
Abstract
BACKGROUND:
Handstand is the most important fundamental skill in gymnastics. A gradual and well-balanced increase in muscle loading in a manner is preferred for young beginners and/or recovering gymnasts to safely achieve the muscle strength required to perform a stable handstand.
OBJECTIVE:
To examine upper limb muscle activity during different levels of handstand training positions.
METHODS:
This study utilized four different positions for progressive handstand training; namely, the 90, 135, elbow stand, and handstand positions. The activities of eight upper limb muscles (upper, middle, and lower trapezius; serratus anterior; anterior and middle deltoid; infraspinatus; and latissimus dorsi were measured by surface electromyography (EMG) for each position. The percentages of EMG in each muscle compared to the values during maximum voluntary contraction were calculated and compared between the positions.
RESULTS:
Muscle activity around the shoulder increased gradually throughout the progression of the four handstand training positions. Furthermore, the muscles required for scapular stabilization, such as the upper and middle trapezius and serratus anterior muscles, were activated at levels similar to those for a handstand without performing this movement.
CONCLUSIONS:
A progressive handstand training program of four different positions resulted in gradual and well-balanced increases in muscle activity.
Introduction
The upper extremities withstand considerable forces and moments during gymnasts’ performances [1]. For example, the load on their wrists is up to 16 times their body weight [2]. Consequently, more than 80% of gymnasts experience wrist and/or elbow pain in a season, although they do not always leave out practices or competitions because of pain [2, 3, 4, 5]. Reckless consideration for pain could increase the risk of injury. Young gymnasts are especially likely to experience unique injuries caused by repetitive stress [6, 7, 8]. For example, osteochondritis dissecans (OCD) of the capitellum is one of the most common injuries in gymnasts between 10 and 14 years of age [9]. Therefore, upper limb strength should be sufficiently achieved to ensure the safe performance of gymnastic movements. Just as the muscle strength of the hip joint affects knee and ankle joint kinematics and loading, [10, 11, 12, 13, 14] the muscles of the shoulder joint play a key role in supporting the elbow and wrist joints during handstands.
Handstands are the most important fundamental skill for gymnastics. Furthermore, a stable and straight posture during a handstand is particularly important in competition. During a handstand, balance control is achieved mainly using the wrist and shoulder techniques [15]. Although the wrist is mainly used to stabilize a handstand position on the floor, a more difficult task, such as a handstand on still rings, requires even greater activity of the muscles controlling the shoulder joint [16].
Adult gymnasts demonstrate a more stable handstand than younger gymnasts [17]. Adult gymnasts predominantly use their wrist flexors and anterior deltoid muscles to stabilize their bodies, whereas their young counterparts rely more on wrist and shoulder muscles, which requires complementary activation of the lower body muscles [17].
Therefore, proper muscle strength around the shoulder joint and scapula is required to ensure handstand stability. A gradual and well-balanced increase in muscle loading is preferable for young beginners and/or recovering gymnasts to safely achieve the muscle strength required to perform a stable handstand. Uzunov introduced four progressive stages of handstand training [18], which are widely known in gymnastics worldwide. Although it is generally believed that appropriate muscle stimulation is achieved in this progressive handstand training, the actual muscle activity has not been scientifically investigated.
Thus, this study examined shoulder and scapular muscle activity during different levels of handstand training to test the hypothesis that these different levels result in significant increases in muscle activities.
Methods
Subjects
This study included 13 healthy male volunteers (age: 20.5
Design and protocol
This study utilized the four different postures used as progressive handstand training: (1) The 90 position in which the shoulders were flexed at 90
Four postures of progressive handstand training. (a) The 90 position, in which the shoulders are flexed at 90 degrees with a straight trunk and legs parallel to the ground, with the body supported by hands on the floor and toes on an adjustable level bench. (b) The 135 position, in which the shoulders are flexed at 135 degrees with a straight trunk and legs and the body supported by hands on the floor and toes on the wall. (c) An elbow stand, in which the shoulders are flexed at 180 degrees with elbows bent to place the forearms on the floor. Both hands are put together to form a triangle with both elbows and hands. The body is supported by the forearms and the head, with the foot held by a supporter. (d) Handstand. A full straight handstand against the wall.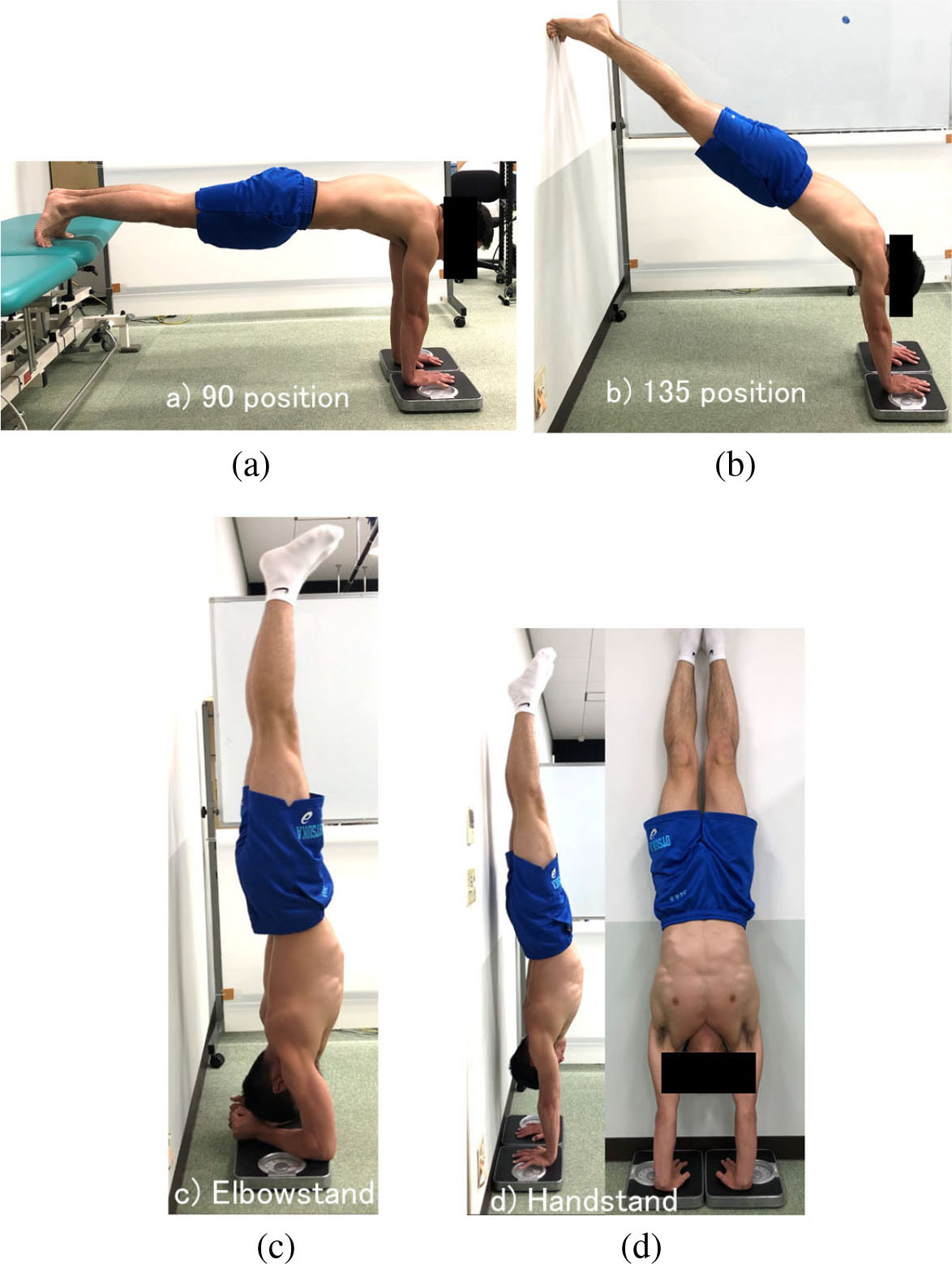
The muscle action potentials on the surface electrodes were measured using a Myosystem 1200 (Noraxon, Arizona, USA). The surface EMGs were set to a sampling frequency of 1000 Hz (Blue Sensor P, P-00-S, Ambu, Ballerup, Denmark). The surface EMG electrodes were applied after wiping the skin with an alcohol cotton, with a distance between the electrodes of 2.5 cm. The placement of the electrodes was determined according to previous studies [19, 20, 21, 22] as follows: UT, at 50% of the line from the acromion to the spine on vertebra C7; MT, at 50% between the medial border of the scapula and the spine, at the level of T3; LT, at 2/3 on the line from the trigonum spinae to the 8th thoracic vertebra; SA, at the muscle belly of the 6th rib; AD, at one finger width distal and anterior to the acromion; MD, from the acromion to the lateral epicondyle of the elbow corresponding to the greatest bulge of the muscle; IS, parallel to and approximately 4 cm below the spine of the scapula on the lateral aspect over the infrascapular fossa; and LD, 4 cm below the inferior tip of the scapula. The amplitudes of the EMG signals were obtained by deriving the root-mean-square of the signal over a 50-millisecond moving window, resulting in a full-wave rectification and smoothing of the raw signal. For statistical comparisons, the normalized and stable waveforms of the central 3 s were selected and the averaged amplitudes were calculated. The measured values were expressed as percentages of the values at the maximum voluntary contraction (MVC) for standardization (%MVC). The MVC was recorded for each muscle. Each contraction was held for 5 s, with maximal effort against manual resistance. The first and last seconds of the EMG data from each MVC trial were discarded; the remaining 3 s of data were used for analysis. The same investigator was responsible for all MVC measurements to ensure test consistency. The MVC evaluations were conducted as previously described, [23, 24] with reported high intraclass correlation coefficients of 0.86–0.99 [25].
Four types of UT, MT, LT, and SA MVC measurements were performed: the participants were seated with their arms fully extended (1), with 135
Muscle activity evaluations for the AD and MD were performed as recommended by Daniels et al for the Manual Muscle Test (MMT); namely, a neutral arm rotation and no movement. The AD was evaluated in the sitting position with the shoulder at 90
IS activity was tested in the sitting position with the shoulder at 0
Muscle activity (%MVC) of each muscle in the four postures of progressive handstand training
Muscle activity (%MVC) of each muscle in the four postures of progressive handstand training
*:
Changes of muscle activity in each posture. UT: upper trapezius, MT: middle trapezius, LT: lower trapezius, SA: serratus anterior, AD: anterior deltoid, MD: middle deltoid, IS: infraspinatus, LD: latissimus dorsi. *: 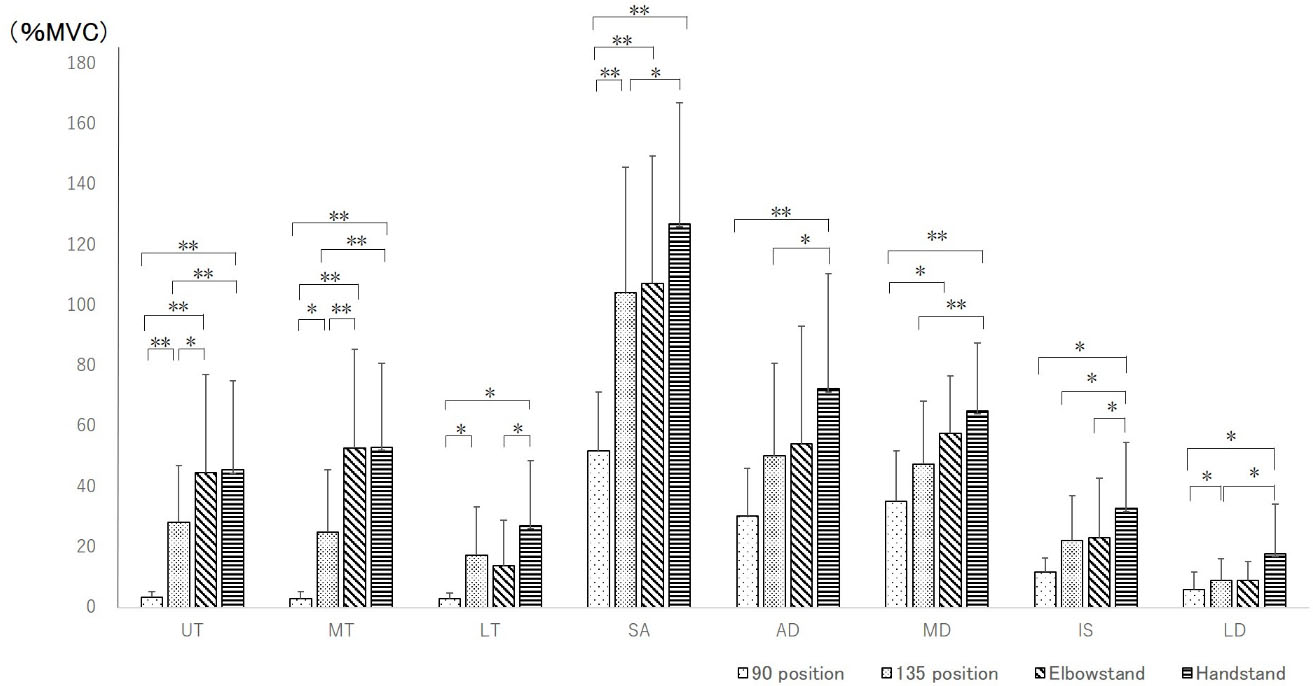
The %MVCs were then evaluated during the four testing positions in random order. The measurements were made with
Because the data were not normally distributed, non-parametric analyses were used. Sample size calculations were performed before the study using G*power 3.1.9 (Heine University, Dusseldorf, Germany). We included 13 men after we calculated the sample size using the software, with an
Results
The results are outlined in Table 1. Muscle activity in the scapular muscles UT, MT, LT, SA, and LD significantly increased from the 90 to the 135
Discussion
The most striking finding of this study was that the muscle activity around the shoulder joint increased gradually with the progression of the four steps of the handstand positions. In addition, different activation patterns were observed among the muscles; that is, the scapular muscles were the first to be activated, followed by the glenohumeral joint muscles. The muscles required for scapular stabilization, such as the trapezius and serratus anterior muscles, were sufficiently stimulated for a handstand without actually performing this movement. Such a muscle activation pattern, from proximal to distal, might be preferable for achieving a stable posture. A well-controlled loading on the shoulder muscles is preferable for young beginner and/or recovering gymnasts to safely achieve the muscle strength required to perform a stable handstand.
Previous studies have measured shoulder muscle activity. Researchers have noted that scapular muscle activity occurs before upper extremity movement to stabilize and position the scapula for glenohumeral elevation [29, 30]. Ekstrom et al. [31] and Hardwick et al. [32] reported that the higher the humerus, the higher was the SA activity [31, 32]. The co-contraction of scapula muscles, such as UT and SA for elevation and upward rotation and the MT and LT for depression and downward rotation, stabilize the scapula for stable glenohumeral movements. High levels of coordination between these functional muscle groups are required during the initial phase of shoulder elevation [33]. Ekstrom et al. [31] demonstrated that the position in which the participants elevated the humerus above the head in line with the LT muscle fibers activated the LT to 97% of the MVC [31]. Overhead upper limb activities induce scapular muscle activation to hold the scapula in an elevated and upwardly rotated position, as observed in gymnasts’ handstand position. Therefore, the scapular muscle shows increased activity with gradually increasing elevation angle. However, the activity increased only in the UT and MT from the 135
The LT and IS showed significantly increased activities from the elbow stand to the handstand. As the LT activity did not increase from the 135
The results of this study suggest two clinical benefits of introducing a stepwise four-position program for a handstand. First, this stepwise program results in gradually increased muscle activity. The scapular stabilizers were stimulated first, followed by the glenohumeral stabilizers. The influence of an unstable scapula on the pathology and dysfunction of the shoulder is well known. The scapula must itself be stable enough to provide a stable base for the glenohumeral joint [37]. Impaired scapular stability increases the risk of pathologies such as impingement or rotator cuff tears [38]. This progressive approach might be beneficial for achieving safe and stable handstands, especially for young gymnasts and/or beginners. In addition, each step of the program can be used to assess the strengths of different stabilizers. Second, this program can be applied for injury prevention and rehabilitation of the upper limbs by practicing handstands in stages. Guadagnoli et al. [39] suggested that the training menu should be adjusted to the skill level of each performer [39]. This stepwise program could help gymnasts safely acquire and achieve a perfectly straight handstand. This program can be used by beginners to achieve a handstand and by injured gymnasts to safely and stably resume performing handstands.
This study has several limitations. First, the participants were limited in number and only male. Females or beginners may show different physical muscle activation for handstand performance. However, the results of this study demonstrated a typical pattern of muscle activity in subjects able to perform a stable handstand, which may be useful in considering other types of physical strategies for a handstand. Second, the proper performance of each posture was determined by visual observation and the angle of the shoulder might have varied between subjects despite the possible effect on muscle activities. However, the difference in shoulder angles in the program was 45
Conclusion
A progressive handstand training program utilizing four different postures showed a gradual increase in muscle activity. The scapular muscles were the first to be activated, followed by the glenohumeral muscles with training progression.
Authors contributions
CONCEPTION: Kazuaki Kinoshita, Yuichi Hoshino and Masashi Hashimoto.
PERFORMANCE OF WORK: All authors.
INTERPRETATION OR ANALYSIS OF DATA: Naoko Yokota, Yuichiro Nishizawa and Noriyuki Kida.
PREPARATION OF THE MANUSCRIPT: Kazuaki Kinoshita, Yuichi Hoshino and Masashi Hashimoto.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: All authors.
SUPERVISION: Kazuaki Kinoshita and Yuichi Hoshino.
Ethical considerations
All the participants understood the purpose of this study and provided informed consent prior to participation according to the ethical standards of the Declaration of Helsinki, and this research was conducted with the approval of Shijonawate Gakuen University Ethics Committee (No. 29-5).
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors would like to thank all the volunteers that participated in this investigation.
Conflict of interest
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.