
Abstract
BACKGROUND:
Some recovery strategies are needed to reduce or eliminate the effect of negative symptoms caused by exercise.
OBJECTIVE:
The aim of this study was to determine the effect of different types of recovery after single-bout strength exercises on biomarkers of muscle damage, cytokine release and lactate elimination.
METHODS:
Following familiarization, 10 male volunteers performed four randomized recovery protocols (passive or active recovery with or without compression garments) following a single bout of resistance exercise (squat and deadlift exercises). The blood creatine kinase (CK), lactate dehydrogenase (LDH), interleukine-6 (IL-6), and tumor necrosis factor-alfa (TNF-
RESULTS:
The CK analysis showed that all protocols significantly increased (
CONCLUSIONS:
Active recovery is an effective method for reducing the severity and duration of muscle damage and for accelerating the clearance of blood lactate (BLa) following a single bout of strength training. There is no added benefit of using compression garments.
Introduction
Unusually high-intensity exercise can cause pain in the working muscles that can be felt in almost the whole body on the next day. This type of pain seen peripherally in working muscles is defined as “Delayed Onset Muscle Soreness” (DOMS). The idea of muscle injury in working muscles after exercise was first described by Hough in 1902 [1] and, since then, the physiological mechanisms responsible for the DOMS phenomenon have been investigated. The extent of DOMS depends on exercise habits, and the duration, type and intensity of exercise. Possible mechanisms of DOMS include micro-ruptures and traumas after concentric and eccentric loads (especially eccentric) in the “Z-line” region of the skeletal muscle [2, 3]. The amount of tension per motor unit increases with these micro tears (as a result of the decrease in the activity of the active motor unit, which is stimulated during the eccentric contraction) at the same time. In addition, stretching during eccentric contractions and prolongation of the muscle length cause an increase in sarcomere damage, and this increased mechanical damage can lead to increases in the level of inflammation [4]. Increased inflammation has the potential to increase the degree of damage to the muscle [5].
Some recovery strategies are needed to reduce or eliminate the effect of these negative symptoms caused by exercise. It is important to determine the optimal recovery strategy for relieving DOMS in terms of successive performances. Numerous methods have been suggested to enhance recovery including active-passive recovery, compression garments, electro-myo-stimulation (EMS), use of anti-inflammatory drugs, massage, stretching, cryotherapy (cold modal application), hot-cold water immersion, and hyperbaric oxygen therapy [6, 7]. Among these types of recovery, it is not clear what the optimal strategy may be when the goal is to relieve DOMS and inflammation levels after resistance training. To our knowledge, there are no studies investigating the effect of different types of recovery on muscle damage and cytokine release after resistance training. Determining the optimal type of recovery strategy to reduce muscle damage and inflammation is of academic interest but would also have important practical application for coaches and athletes.
Although active and passive recovery is a common recovery strategy in the literature, there is no consensus on the optimal approach [8]. The preferred mode of active recovery is often aerobic exercise, such as running and cycling, at 30–60% of maximal heart rate [9]. Providing adequate blood flow to the fatigued muscle, is thought to be the most critical precursor of recovery [10]. Proper application of the duration and intensity of active recovery will increase the blood supply and facilitate PCr resynthesis in the muscle. Indeed, it has been reported that recovery can be optimized by removing H
While active recovery has been widely used by coaches and athletes for many years, recently there has been increased focus on alternative recovery strategies. Nowadays, many professional and recreational athletes also use compression garments to delay fatigue or recover more quickly. However, while compression garments have been used clinically for the treatment of chronic inflammation disorders [3], it remains uncertain whether such garments influence DOMS and inflammation levels following resistance exercise training [6, 11].
Compression garments have been shown to be capable of narrowing the area susceptible to swelling, bleeding and hematoma formation and to have the potential to provide mechanical support. In addition, compression garments are thought to have the potential to blunt inflammatory responses following soft tissue injury caused by acute exercise [12]. The possible effects of compression garments have been studied, especially for long-haul flights, and significant reductions in venous thrombo-embolism have been reported in patients wearing compression knee socks [13, 14, 15]. In sports, a possible efficacious mechanism of action of compression garments is an improved capillary filtration and increased venous return due to compression of the superficial veins [16]. It has been suggested that these possible mechanisms may have similar effects to active recovery such as helping to remove metabolites and shortening the time to for blood gases to return to normal [17]. At the same time, the use of compression garments after strenuous exercise is thought to reduce/narrow the areas of edema and accumulation of fluids due to the exertion of external pressure [6]. To date, the number of studies using compression garments as a means of recovery has been limited and the results have been equivocal [6, 18, 19].
Therefore, it is important to determine if compression garments will influence DOMS, inflammation and lactate elimination. In general, previous studies have only investigated the use of compression garments as an independent recovery strategy. Furthermore, the majority of researches have focused on some specific sport branches such as after marathon and rugby match [18, 20], only after eccentric contraction [18, 21, 22], and limited recovery strategies [23]. Thus, there is a need to focus on the effectiveness of both compression garments on their own and the use of compression garments together with other effective (active) recovery strategies on especially general exercise participants. To the best knowledge of the authors, the use of compression garment with different recovery strategies after single-bout resistance training has not been examined. Therefore, the aim of this study was to determine the effect of different types of recovery after single-bout strength exercises on muscle damage, cytokine release and lactate elimination. It was hypothesized that an active recovery strategy and wearing compression garments would promote a reduced severity and duration of muscle soreness and inflammation also, accelerate the clearance of blood lactate.
Methods
Participants
The sample of this study consisted of 10 male volunteers who did not attend any regular training programs. They were 21.1
Determination of 1 repetition maximum
Biometric measurements of volunteers were conducted in the first week of the study. After 48 h, the acclimation phase was started and the volunteers were given 3 training phases to get used to strength training (squat and deadlift) at 48-h intervals. In order to determine the initial exercise loads of the volunteers, 1 repetition maximum (1 RM) for the squat and deadlift movement was determined for each volunteer 48 h after the acclimation phase ended and one week before the main study began.
The maximum amount of weight that each volunteer could handle in 6 repetition maximum (6 RM) was determined. During each exercise, the volunteer was asked to perform 6 RM with the weight they estimated they could lift. They were asked to repeat the exercise by adding 2.5–5 kg according to the perceived difficulty level. In this way, the maximum amount of weight that they could lift 6 times was recorded as 6 RM of the volunteer. The bar grip for squat and deadlift was determined based on the National Strength and Conditioning Association criteria (NSCA, with hands held a little wider than shoulder width and in closed pronated grip). Volunteers were asked to do flexion movement with optimal range of motion for squat, complete extension of the knee joint in their starting position, with their legs parallel to the floor (80–90
Determining Maximum Heart Rate (MHR) and Target Heart Rate (THR)
In order to determine the individual THR of the volunteers during active recovery, MHR was calculated with the formula developed by Tanaka et al. [26]. Volunteers’ resting heart rate (RHR) was measured with a chest band polar watch (Polar V800, Electro OY, Kempele/Finland) as soon as they got up in the morning on three different days and the average of three different measurements was used as a base. THR values developed by Karvonen (1957) were calculated using MHR and RHR values obtained [27].
Recovery protocols
In the study, four different recovery protocols were applied and a resting interval of 15 days was allowed between each protocol for volunteers to return to baseline.
Protocol 1 (Prot-1): Passive recovery was applied after single-bout strength exercise (all volunteers were seated for 30 minutes without any intervention).
Protocol 2 (Prot-2): Before the single-bout strength exercise, the volunteers put on compression garments, performed strength exercise and, after exercise, passive recovery was applied (all volunteers were seated for 30 minutes in compression garments).
Protocol 3 (Prot-3): After single-bout strength exercise, 30 minutes of active recovery was applied to volunteers at a low tempo. Active recovery was applied with 50% MHR for each volunteer. All volunteers adjusted their speed and pace using a heart rate monitor (Polar V800 GPS, Finland).
Protocol 4 (Prot-4): Before the single-bout strength exercise, the volunteers put on compression garments and performed strength exercise. After the exercise, 30 minutes of active recovery was applied at a low tempo. Active recovery with compression garments was applied with 50% MHR for each volunteer. All volunteers adjusted their speed and pace using a heart rate monitor (Polar V800 GPS, Finland).
Single-bout strength exercise protocol
Volunteers were given a general warm-up (jogging, cycling, etc.) for the targeted muscle groups for 5 minutes before all protocols and specific warm-up to rehearse the target exercises for 5 minutes. After general and specific warm-up, squat and deadlift movements were performed as two different strength exercises in all protocols. Olympic bars were used for both exercises (Eleiko, Halmstad, Sweden). For squat and deadlift, the hands were positioned slightly wider than the shoulder width (1.5 times the acromion) and with a pronated closed grip. Participants were asked to go below the knee level in the lateral view of the hip in order to standardize the depth of the squat during exercise. Deadlift was asked to be done in a neutral posture with the bar on the ground, a flat back and a full extension of the hips during the lift (180
Collection of blood samples
Reference baseline blood measurements were taken from the volunteers before the study (1 month earlier). Volunteers who had a difference of greater than 5–10% of the baseline blood measurement values before each protocol were re-evaluated after waiting for the difference to fall below 5–10%. In addition, reference baseline measurements were taken to determine whether volunteers were exposed to a stimulus that could cause any muscle damage or inflammation during the study.
Biochemical parameters were analyzed at Inonu University Turgut Ozal Medical Center Clinical Biochemistry Laboratory. All blood collection procedures were performed by an experienced nurse. Blood samples were taken by venous puncture method between 09.00–11.00 am and put into biochemistry tubes and delivered in cold chain to the laboratory for analysis. Blood samples were centrifuged at 4000 rpm for 10 min and blood cells were separated from serum. From the serum obtained, TNF-
CK and LDH (U/L): CK and LDH were measured using the Abott brand C 16000 model instrument with the spectrophotometric method [(Abott Park, IL 60064, USA; intra-assay Coefficient Variance (CV)
TNF-
Blood lactate measurement
In order to determine the effects of different recovery types on blood lactate concentration after single-bout strength exercise, 50
CK profile measurements mean 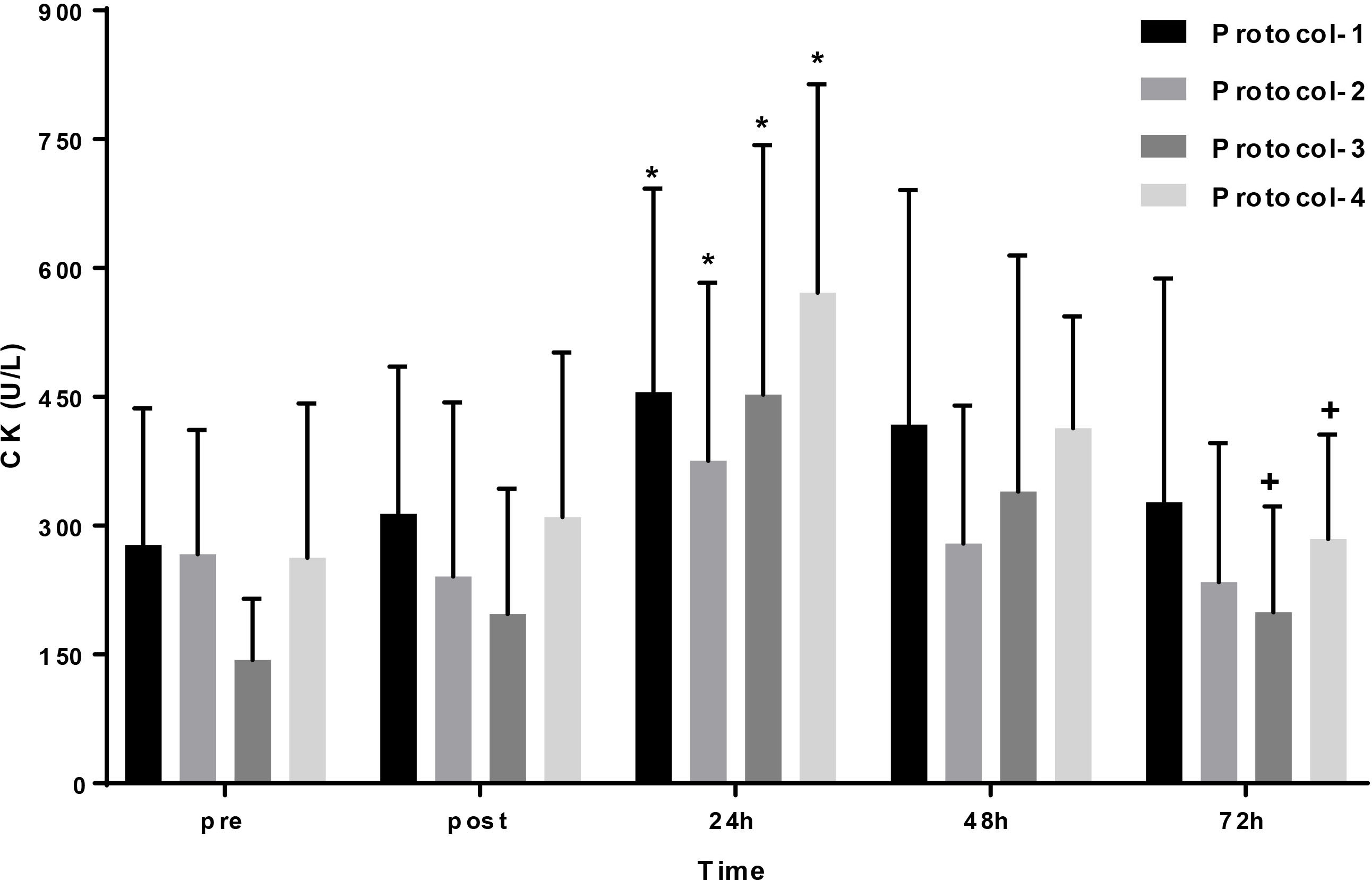
The pressure applied by the compression garments to the body generally exceeds the average capillary pressure (24 mmHg), and lower limb compression of 20–35 mmHg leads to an increase in venous blood flow; however, even lower pressures (15 mmHg) can also provide effective clinical results [28, 29]. Therefore, in the study, considering the individual characteristics of all volunteers (after measurement of ankle, calf, and knee widths), each participant was fitted with “Mediven Dougment Series CCL2” compression stockings with a pressure of 23–32 mmHg, at the specific thigh level (Medi GmbH, Bayreuth, Germany).
Statistical analysis
The data were analyzed using SPSS 23 software. Normal distribution of the data was tested using the Shapiro-Wilk normality test. As a result of the normality analysis, BLa, CK, and LDH showed normal distribution (
Results
All volunteers recruited completed all assessments performed in the research. Examination of the CK data revealed a main effect for time (
Analysis of the LDH data showed no effect for time (
LDH profile measurements mean 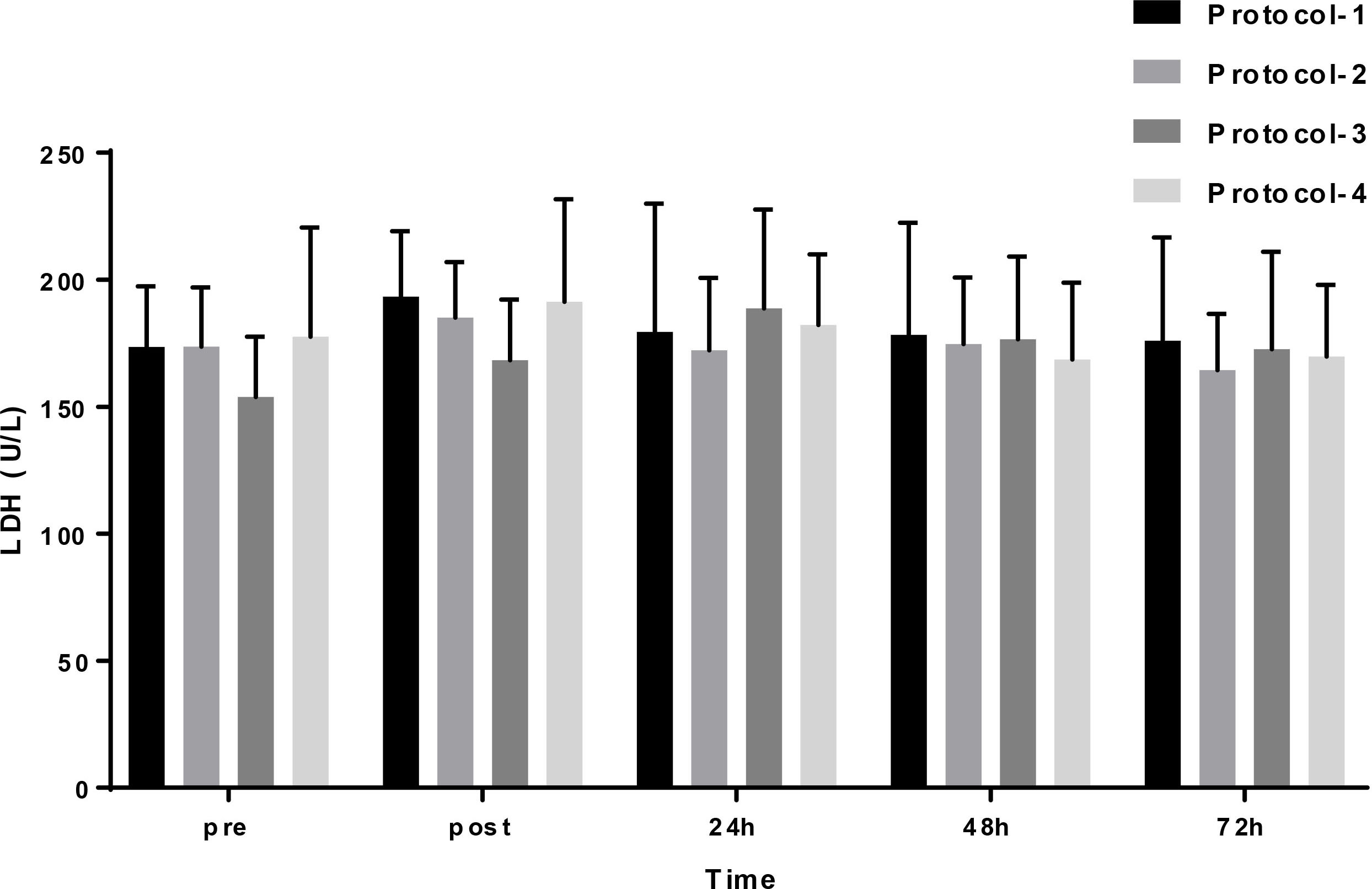
IL-6 profile measurements mean 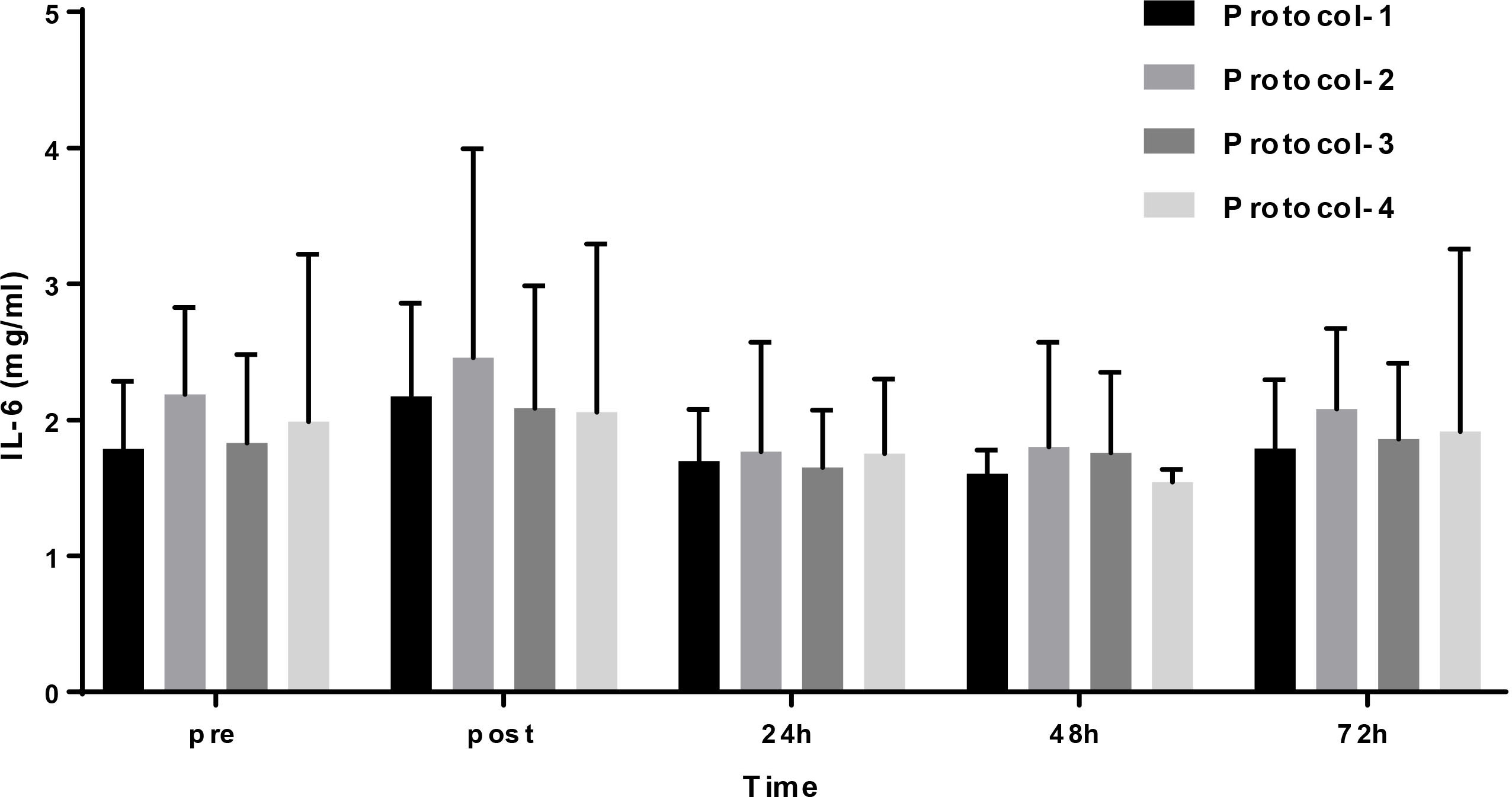
TNF profile measurements mean 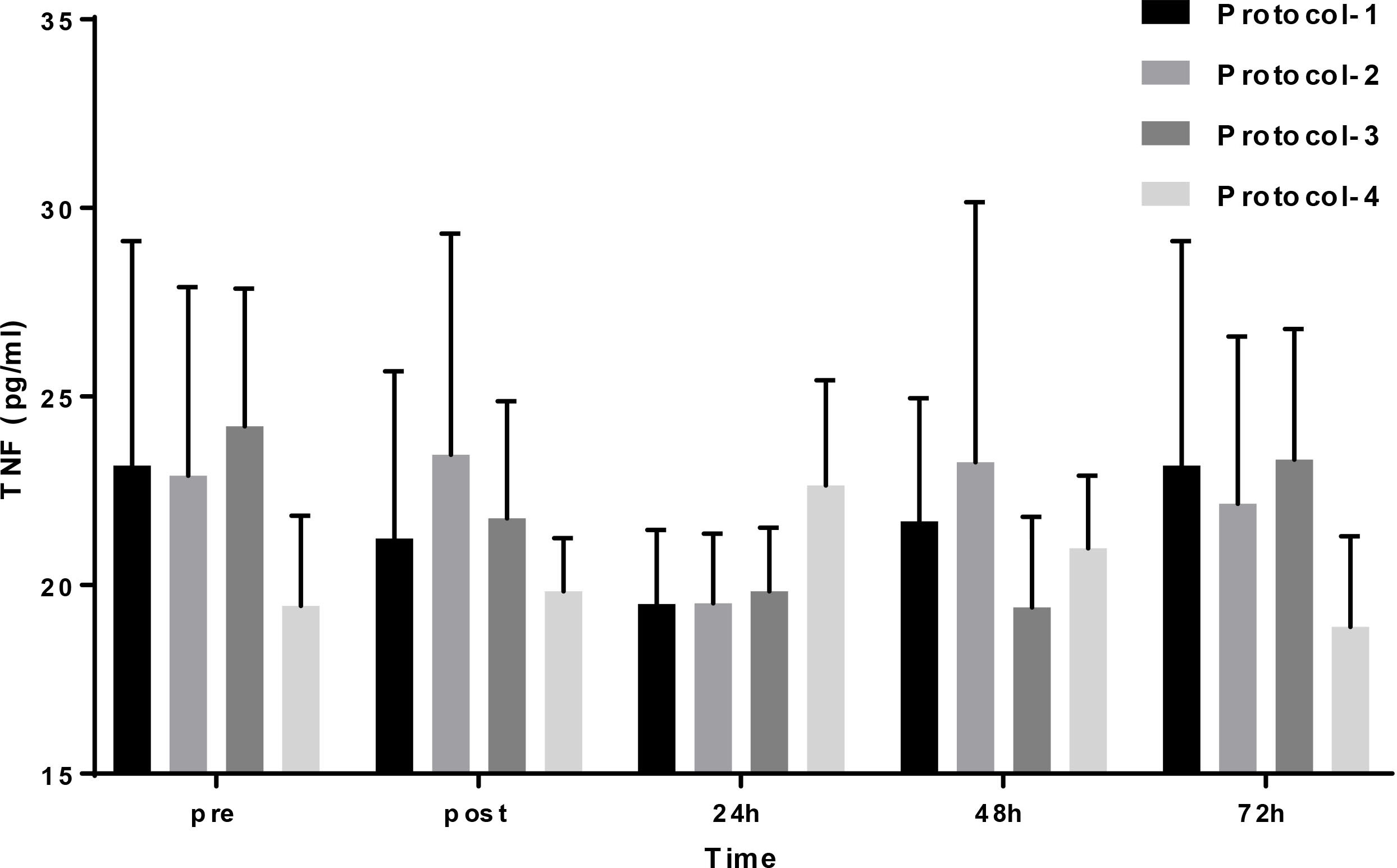
Examination of the BLa data revealed a main effect for time (
BLa profile measurements mean 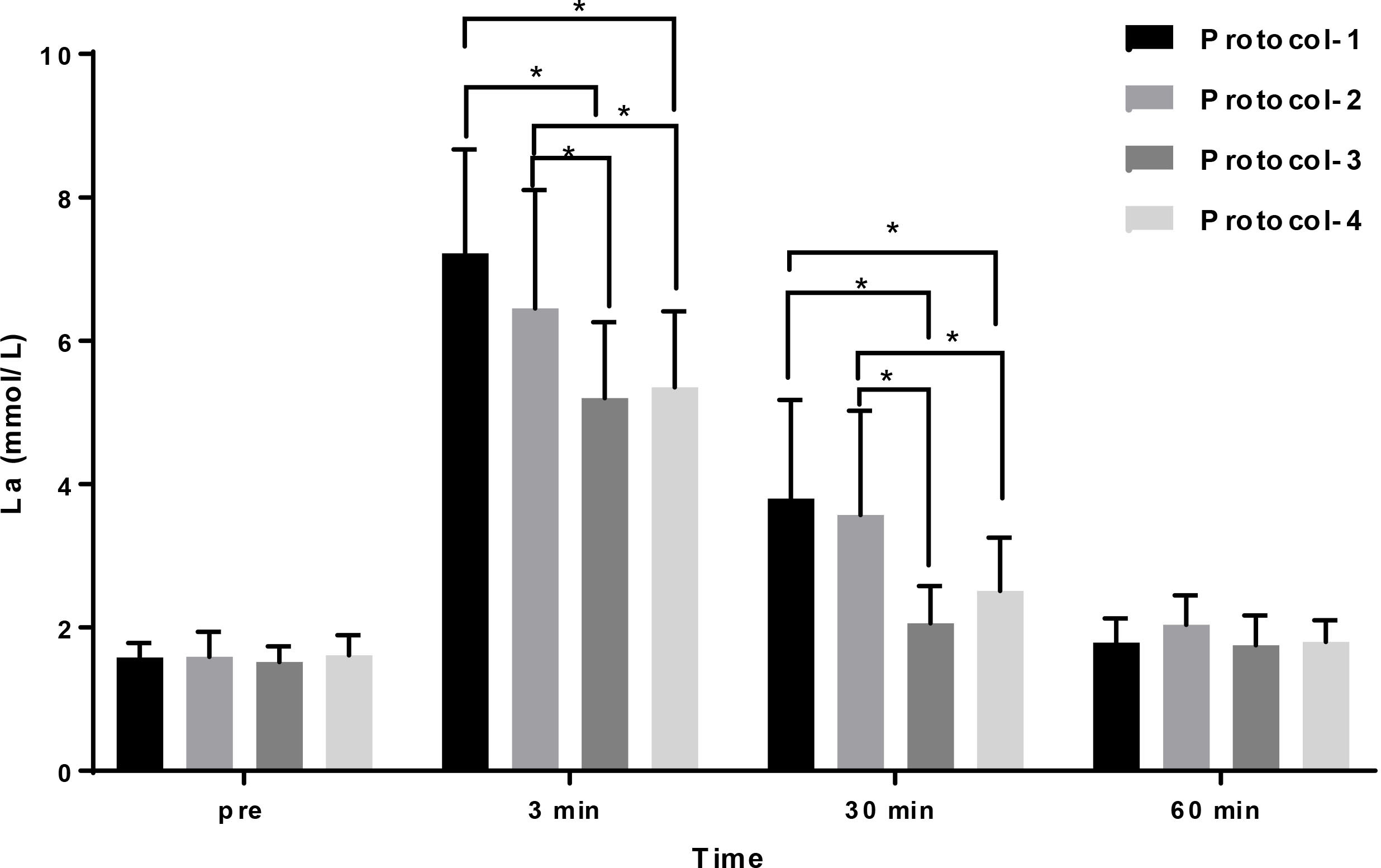
To our knowledge, this is the first study to determine the effects of different recovery strategies in combination with compression garments on biomarkers of muscle damage and inflammation after a single strength training session. It was hypothesized that an active recovery strategy would promote a reduce severity and duration of muscle damage and inflammation also, accelerate the clearance of BLa. The main finding of this study was that CK concentrations and BLa clearence were lower active recovery compared with passive or wearing compression garments recovery strategies. We also found a significance decrease in CK within 24 h and a faster decrease after 48 h in active recovery protocol compared to the other recovery protocols (
When the literature is reviewed, post-exercise muscle damage or pain is often experienced by individuals after strenuous exercise. Although the causes of this muscle injury are not known, uncommon exercises and myofibril injuries caused by eccentric contraction are frequently suggested to be possible causes [35]. In addition, as a rational mechanism of muscle damage, it is known that mechanical trauma in skeletal muscle results in the development of structural damage and inflammation [2]. In this context, the most prominent plasma markers of structural damage to muscle are accepted as enzyme concentrations such as CK and LDH [19]. It is emphasized that some soreness and inflammation after resistance training may be important for skeletal muscle development and structural regeneration. However, a delayed or prolonged muscle pain may negatively affect both professional athletes and health-conscious exercise participants. Negative effects of DOMS include transient decrease in muscle strength, decrease in potential to produce force, swelling and pain [21, 22]. It has been reported that muscle pain after exercise peaks within 24–48 h and then begins to decline [19]. Therefore, although it depends on factors such as exercise type, duration and intensity, it is accepted that muscle pain increases significantly after 24 h.
In a study where Gill et al. [17] applied different recovery strategies to rugby players after a match, they reported that after 84 h, active recovery had the highest recovery rate (88%), compression garments and cold-water immersion had a similar effect (84.4% and 85% respectively) and that passive recovery was the worst recovery strategy (39%). In another study, Kraemer et al. [19] found that the use of compression garments rather than normal garments after high intensity exercise leads to decreases in CK values [19]. These results in a contrast with our finding that found the use of compression garments was not effective compared to active recovery for reducing the CK concentration [12, 17]. When the possible mechanisms of compression garments are examined, their potential to improve peripheral circulation and venous return, remove blood lactate, and clear CK-like muscle damage markers seems clear [19, 36, 37]. Although many studies have investigated the use of compression garments as a sporting performance and exercise/post-match recovery strategy, their effectiveness is still controversial. The ongoing debate on the effectiveness of compression garments is thought to be due to variables such as different methodologies used in studies, sample sizes and diversity of subjects, and exercise modality, duration and intensity.
However, this positive finding for CK in our study was not obtained for other parameters (LDH, TNF, IL-6). Kraemer et al. [19] found that compression garments used after maximal eccentric exercise did not affect LDH release and downgrade time [19]. Similarly, Friden et al., [4] used compression garments as a recovery strategy after eccentric and concentric exercises and reported that there was no significant difference in LDH responses [4]. The results of the present study are consistent with these earlier reports. Also, in a study by Kim et al. [21], the use of compression garments after eccentric exercise was reported to affect neither IL-6 nor TNF-
Another main finding of the study is that active recovery has the potential to influence the rate of lactate elimination. In this study, it was found that active recovery is an effective methodology for removal of lactate consistently with previous researches [42, 43]. When the effect of active recovery on BLa elimination is examined, it is seen that there are some possible physiological mechanisms. Possible mechanisms for this include faster removal of deoxygenated blood, optimization of muscle oxygen utilization, increases in the rate of conversion of lactate to energy [39, 40], and the potential for improvement of peripheral circulation and venous return with active recovery [19]. Also, in our study, we did not find any significant influence of wearing compression garments on removal lactate. In a study conducted by Berry et al. [39], it was reported that the use of compression garments increased lactate elimination after cycling training with maximal effort [42]. However, Duffield et al. [22] found that the use of compression garments did not affect lactate elimination after high intensity training [23]. Similarly, in a study by Trennell et al. [40], it was reported that wearing compression garments had little effect on lactate elimination [40]. Previous studies investigating the potential for metabolite removal via compression garments after training or competition have produced inconsistent results. The lack of consistency with previous findings might be related to differences in training intensity used in the research, along with differences in participants’ lactate levels during and post-training.
There are some limitations in this study. The study sample consisted of small group and male only volunteers who were exposed to moderate intensity resistance training protocol. Higher training intensities could potentially highlight the importance of using different recovery strategies. Thus, further studies are needed to investigate the effects of the use of different recovery strategies with different gender (female), larger sample size, and with different training types and intensity levels.
Conclusion
Active recovery can be used as an effective method to reduce the severity and duration of DOMs symptoms and to accelerate the clearance of BLa. Coaches and athletes can opt for active recovery as an effective means to shorten recovery time after high intensity training and matches. However, the use of compression garments with active recovery seems not to offer any additional benefit.
Author contributions
CONCEPTION: Fatma Beyza Şahin, Armağan Kafkas and M. Emin Kafkas.
PERFORMANCE OF WORK: Fatma Beyza Şahin, Armağan Kafkas and M. Emin Kafkas.
INTERPRETATION OR ANALYSIS OF DATA: Fatma Beyza Şahin, Armağan Kafkas, M. Emin Kafkas, Mehmet Çağatay Taşkapan and Andrew Mark Jones.
PREPARATION OF THE MANUSCRIPT: Fatma Beyza Şahin, Armağan Kafkas, M. Emin Kafkas, Mehmet Çağatay Taşkapan and Andrew Mark Jones.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Fatma Beyza Şahin, Armağan Kafkas, M. Emin Kafkas, Mehmet Çağatay Taşkapan and Andrew Mark Jones.
SUPERVISION: M. Emin Kafkas and Andrew Mark Jones.
Ethical considerations
This study was approved by the Ethics Committee of Inonu University (2017/28) and met the conditions of the Helsinki Declaration. The procedures, conditions, benefits and risks of the study were explained verbally and all participants signed informed-consent forms.
Funding
This research was supported by Inonu University, Scientific Research Project Unit, with the project number TYL-2017-808.
Footnotes
Acknowledgments
The authors thank the volunteers for their commitment throughout the completion of this study. Also, the authors thank Inonu University Scientific Research Projects Unit for supporting this research (the project number TYL-2017-808).
Conflict of interest
The authors have no conflicts of interest to report.