 10 questions and six statements for each question. The statement was scored 0 if the patient chose the first statement and scored five if the last statement was checked. If all 10 questions or sections were answered, the overall score was calculated as follows: (gained score/5
Pain score
The MLBP was evaluated using the VAS for pain, which was self-assessed by the patient. The patient expressed his level of pain on the VAS, by placing a perpendicular line at the point that described the pain intensity [19].
Cross-sectional area of AbdH muscle
The AbdH muscle was insonated using an HI Vision Avius ultrasound unit (Hitachi) connected to a L12-5 MHz, 50 mm broadband linear array ultrasound probe. The patient was placed in the supine position. The patient’s knees were in full extension, while the ankle joint was positioned at 90 degrees, and the plantar surface of the foot was rested on a platform to maintain the ankle in a fixed and stable position. Behind the navicular tuberosity, at approximately 1 cm, the ultrasound probe measured the CSA of the AbdH muscle along the muscle borders using a manual tracing technique. To reduce any possible changes in muscle morphology, the probe pressure was maintained at minimum during imaging. The imaging procedures were repeated three times, and the average score was used for the analysis [20, 21].
The FPI-6
The FPI-6 was used to provide a complete and multi-aspect assessment of the foot. The FPI-6 evaluates specific anatomical parts of the forefoot and rearfoot as follows: (i) head of talus palpation, (ii) curvature of the superior and inferior lateral malleolus, (iii) deviation of the calcaneus to inversion/eversion, (iv) bulging of the talonavicular joint, (v) curvature status of the MLA, and (vi) the state of the forefoot and rearfoot in terms of abduction/adduction.
Each patient was screened for six index parts, and the score ranged from
The ND test
At the beginning of the test, a pen dot with a fat marker was placed on the tuberosity of the navicular bone while the patient was sitting (unloaded). The distance from the navicular tuberosity to the ground was measured in millimeters and marked on a piece of paper. The patient was then instructed to stand (loaded), and the distance from the navicular tuberosity to the ground was again identified on the same paper. The difference between the two marks on the piece of paper was calculated. This process was repeated three times, and the average was used for the analysis. A difference
Treatment procedures
SFEs
The SFEs were performed in two stages, each lasting for 3 weeks. First, the patient shortened the foot in the anterior-posterior direction, approximating the head of the metatarsals to the heel, avoiding toes flexion. The patient was placed in a seated position, without loading and was asked to notice an increase in the MLA while performing the exercise. The second stage included an increased level of difficulty using balance loading of three support points (heads of first and second metatarsals and calcaneus). The patient performed the exercises in three different positions: sitting, standing, and half-squat [24]. The exercise in each stage was repeated for 30 repetitions; each repetition lasted for 30-s interrupted with a rest period of rest of 10 s [25]. The SFEs was done daily for 6 weeks. At least two sessions per week were supervised by one of the authors. The patient was kept barefoot while performing the exercises. Both feet received the SFEs in the same session, even if the patient had a unilateral occurrence. However, the examination of outcome measures (ND, FPI-6 score, and the CSA of the AbdH muscle) was obtained from the affected foot only.
The TPT
In the SFE
Non-biomechanical exercises
Non-biomechanical exercises are designed for non-therapeutic effects that cannot induce a substantial change in foot mechanics. These exercises consist of dorsiflexion and plantarflexion of the metatarsophalangeal and ankle joints without resistance, in the unloading position, with the ankle and knee joints at 90 degrees and at full extension, respectively. The non-biomechanical exercises were conducted for 30-s for each exercise, alternating with a 10-s rest between sets, five sets daily, for 6 weeks.
Outcome measures
The functional disabilities and pain level of MLBP patients were measured using the Oswestry Disability Index (ODI) questionnaire and VAS, respectively. Ultrasonography was used to estimate the changes in the CSA of the AbdH muscle (mm
Statistical analysis
All statistical analyses were computed using the IBM SPSS (Statistical Package for Social Sciences (SPSS), Version 23, Chicago, IL). All data are represented as mean
Results
Basic and demographic characteristics
Forty-six patients were analyzed, but 66 feet were investigated (SFE: 22 feet; SFE
Demographic characteristics of all participants
Demographic characteristics of all participants
BMI: Body mass index; Q angle: Quadriceps angle; CI: Confidence interval; Q1: 25
A paired
Changes of ND, FPI, and CSA of AbdH pre- to post-treatment intervention among three groups
Changes of ND, FPI, and CSA of AbdH pre- to post-treatment intervention among three groups
ND: Navicular drop test; FPI: Foot posture index; CSA: Cross-sectional area; AbdH: Abductor Hallucis; CI: Confidence interval;
Changes of VAS and ODI pre- to post-treatment intervention among three groups
VAS: Visual analogue scale; ODI: Oswestry disability index; CI: Confidence interval;
The FPI-6 score improved significantly in the SFE and SFE
Regarding the CSA of the AbdH muscle, patients in the SFE
The pain scores changed significantly among the three groups (
As for the ODI scores, the results revealed that there were significant improvements in patients’ functional abilities among the three groups,
The effect of SFEs alone on dependent variables, inferred by the effect size values
The magnitude of significant differences in the variables of interest resulted from SFEs is presented in Fig. 2. It is to be noted that the effect size for all variables of interest was above 1, which means that SFEs could have a positive impact on correcting foot overpronation and reducing mechanical LBP.
Effect sizes of significant intervention of SFEs; d: Cohen’s d; SFEs: Short foot exercises; AH: Abductor Hallucis muscle.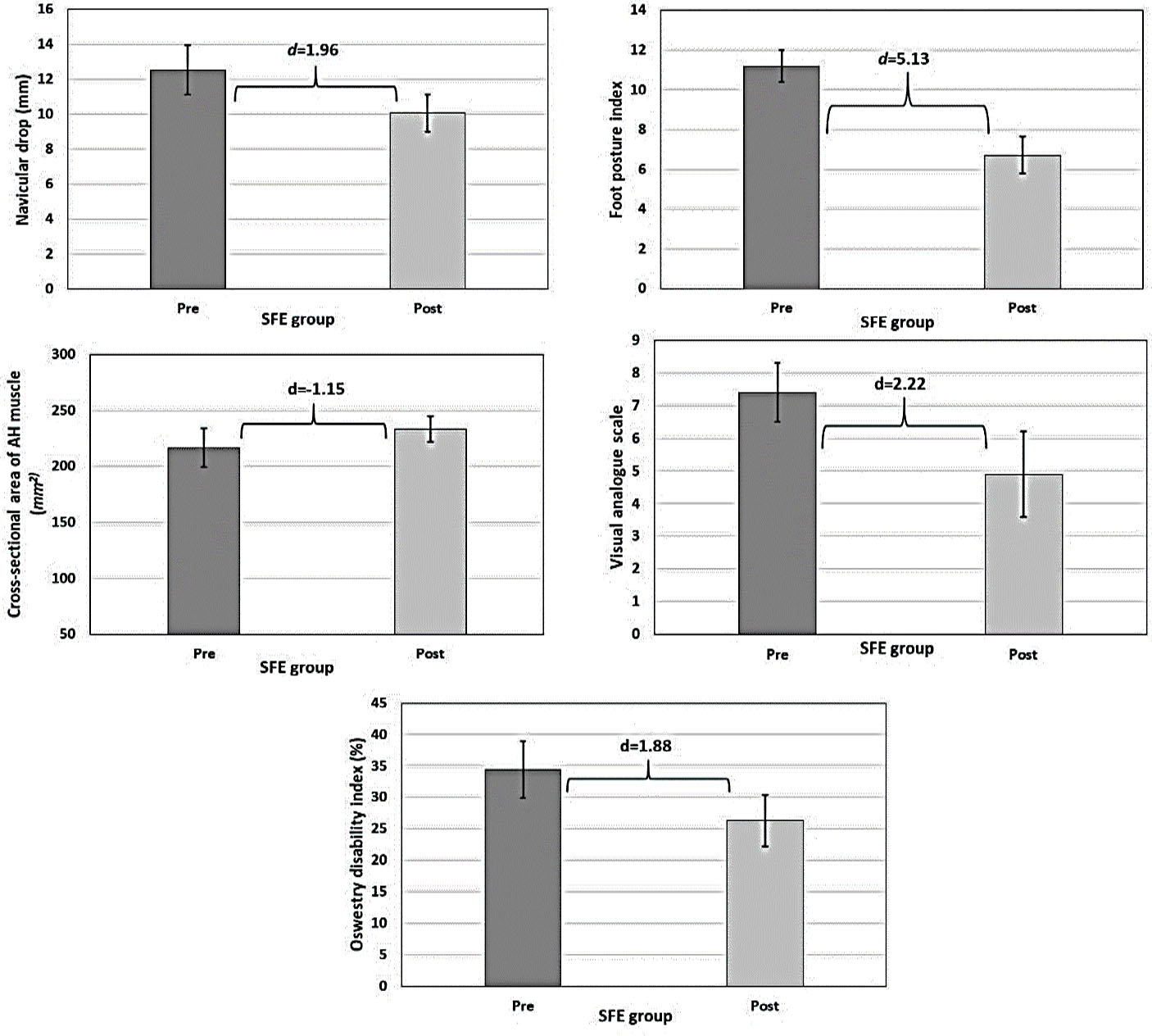
This study aimed to determine the influence of SFEs on patients with MLBP and foot overpronation that is, we intended to determine whether the SFEs could have a noticeable effect on MLBP in addition to its impact on the correction of foot overpronation. Our study reports significant differences in ND and the FPI-6 and ODI scores among the three groups. The ND and the FPI-6, and ODI scores improved significantly in the SFE and SFE
Abnormal morphological structures in pronated feet induce stretched and weakened intrinsic foot muscles by lengthening these muscles behind the resting physiological length. Furthermore, the adverse effect of these abnormal alignments in foot overpronation interrupts the length-tension relationship of intrinsic muscles, consequently decreasing intrinsic muscles’ ability to generate sufficient force [28]. Overpronation of the feet probably induces biomechanical changes in the lower limbs due to the internal rotation of the hip joint [29]. In addition, long-lasting foot overpronation leads to an increase in the exposure of the medial line of the foot to excess pressure, which negatively affects the lumbopelvic region during static and dynamic activities. These disorders of the lumbopelvic region may cause atrophy of the lumbopelvic muscles indirectly [30]. Therefore, ankle and foot exercises could have an apparent effect on the direct correction of foot problems and thus work to improve MLBP indirectly.
The results of the present study indicate that patients in the SFE
According to the integrated kinetic chain paradigm, the myofascial chains transfer loads through muscular pathways, which are connected together, because when the load is applied, the musculoskeletal system demands to become stiff [35]. In this context, Sulowska-Daszyk et al. stated that SFEs could enhance the muscle extensibility of the upper body [36]. Notably, in a previous study, the authors revealed that the tibia was the most adjusting mediator segment in the kinematic chain reaction that occurs during posture alignment and intervention of foot overpronation. It was found that the tibia has a significant influence on pelvic adjustment (change of 2–3 degrees measured at the pelvis) in approximately 40% of cases [37].
Based on the effect size results, it is evident that the SFEs had the ability to improve overpronated feet and reduce MLBP, where all values of the effect size scored above 1. The results of the present study suggest that the application of SFEs for patients experiencing MLBP with foot overpronation might improve muscle strength and power in proximal segments, based on the kinematic chains.
It is well known that the AbdH is a dynamic supporter of the MLA of the foot, helping the peroneus longus muscle to decrease the arch flattening at heel strike and raise the arch to commence the toe-off phase of the gait [38]. The results of the current study show that the SFEs had the ability to significantly increase the thickness of the AbdH muscle, but with a higher percentage in the SFE
Abe et al. reported a correlation between the strength of the short foot muscles and physical performance in terms of walking speed in healthy volunteers [40]. In the current study, the SFE
Since ND is considered a determinant of the medial longitudinal arch status, the ND value contributes an essential part of shock absorption and energy transfer during motion [42]. Moreover, Kendall et al. reported in a previous study that the shock forces elicited during running were transferred to the lumbar region higher in subjects with pronated feet than in supinated feet [43]. The present study reported that the SFEs corrected ND significantly in the SFE (effect size
In the current study, SFEs had a significant effect on correcting foot overpronation as well as reducing MLBP and enhancing functional abilities, as measured by the ODI. The observed results might support that the correction of foot pronation indirectly decreased the anterior pelvic tilt and subsequently LBP. There was a strong correlation between anterior pelvic tilt and the aggravation of LBP [46]. In addition, previous studies suggested that treating foot pronation by the application of foot orthosis could regain the normal alignment of the tibia and femur and improve the properties of the lower limb joints, consequently decreasing the spinal load and LBP [47, 48].
The FPI-6 score was the most important variable of interest that improved because of SFEs in the current study. The FPI-6 score decreased significantly in both the SFE (effect size
The results of the current study show that while decreased pain level (the VAS score) was evident in both the SFE
Limitations
The current study is limited by several factors, which may be controlled in future studies. First, it was conducted on a limited sample size, which needed follow-up investigations. Second, the entire sample selection consisted of males, which was done to prevent the discrepancy of the AbdH muscle size between females and males and possible incorrect explanation of results, but this might affect the generalizability. Third, we did not measure the effect of the SFEs on leg length discrepancy, which might have a role in correcting foot overpronation, especially in cases of unilateral occurrence that correlated with LBP [51].
Conclusion
Based on the clinical findings of the current study, SFEs is effective in the treatment of MLBP patients with foot overpronation. The SFEs may be considered as a standalone treatment in improving the pain and functional disabilities in patients with MLBP, in addition to correcting ND, the FPI-6 score, and the CSA of AbdH muscle in the overpronated foot.
Ethical considerations
Before beginning of the study, details and procedures were described to all participants following the ethics of the Declaration of Helsinki. All patients agreed to participate in the study after signing the consent form. Ethical approval for this study was granted by the Research Ethics Committee (No. RHPT/021/016) of the Health and Rehabilitation Sciences Department, College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Saudi Arabia.
Funding
This publication was supported by the Deanship of Scientific Research at Prince Sattam Bin Abdulaziz University, Alkharj, Saudi Arabia.
Footnotes
Acknowledgments
The author would like to thank and appreciate all subjects who participated in this study for their cooperation.
Conflict of interest
There was no potential conflict of interest in this article.