
Abstract
BACKGROUND:
In order to guide sports active subjects with musculoskeletal (MSK) shoulder dysfunctions it is essential to have precise insights of possible weak links in the kinetic chain of their shoulder girdle with access to reference data. Equally, it is uncertain whether so-called functional shoulder strength tests are complementary to an isokinetic shoulder strength test.
OBJECTIVE:
To establish reference values and to clarify the relationship between two upper extremity field tests – the Scapular Muscle Endurance test (SME) and the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) and the isokinetic strength test of the shoulder internal (IR) and external rotators (ER).
METHODS:
Seventy-six male sport active men performed the CKCUEST, the SME, and underwent a bilateral isokinetic strength test to establish reference values of the isokinetic shoulder relative to body mass Peak Moment (PM/kg) and Power (Power/kg) for the IR and ER. A mixed-design ANOVA calculated possible side-to-side differences and one-way ANOVA was applied for eventually age group differences. Additionally, the relationship between the three tests was examined with a Spearman rank-order correlation coefficient.
RESULTS:
No significant correlations were indicated between the SME and the criterion isokinetic test and between the SME and CKCUEST.
CONCLUSIONS:
The main outcome parameters in this study warrant individual assessment as they measure different constructs, leading to a diverse profile of the shoulder.
Introduction
Shoulder pain (SP) is a matter of concern within the working [1, 2, 3] and general population [4, 5, 6]. This is shown by an increasing overall 1-year prevalence of chronic SP in the general population between the years 1994 and 2004 (46.7%–55.2%) [4]. Smaller percentages (2.28%; 15.7%) were observed in UK [6] and Norwegian [5] population indicating international differences and highly varying prevalence numbers. These percentages seem also in line with an active working male population showing a 1-year prevalence and incidence of acute SP around 16.2% [3] and 10.4% [1]. These percentages can be extended for the 1-year incidence of overall chronic SP in the French active working population [2].
Anthropometric data of the subjects (
76) all displayed in (Median and (Interquartile range))
Anthropometric data of the subjects (
Abbreviations: BMI, body mass index; PA, physical activity.
These numbers stress the importance of including future interventions to reduce the incidence of chronic SP at work within an active population [1, 2]. The interest of applying interventions to cope with chronic musculoskeletal (MSK) SP is increasing in order to avoid chronicity. Especially, chronic SP is mostly associated with increased disability at work or during leisure time, higher pain levels at 6 months, increased sick leave and increased medical consumption [5, 7].
For individualized interventions, several factors have to be taken into account since there is a positive association between SP at work and the following factors: age, high perceived physical exertion, work with arms above shoulder level [1], forceful effort and job demand [2]. From a prospective cohort study during 6 months within Dutch general practices 35%, 24% and 41% of the patients presented with respectively acute, sub-acute and chronic SP. Perceived causes of SP reported by the patient were mostly overuse and to a lesser extent trauma events [7]. Despite the detection of previously stated associated factors, the true mechanism of several shoulder pathology causing SP are not yet fully understood [1, 2, 5, 7, 8]. Moreover, for a subgroup of patients with SP with tear of supraspinatus, pain intensity is not a sensitive factor, rather, it is decreased external rotation (ER) PM/kg (Peak Moment) measured isokinetically [9]. Although patients with subacromial impingement show a decreased strength of the (IR) and ER on their affected side [10], the results vary depending on the isokinetic shoulder strength protocol [11]. A recent systematic review [12] has indicated that the supine isokinetic protocol has a relatively small measurement error [13] and is reliable [12].
In addition to shoulder strength testing, Physical Performance Tests (PPT) have become increasingly popular [14, 15]. They also have the advantage of being mainly multi-joint [31] and thus more functional than the isokinetic shoulder IR and ER test. The Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) seems to discriminate for subacromial impingement syndrome [16], but this evidence is still not confirmed as there are conflicting reports [17]. Limited but promising evidence exists also with regard to another functional PPT of the posterior kinetic chain, the Scapular Muscle Endurance test (SME), which may discriminate between chronic SP and asymptomatic subjects [18] and subacromial impingement syndrome [19]. Some reviews have proposed the CKCUEST as one of the more researched PPTs to measure functional performance of the shoulder [14, 20]. Another review discourages their use as single ‘best’ test to predict or screen for SP in an active population [21]. Hence there is a tendency to combine several PPTs [22, 23] since applied as a single PPT they still do not have sufficient measurement properties to guarantee their use in determining return to play or work [14]. Lastly, the relationship between the two previously mentioned PPTs and the golden standard isokinetic shoulder rotational strength [20, 24] is still uncertain except for the CKCUEST where two studies have already shown high to moderate correlations [25, 26] with the isokinetic shoulder IR and ER PM.
Thus the main objective of this study was to provide grouped age reference data for the isokinetic shoulder IR and ER strength and Power, but also for the 2 PPTs within sports active individuals and their inter correlations.
Participants
The sample of this study consisted of 76 men in active duty aged 20–55 years who were tested over a time interval of one year and a half starting from September 2018. Their anthropometric characteristics are outlined in Table 1. Participants were recruited from the Belgian Defense Forces after being informed about the goal and the inclusion and the exclusion criteria by e-mail, advertising poster, or verbal announcement. All tests conformed to The Code of Ethics of the World Medical Association (Declaration of Helsinki). After expressing their interest and understanding by signing the written informed consent, they were invited for an intake and eligibility screening. The ethical committee of University Hospital Center Brugmann approved this study (Reference CE 2018/93).
The following exclusion criteria were applied: 1. previous pain or having undergone surgery in the upper extremity or spine within a year before the onset of this study [27]; 2. failing to pass the annual side bridge military physical fitness test; or 3. having less than 60
Procedure
The same physiotherapist (first author), familiarized with all the previously stated tests, conducted all the tests. To prevent order biasing the test sequence was randomized. After each test, a 5-min break was allowed [28]. Before testing, all subjects were given a detailed explanation of the testing procedures. The following baseline measures were taken into account: weight, height, (BMI), age, and physical activity level indices assessed by the Baecke questionnaire [29]. The standard warm-up before the first test consisted of ten times the PNF (Proprioceptive Neuromuscular Facilitation) flexion and extension D1 and D2 Pattern for each side with a light elastic band [30]. After a demonstration, the subject was positioned in the start position for each of the following tests. Verbal and tactile feedback were given during the tests to ensure proper execution.
Field tests
The Scapular Muscle Endurance test (SME) was originally developed from a strengthening exercise described by Sahrmann [31]. The test is meant to assess bilateral scapular stability and endurance of the scapulothoracic muscles [32]. For this test, the subject stood in front of a wall, with the shoulders and elbows in a 90/90
Scapular muscle endurance test.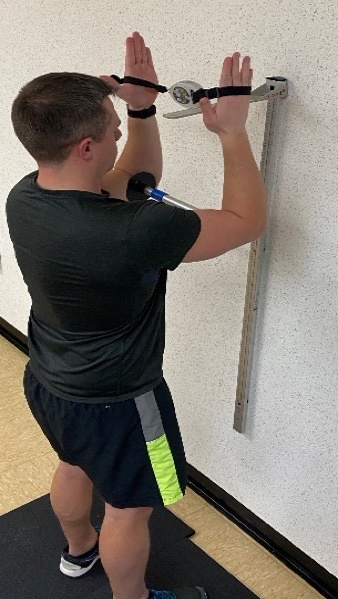
The Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) is a functional tool to measure the upper extremity stability and Power [34, 35, 36]. The CKCUEST was administered as followed: the subject took a push-up position for the start of the test with each hand on one piece of tape and keeping the body straight. Both pieces of tape were placed at 91.44 cm distance between the medial borders of the hands. Hands were placed at shoulder height and feet were positioned at shoulder width. The test was performed with shoes to prevent slipping (Fig. 2). The test consisted of moving one hand to touch the other hand while stabilizing the whole body and alternating sides. This sequence was repeated as quickly as possible for 15-s. Each start and stop were indicated by a beep of the timer (GYMBOSS, St. Clair, USA), the same as used for the SME, to standardize and a 45-s rest followed each trial. The first trial was sub-maximal for familiarization. The three following trials were taken into account and were videotaped with a smartphone to ensure the accuracy of test scores. Proper execution of the test included completion of the test with a straight body, arms perpendicular to the ground, keeping the feet in start position, without touching the floor with other body parts than hands and feet [16]. Each improperly executed trial was repeated after 45-s.
Closed kinetic chain upper extremity stability test.
The number of taps during the 15-s were recorded [35]. A tap counted when one hand touched the opposite hand. The mean value was calculated from the last three maximal trials and applied as the subject’s test score. Three types of scores were calculated: the raw score as the number of taps by the subject, the normalized score, the number of taps divided by the height, and a Power score by multiplying the average number of taps with 68% of the body weight in kilograms divided by 15 [37]. This last score represents the amount of work performed per time unit. The CKCUEST was found to be reliable in male college students (ICC 0.922) [35].
To have a more analytical or single-joint measure [38] of the shoulder’s, rotational strength a criterion standard isokinetic test is recommended [39]. We opted to test the participants in a supine position with the shoulder in 45
The isokinetic shoulder internal and external rotation test with the isokinetic dynamometer (CSMI, Humac/Norm 502140, Henley Healthcare, Sugarland, TX, USA).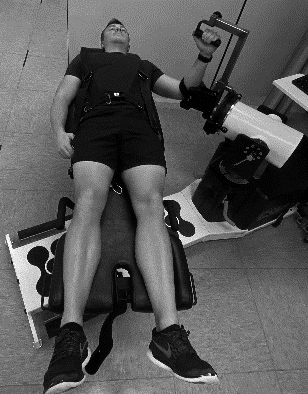
All further settings of the dynamometer were adapted individually to create the above-mentioned test position. Through standardization, first the non-dominant limb was tested and then the dominant, defined as the preferred limb. During all tests, participants were encouraged orally, but visual feedback from the computer screen was not permitted. Three familiarization series of 6 repetitions at 120
First, the subjects performed a maximal concentric-concentric IR-ER protocol at 120
Demographic characteristics of the subjects (
Following a 5-minute break, which allowed for a change of sides, the tests were repeated for the other limb using the same testing protocol as described above. The following outcomes were retained for further analysis: the bodyweight normalized peak moment (Nm/kgbw) and Power (Watt/kgbw) values for the IR, the ER, and the ER/IR ratio [12, 27].
All statistical tests were run on SPSS (IBM Corp, released 2019, IBM SPSS Statistics for Windows, Version 26.0, Armonk, NY). Outcome measures are displayed as mean
A descriptive analysis was performed on the anthropometric data and in those cases where the following parameters did not meet the assumption for normality: age, weight, BMI, preferred side, class, leisure-time index, and combined score, a Kruskal-Wallis ANOVA was performed. The demographic data were presented in frequencies.
For the reference data, possible side differences (within subject variable) between age groups (between-subject variable) were analyzed by a mixed-design ANOVA for all isokinetic test parameters. The following parameters did not meet the assumption for normality: the Non-Dominant (ND) PM/kg and the ND PM/kg ratio at 120
To examine the correlation between the three test data a Spearman Rank-Order Correlation Coefficient was calculated on each dependent variable because most of these were not normally distributed based on the Shapiro-Wilk tests. This was also done between some isokinetic IR and ER parameters in order to support our conclusions. The following categories for the Spearman rank-order correlation coefficient were used: negligible (
A priori power analysis for the post-hoc mixed design ANOVA by the G-Power program (G*Power Version 3.1.9.4, Dusseldorf, Germany) concluded the following there was 81% chance of correctly rejecting the null hypothesis of no significant effect of the interaction with 4 age groups for a total of 48 subjects with 12 subjects per group.
Results
The descriptive anthropometric data are displayed in Table 1. Only the mean BMI of the youngest age group was significantly lower than those in the oldest age group at post hoc testing. The age groups were comparable for all other anthropometric characteristics. The demographic characteristics are presented in Table 2 with their percentage of appearance in the sample (
Table 3 outlines the isokinetic reference values for the relative strength of the IR and ER measured at the 3 speeds. Table 4 displays similar results for the relative
Reference values of isokinetic peak moment for internal and external rotation of the shoulder in Mean
SD (95% Confidence interval) for the PM/kg (Nm/kg)
Reference values of isokinetic peak moment for internal and external rotation of the shoulder in Mean
Abbreviations: Diff, difference; D, dominant side; ND, non-dominant side; PM, Peak Moment;
Reference values of isokinetic angular speed for internal and external rotation of the shoulder in Mean
Abbreviations: Diff, difference; D, dominant side; ND, non-dominant side;
Reference values of the CKCUEST and the SME (min:sec) in Mean
Abbreviations: SME, Scapular Muscle Endurance test, CKCUEST, Closed Kinetic Chain Upper Extremity Stability Test;
Power values. The mixed-design ANOVA showed some significant side differences over the different age groups
Table 5 outlines the functional shoulder test reference values for the SME and the three CKCUEST scores. Post hoc analyses showed only for the raw CKCUEST scores a significantly higher score in the two youngest groups versus the oldest group (
The values of the correlation coefficient between the IR and ER power and the PM at 60
The primary goal of this study was to establish reference grouped age values for the CKCUEST, the SME, and the isokinetic shoulder strength and Power for the rotators in sports-active men and to examine the possible relationship between these tests. The main observations were: (1) when using these reference values age should be taken into account with the exception for the SME test; (2) the findings of these tests are not interchangeable.
Reference values for the field and isokinetic tests
In the current study, the CKCUEST findings were comparable to these of elite track and field athletes [43]. Although 90% of the present healthy cohort had a medical, administrative or logistic job, the CKCUEST is commonly used in patient and general populations [16, 17]. Comparing the youngest age group of the present study to another but smaller group of overhead active and sedentary males, the mean score of 27
Correlation coefficient (
) between the CKCUEST and criterion isokinetic test for the normalized strength and Power based on the Spearman rank-order correlation coefficient
Correlation coefficient (
Abbreviations: IR, Internal Rotators, ER, External Rotators, D, dominant side; ND, non-dominant side; PM, peak moment.
tient and general population (22; 22 taps) [17] also indicating that higher physical activity levels give higher raw CKCUEST scores. Moreover, the age effect apparent between the youngest age groups and the oldest within the present cohort is supported by another study among overhead athletes [25] indicating higher raw CKCUEST scores can be expected in younger cohorts.
Considering the SME test, we did not find an age effect on the test scores. Since this test is not frequently applied the only comparison could be made to two studies with smaller asymptomatic cohorts [28, 42]. The mean score of 153
Isokinetic strength and Power of IR and ER are mostly used in MSK screenings for the shoulder so several reference values do exist to compare with [44]. Unfortunately, for the supine lying protocol tested with the arm positioned at 45
One meaningful advantage of this method is its bilateral design and the detection of asymmetries. The only significant side asymmetry (12.4%) in favor of the ND side was detected for the IR Power at 240
The study [12], that inspired us using the specific supine protocol, tested a rather small sample (
We observed rather moderate to low Spearman correlation coefficients between IR and ER strength at 60
However these mixed correlations possibly reflect the difference in construct between both tests, which could be explained by the difference in muscle performance between the tests. During the CKCUEST, the muscles are providing isometric stabilization of the joint with glenohumeral movement while during isokinetic testing they are specifically executing a movement in the glenohumeral joint. Due to the lack of other studies examining the construct validity of the CKCUEST and the SME, the present finding provides a preliminary evidence that these three tests are not measuring the same construct in the present cohort. This supports the use of a combination of single-joint and multi-joint tests with upper limb evaluations [38].
Finally, in this study we have chosen the bodyweight normalized units for both strength and Power in view of their wide use. The addition of the latter parameter was motivated by the aspiration to derive additional information (beyond the PM). However, the very high correlations between these two outcome measures render Power a largely redundant parameter while leaving the PM (or PM/kg) as the quintessential isokinetic outcome parameter.
In terms of this study’s limitations, more participants could allow stronger comparisons between other studies and different populations (age groups, physical activity level subgroups and gender). In addition, previous studies already demonstrated significant age effects on the CKCUEST and hence future reference data studies should take this element into account, especially as in the present study we have under-represented the 50–55 age group (
Conclusion
Low to moderate Spearman correlation coefficients between the isokinetic and functional tests is an indication that including both tests in shoulder girdle screening could have an additional value.
In view of the analysis, we recommend that the PM is used as the representative parameter while using the range of the concentric ER/IR ratios: 58.9%–71.5%, as a general reference for similar cohorts when tested using the same protocol.
Author contributions
CONCEPTION: T. Van Haele, L. Moerman, N. Duvigneaud and D. Van Tiggelen.
PERFORMANCE OF WORK: T. Van Haele, L. Moerman, N. Duvigneaud and D. Van Tiggelen.
INTERPRETATION OR ANALYSIS OF DATA: T. Van Haele, L. Moerman, N. Duvigneaud and D. Van Tiggelen.
PREPARATION OF THE MANUSCRIPT: T. Van Haele, L. Moerman, N. Duvigneaud and D. Van Tiggelen.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: L. Moerman, N. Duvigneaud and D. Van Tiggelen.
SUPERVISION: L. Moerman, N. Duvigneaud and D. Van Tiggelen.
Ethical considerations
All tests conformed to The Code of Ethics of the World Medical Association (Declaration of Helsinki). The ethical committee of University Hospital Center Brugmann approved this study (Reference CE 2018/ 93). All participants signed a written informed consent, prior to participation.
Funding
There was no financial support that could have influenced this study.
Footnotes
Acknowledgments
A word of thanks is directed to the Director of the Military Hospital Queen Astrid for providing the infrastructure and for supporting this work. In addition, the authors want to thank all participants for their willingness to participate in this study.
Conflict of interest
The authors declare no conflict of interest.