
Abstract
BACKGROUND:
Hand-held dynamometry (HHD) is used to assess muscle strength in various patient populations, but many variations in protocols exist.
OBJECTIVE:
First, to systematically develop a protocol of HHD for all lower limb muscle groups and evaluate intra-rater reliability; second, to validate HHD with fixed dynamometry for the knee flexor and extensor muscles.
METHODS:
Thirty healthy young adults (women: men – 15:15) participated in two testing sessions. HHD of 12 lower limb muscle groups was performed in both sessions, while fixed dynamometry of knee muscle groups was performed only in the second session.
RESULTS:
The intra-rater reliability of HHD was good for five muscle groups and excellent for seven muscle groups (ICC3,
CONCLUSIONS:
The proposed HHD protocol provides reliable and valid measurements of lower limb muscle isometric strength in healthy adults, which may also be used to test patients with mild muscle strength deficits. However, possible underestimation of absolute strength must be considered when interpreting the results of knee extensors or other large muscles.
Introduction
Skeletal muscle strength assessment is an integral part of clinical examination, goal setting, and treatment planning in patients with musculoskeletal and neurological impairments [1, 2, 3]. Objective quantitative measures of muscle strength, such as fixed and hand-held dynamometry (HHD), are highly sensitive and therefore suitable for evaluation of treatment effectiveness and patient monitoring [4, 5, 6]. HHD proved to be a reliable measure of hamstring strength in athletes with acute hamstring injuries [7]. Its reliability and validity have also been demonstrated for quadriceps muscle in patients after the ACL reconstruction [8]. However, because stronger participants can overpower the tester, HHD may be feasible to measure muscle strength in athletes, mainly in the early stages of recovery from injury or surgical intervention [9].
Since fixed dynamometers are not feasible in certain settings [6], hand-held dynamometers are increasingly used in clinical practice [10]. Compared to fixed dynamometers, they are smaller, cheaper, portable, and easier to use with less time-consuming assessment protocols [11, 12]. However, because fixed dynamometers have been shown to be reliable and valid instruments for assessment of lower limb muscle strength, they are often used as the gold standard reference for other devices [12, 13]. Although HHD is generally reliable and its validity has been previously confirmed by comparisons with isokinetic dynamometry [6, 12, 14], there are many variations in HHD protocols between studies, particularly in relation to patient and tester positions [12]. Other inconsistencies in assessment protocols include, but are not limited to, patient stabilization, lower limb position and muscle activation with respect to gravity, number of measurement trials, rest periods, and use of verbal encouragement [6, 14]. Two testing techniques, i.e. “break” or “make” test, are used, with or without additional stabilization of the dynamometer [14]. Since the majority of previous studies on the reliability of HHD have examined only individual muscle groups [6, 12, 14], there is a lack of systematic and standardized protocols for testing all muscle groups of the lower limbs.
Therefore, the primary aim of our study was to develop a systematic protocol of HHD for all lower limb muscle groups and evaluate its intra-rater reliability in a young, healthy population. The secondary aim was to evaluate the criterion validity of HHD for the knee flexors and extensors by comparing it with fixed dynamometry.
Method
Participants
A convenience sample of 30 healthy young adults was recruited. Inclusion criteria were age between 18 and 25 years and good general health. Participants were excluded if they had a history of injury or current lower limb pain; if they had any existing comorbidities such as neurological, cardiovascular, respiratory, or psychiatric conditions; were pregnant; were professional athletes; or had participated in intensive physical activity in the past 48-h. Participants were asked to avoid any intensive physical activity during the experimental period. The study was approved by the National Medical Ethics Committee of the Republic of Slovenia (0120-48012018/5) before the start of the experiment and was conducted in accordance with the principles outlined in the Helsinki Declaration. All participants gave written informed consent to participate in the study.
Study protocol
Participants attended two testing sessions separated by 2-d. The HHD was performed during both sessions, while the fixed dynamometry was performed only in the second testing session, following the HHD. In order to reduce fatigue and duration of testing sessions [15], only the dominant lower limb of each participant was assessed. A self-reported lower limb used to kick a ball was considered dominant [16]. All measurements were performed by the same tester (physical therapist, female). Before starting the experiments, the tester was familiarized with the protocol and practiced it on six healthy adults who were not included in the study sample.
Hand-held dynamometry
The hand-held dynamometer (Model-01165, Lafa-yette Instrument Company, USA) was used to assess the strength of 12 lower limb muscle groups. The HHD protocol was compiled and performed from protocols used in previous studies using Lafayette or MicroFET dynamometers [3, 9, 15, 17, 18, 19, 20] and the hand-held pull gage [21]. Participants were tested in positions that eliminate the influence of gravity on muscle groups [5].
The test positions used for HHD are shown in Fig. 1 and described in detail in the Appendix. The order of testing the muscle groups was the same for all participants. HHD was performed in four body positions: 1) supine: hip flexors, hip abductors, hip adductors, ankle dorsiflexors, ankle evertors, ankle invertors; 2) prone: hip external rotators, hip internal rotators, knee flexors, ankle plantar flexors; 3) seated: knee extensors; 4) standing on the opposite lower limb with the upper body supported on a table: hip extensors. When necessary, the participant was asked to stabilize his body position by holding onto the long edge of the table, or stabilization was provided by the tester (see Appendix). A belt was used to stabilize the dynamometer for the assessment of the ankle plantar flexors, knee extensors, and hip extensors, in accordance with previous studies [21, 22, 23].
Test positions for HHD of the lower limb muscle groups: Hip flexors (A), hip abductors (B), hip adductors (C), ankle dorsiflexors (D), ankle evertors (E), ankle invertors (F), hip external rotators (G), hip internal rotators (H), knee flexors (I), ankle plantar flexors (J), knee extensors (K), hip extensors (L).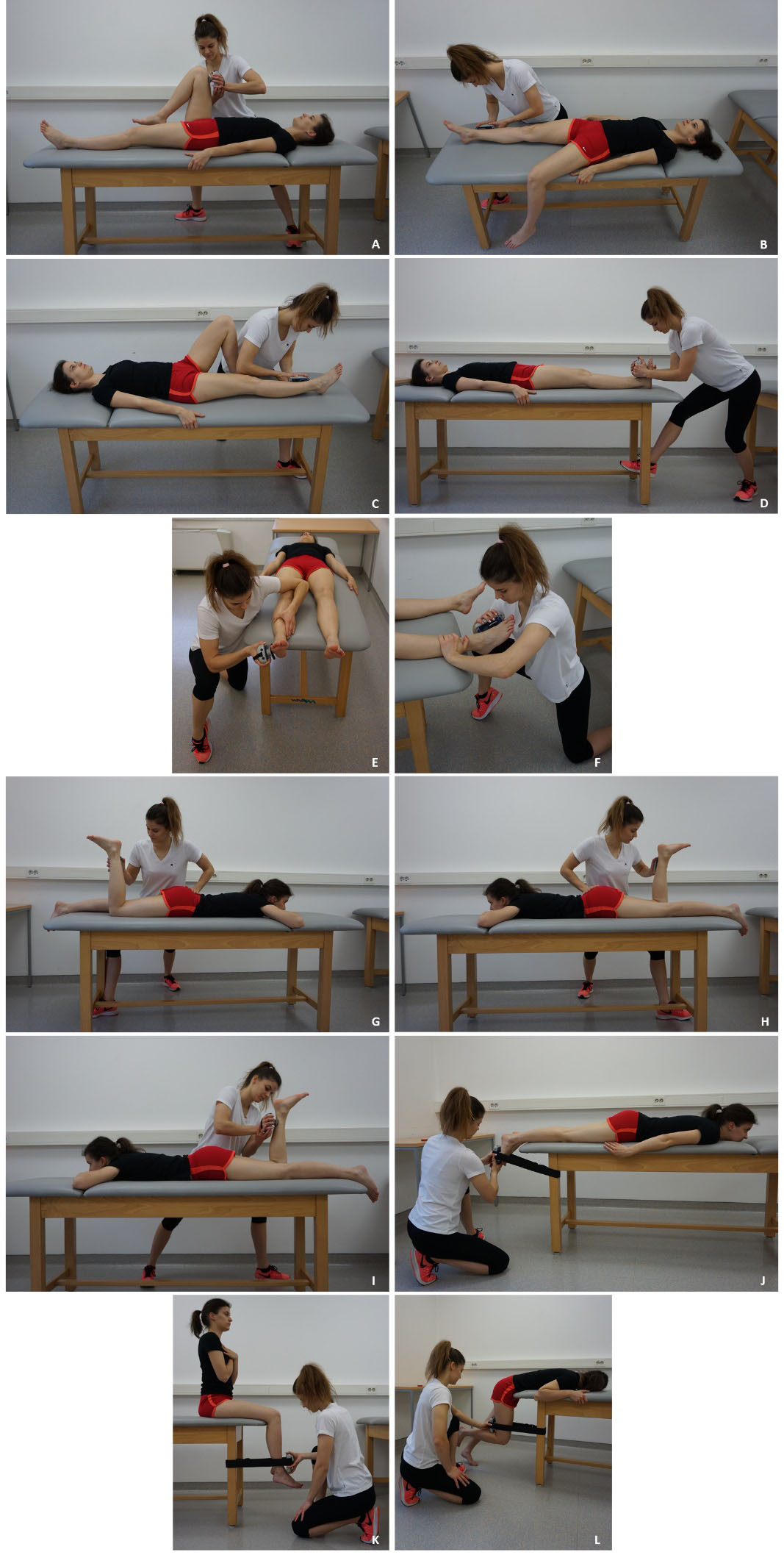
Participant’s position on a fixed dynamometer during measurements of maximal isometric contraction moment of the knee extensors (A) and knee flexors (B) at 90
All measurements were made using a “make” test. The tester held the dynamometer stationary, perpendicular to the tested limb segment, while a participant applied a maximal force against it [6, 24]. The points at which the dynamometer was placed were marked on the participant’s skin with a ballpoint pen prior to testing to ensure consistent positioning between trials of each session. Participants were familiarized with how to perform maximal voluntary isometric contraction (MVIC) in an exercise trial during the assessment of the first muscle group. They were required to produce a maximal force over a period of 2 s and continue their maximal effort for a further 3 s [5, 25]. To initiate the action, the tester said “Contraction!” and then “Maximum! Push, push, push!” as a standardized verbal prompt during all HHD measurements. One exercise trial was performed for each muscle group, followed by two measurement trials. To minimize fatigue effects, a 30-s rest was given between trials of the same muscle group [26]. The peak forces of the two measurement trials were recorded. If the values differed by more than 15% between the two trials, the third trial was performed [27]. In this case, the measurement that differed the most was eliminated. The mean value from two trials was used for further analysis. The duration of the HHD protocol for all 12 muscle groups was approximately 30 min. The same HHD protocol was repeated after 2 d. Between the first and the second session, the tester and the participants had no insight into the measurement results. For validity assessment, the results of the second session were used.
To calculate the moment (Nm) of the knee extensors and flexors, a distance (m) between the lateral knee joint line and the point of force application (center of the hand-held dynamometer pad) of these muscles was measured for HHD. This value was multiplied by a mean muscle force converted from kilograms to newtons to obtain the moment.
The knee flexors and extensors were also studied using an isokinetic dynamometer (Humac NORM, CSMI, USA). Measurements of MVIC moment were performed according to the standard positions described in the CSMI manual [28] using gravity correction. Positions were chosen that were as similar as possible to those used in HHD and which have previously shown good to excellent reliability [29, 30, 31]. The knee extensors were tested in a seated position and the knee flexors in a supine position (Fig. 2). Both muscle groups were tested at 60
Mean peak forces (kg), intra-rater reliability and minimal detectable change for the hand-held dynamometry of all major lower limb muscle groups (calculated for participants of both genders)
Mean peak forces (kg), intra-rater reliability and minimal detectable change for the hand-held dynamometry of all major lower limb muscle groups (calculated for participants of both genders)
CI
The knee extensors were always assessed first, followed by the knee flexors. Participants were given standardized instructions, “On the count of three, push as hard as you can against the lever and maintain that contraction for 4–5 s until I tell you to relax.” Verbal encouragement was given during each trial to ensure maximal effort was achieved. Two exercise trials were performed for each muscle group. The first was performed at the participant’s individual perception of 50% of an MVIC, the second at 75%. Then, the participant performed three maximal trials [29, 30, 31] at a specific knee joint position (60
Estimation of minimal sample size at statistical power level of
Statistical analysis
IBM SPSS Statistics 25 (IBM Corp., Armonk, New York, USA, 2017) was used to perform statistical tests. Intra-rater reliability was estimated using intraclass correlation coefficient (ICC 3,k) with inter-session consistency agreement. The strength of reliability was rated as follows: ICC
Results
Participants were evenly distributed by gender (15 males, 15 females). Their age ranged from 19 to 25 years (mean 21.7; SD 2.4 years), mean height was 174.5 cm (SD 8.9), and mean body mass was 71.8 kg (SD 9.8). All but one participants were right lower limb dominant. All participants attended both testing sessions.
The intra-rater reliability of the HHD was excellent for seven muscle groups and good for five (Table 1). The ICC value was lowest for the plantar flexors and highest for the knee extensors and hip external rotators. The highest MDC was found for the hip extensors and plantar flexors, and the lowest for the hip external rotators, internal rotators and abductors. The strength of the reliability calculated separately for male and female participants was not substantially different from the reliability for all combined (Table 2). For female participants, reliability was lower for two muscle groups (hip extensors and external rotators), and for male participants, reliability was lower for five muscle groups (hip abductors, adductors and internal rotators, knee flexors, ankle invertors).
Comparison of intra-rater reliability of hand-held dynamometry between female and male participants
Comparison of intra-rater reliability of hand-held dynamometry between female and male participants
CI
Relationships between peak moments (Nm) of the knee muscle groups obtained with hand-held and fixed dynamometry
HHD
The criterion validity of HHD for the knee flexors ranged from very good to excellent (Table 3). Correlation with fixed dynamometry was greater when fixed dynamometry was performed at 60
The mean values of the peak moments of the knee flexors (
A systematic protocol of HHD for 12 lower limb muscle groups was developed and its intra-rater reliability evaluated in young healthy subjects. The mean peak forces obtained for four muscle groups were consistent with other studies with comparable testing protocol (hip abductors: 12.5–13.9 kg [15], ankle dorsiflexors: 17.8–27.5 kg [15], ankle evertors: 17.5–22.4 kg [9, 18], ankle invertors 18.5–22 kg [9, 18]), while they were higher for five muscle groups (hip flexors: 15.3 kg [17], hip external rotators:
Intra-rater reliability was good to excellent (ICC
Three muscle groups (plantar flexors, knee extensors, and hip extensors) were assessed with a belt-stabilized hand-held dynamometer. When assessing stronger muscle groups in healthy participants or patients with only minor strength deficits, muscle forces can often exceed those that the tester can resist without movement, thus requiring additional stabilization of the dynamometer [14]. In our participants, the use of a belt to stabilize the dynamometer proved effective and reliable for knee extensors assessment, confirming the results of previous studies [23, 25]. In contrast, the use of a belt did not improve dynamometer stabilization during HHD of plantar flexors. Being one of the strongest muscle groups of the lower limb [35], which generates its force through a longer anatomical lever compared to a lever of external resistance [36], the tester is not able to maintain the ankle in the neutral position [37] and provide sufficient resistance [35] during HHD. Although we used a short and wide belt (see Fig. 1J), ankle movement could not be completely prevented. Excessive joint movement is most likely the cause of the lowest reliability and second highest MDC in this muscle group (see Table 1). The measurement may also be affected by the force of upper limbs resisting sliding of the body on a table in the cranial direction [35]. In the studies by Mentiplay et al. [15, 38], the tester held dynamometer in his hand while leaning his upper arm and body against a wall to increase the resistance and stabilization of the dynamometer. The intra-rater reliability of HHD for the plantar flexors in healthy participants (ICC
Although the intra-rater reliability of HHD was good for the hip extensors, the MDC of these measurements was the greatest. The main problem observed with HHD for these muscles was the inappropriate shape and size of the dynamometer pad for the posterior thigh region. Most of our participants were uncomfortable at the point of contact between the limb and the dynamometer. We hypothesize that the degree of discomfort negatively affected their ability to exert the MVIC moment [14]. Participant effort has previously been cited as a possible factor in reliability [40] and lack of consistency as a possible source of measurement error [41]. Discomfort could be reduced with a modified, belt-stabilized HHD configuration [23] in which the dynamometer is placed against a rigid surface (e.g., a table leg) so that a padded strap is in contact with the participant’s body segment.
For fixed dynamometry of both knee muscle groups, a knee flexion of 90
In contrast to the knee flexors, the criterion validity of HHD for the knee extensors was higher when compared to fixed dynamometry at 90
Degree of criterion validity of HHD was clearly not affected by calculating the mean peak moment from only the first two rather than all three maximal contractions. Therefore, two repetitions of the maximal contraction on a fixed dynamometer are sufficient for comparison with HHD, even though three repetitions are usually performed for accurate determination of MVIC moment [29, 30, 31]. All in all, the HHD protocol for both knee muscle groups used in our study had good to excellent criterion validity while also being practical and not time-consuming.
Some limitations of our study need to be considered. Inter-rater reliability was not evaluated, and the criterion validity of HHD was evaluated only for the knee muscle groups. Because HHD was performed only on the dominant lower limb, possible differences in measurement properties for the nondominant lower limb cannot be excluded. The results of our study were obtained on healthy young adults; therefore, they cannot be generalized to older adults and patient populations with markedly reduced muscle strength.
Conclusions
We developed and evaluated the measurement properties of a new protocol for standardized HHD of 12 lower limb muscle groups. Intra-rater reliability was found to be good for five muscle groups and excellent for seven muscle groups. Criterion validity of HHD was very good to excellent for the knee flexors and good to very good for the knee extensors. This protocol is suitable for testing stronger participants, i.e., healthy adults and may be useful for patients with mild deficits in muscle strength. However, the peak moment values for the knee extensors were significantly underestimated, so absolute muscle strength of knee extensors or other large muscles obtained with HHD should be interpreted with caution. The measurement properties of the proposed HHD protocol need to be determined for different patient populations before its use in clinical practice can be fully endorsed.
Author contributions
CONCEPTION: Tjaša Lipovšek and Urška Puh.
PERFORMANCE OF WORK: Tjaša Lipovšek, Alan Kacin and Urška Puh.
INTERPRETATION OR ANALYSIS OF DATA: Tjaša Lipovšek, Alan Kacin and Urška Puh.
PREPARATION OF THE MANUSCRIPT: Tjaša Lipovšek.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Alan Kacin and Urška Puh.
SUPERVISION: All authors read and approved the final version of the manuscript.
Ethical considerations
The study was approved by the National Medical Ethics Committee of the Republic of Slovenia (0120-48012018/5) before the experiment was started. All participants gave their written informed consent to participate in the study.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.
Appendix: Test positioning,stabilization,and dynamometer pad placements for hand-held dynamometry of lower limb
Muscle group
Test positioning
Dynamometer pad placement
Participant
Tested limb
Tester
Hip flexors
LS, untested lower limb extended; S: holding onto edge of table.
Hip in 90
flexion, knee in relaxed flexion.
Stands on the tested side.
Anterior surface of thigh – two finger widths proximal to the base of the patella (measured with the knee extended).
Hip abductors
LS, untested lower limb abducted with leg hanging off table; S: holding onto edge of table.
Hip neutral, knee extended.
Stands on the tested side.
Lateral surface of the leg – three finger widths proximal to the ankle joint line.
Hip adductors
LS, untested lower limb flexed; S: holding onto edge of table.
Stands on the untested side.
Medial surface of the leg – three finger widths proximal to the ankle joint line.
Ankle dorsiflexors
LS, untested lower limb extended, heels on a table; S: holding onto edge of table.
Hip neutral, knee extended, ankle neutral.
Stands at the tested foot.
Dorsal surface of the foot – between the cuneiforms and metatarsophalangeal joints.
Ankle evertors
LS, untested lower limb extended, feet across a table; S: holding onto edge of table.
Hip neutral, knee extended, ankle in relaxed
Lunge at the tested foot; S: manually stabilizing leg medially.
Lateral side of the foot – below the head of the 5th metatarsal.
Ankle invertors
plantar flexion.
Lunge at the tested foot; S: manually stabilizing leg laterally.
Medial side of the foot – below the head of the 1st metatarsal.
Hip external rotators
LP, untested lower limb extended, hands under chin.
Hip neutral, knee in 90
Stands on the untested side; S: manual stabilization of the pelvis.
Medial surface of the leg – three finger widths proximal to the ankle joint line.
Hip internal rotators
Stands on the tested side; S: manual stabilization of the pelvis.
Lateral surface of the leg – three finger widths proximal to the ankle joint line.
Knee flexors
Stands on the tested side.
Posterior surface of the leg – three finger widths proximal to the ankle joint line.
Ankle plantar flexors
LP, untested lower limb extended, feet across a table; S: holding onto edge of table.
Hip neutral, knee extended, ankle neutral.
Kneeling at the tested foot.
Plantar side of the foot – metatarsal heads. B: around the leg of a table and dynamometer.
Knee extensors
Sitting upright on the edge of the table, feet not touching the floor, arms crossed in front of the chest.
Hip and knee in 90
Kneeling in front of a participant.
Anterior surface of the leg – three finger widths proximal to the ankle joint line. B: around the leg of a table and dynamometer.
Hip extensors
Prone standing (upper body supported on table), knee of untested lower limb extended with forefoot on floor; S: holding onto edge of table.
Kneeling on the tested side.
Posterior surface of the thigh – as close as possible to the posterior knee joint line. B: around the leg of a table and dynamometer.