
Abstract
BACKGROUND:
Rotator cuff weakness is considered an important risk factor for shoulder injuries in volleyball.
OBJECTIVE:
To evaluate association of shoulder preseason strength status with shoulder injury occurrence in subsequent season.
METHODS:
Volleyball players (
RESULTS:
During the season we have registered 14 (7.7%) shoulder injuries (10 in men). All injuries affected the dominant shoulder. There was significant preseason weakness of ER and lower ER/IR strength ratio in players with shoulder injury. Normal strength ratio ER/IR was a significant protective factor (Exp (B)
CONCLUSIONS:
The inclusion of systematic strengthening of the external rotators of the shoulder is necessary, especially for male volleyball players, as part of preventive measures for the prevention of shoulder injuries.
Introduction
Volleyball is one of the most interesting team sports that is played worldwide at all proficiency levels [1]. The basic characteristics of volleyball are different fast and explosive movements, ranging from rapid direction changes in the playing field to numerous vertical jumps and rapid overhead arm accelerations (swings) in the attack and/or the defense phase of the game. Although some matches can last up to 3 hours, volleyball is predominantly anaerobic sport [2], and in order to play at competitive level individuals must have certain physical characteristics in addition to the technical and tactical knowledge of volleyball. One of such characteristics is the strength of the muscle groups that are necessary for the execution of basic volleyball movements: vertical jump and overhead arm swings.
Overhead arm swing is the movement encountered in many sports (e.g. baseball, handball, water polo, tennis, badminton, javelin throw) and in volleyball it is necessary for spiking and serving. For completion of overhead arm swing all four joints of shoulder region (acromioclavicular, sternoclavicular, glenohumeral and scapulothoracic joint) are participating in a coordinated manner. However, the greatest stress is placed on the shoulder internal and external rotators (rotator cuff) that are responsible for the execution (concentrically) and the control (eccentrically) of the spike and studies have indicated that rotator cuff overloading may be a primary etiology of tendon pathology [3]. Therefore, it is not surprising that rotator cuff muscle weakness as diagnosed with isokinetic testing is an important modifiable factor associated with shoulder injuries in volleyball [4]. Additionally, concentric strength of the dominant shoulder (e.g. measured at 60
Epidemiological data shows that shoulder dysfunction is present in 8% to 20% of volleyball players and in almost 50% of the cases the nature of shoulder problems is such that it interferes with player’s sport performance [6], and these problems are responsible for the longest absence from the training and competition (6.2 weeks on average) [7]. More shoulder problems is reported by players at playing positions where spiking is more frequent and more intense (e.g. outside hitters, opposites, and middle blockers) [6], and this could be explained by differences in strength and strength ratios that were reported among different playing positions [8].
There were several cross sectional studies in which rotator cuff strength was compared between volleyball players with and without shoulder problems. Stickley [9] has reported that rotator cuff strength ratios were more related to shoulder injury prevalence than the absolute strength. Decreased dominant external rotation, higher deficit of dominant eccentric external rotation peak moments, and higher dominant rotator fatigability were correlated with previous shoulder pain/injury in a study which used mixed volleyball/handball population [10]. Finally, our research group has reported a findings from the largest volleyball cohort so far (99 men, 82 women) [11]. We found that male volleyball players with history of shoulder problems had a lower external-rotation/internal-rotation strength ratio of the dominant shoulder and that female volleyball players at a higher skill level were 2.5 times more likely to have abnormal strength ratios.
To our knowledge there is only one prospective cohort study so far that investigated the true relationship between rotator cuff strength and shoulder problems in the sample of 66 volleyball player (34 men) [12]. The eccentric maximal strength developed by the internal and external rotators was found to represent a protective factor in volleyball players (respective odds ratios
Methods
Participants
One hundred and eighty one (
Procedures
Each participant has completed an enrolment questionnaire about previous shoulder injuries, hand dominance, playing position, level of play, and hours of training. The D hand was defined as the hand used to serve or spike. Anthropometric measurements (body mass, body height, skinfolds) were performed using a stadiometer and scale (models 222 and 762, respectively; Seca Instruments Ltd, Hamburg, Germany) and Harpenden skinfold calipers (Holtain Ltd, Crosswell, Crymych, United Kingdom). From 7 skinfold measures, we calculated the body fat percentage using the Jacksons Pollock formula [13].
The same experienced examiner performed all the isokinetic testing procedures. Players from the same volleyball club were tested on the same day. A day prior to testing no practice was allowed. Each testing session started with a warm up consisting of 3 sets of 10 repetitions of shoulder internal and external rotation using elastic resistance band. All participants were given a detailed explanation about the testing procedure, which was also demonstrated on an independent subject not participating in the study prior to testing.
Testing was performed using Techno-Gym REV 9000 isokinetic dynamometer (TehcnoGym, SpA, Via G. Perticari 20, 47035 Gambet-Tola, Forli, Italy) in concentric-concentric mode at 60
Statistical analyses
All data were analyzed using the IBM SPSS Software for Windows (version 25, SPSS Inc., Chicago, Illinois, USA). Categorical variables are displayed as numbers and percentages, and continuous variables are presented as means and standard deviations. All numeric variables were firstly checked for normality of distribution with Shapiro-Wilk’s test.
Analyses were initially performed separately for sex. Preseason isokinetic findings of the D and ND shoulder were compared between injured and uninjured players using a one-way analysis of variance, while the differences between dominant and non-dominant shoulder were evaluated using paired
Results
Basic characteristics of the volleyball players that participated in the study are presented in Table 1.
Main characteristics of the volleyball players
Main characteristics of the volleyball players
During the one competitive season we have registered 14 shoulder injuries (10 in male and 4 in female volleyball players). All injuries affected the dominant shoulder. In male players there were 8 new injuries and 2 re-injuries, while in female players there were 2 new injuries and 2 re-injuries. Previous injury was significantly related with shoulder injury incidence only in females (
External-rotator and internal-rotator strength and strength ratios of the dominant (D) and nondominant (ND) shoulders (60
D – dominant shoulder; ND – non-dominant shoulder; a – significant difference between D and ND shoulder (please note that in subgroup of injured players this is comparison of healthy and injured shoulder); b – significant differences between injured and uninjured shoulder.
Multivariate logistic regression model for shoulder injury
Preseason isokinetic strength findings of the shoulder (Table 2) in male players with subsequent shoulder injury indicate significant preseason weakness of ER (0.45 vs. 0.54;
There was a significant association between a decrease in the ER/IR ratio and shoulder injuries in the male players (
In the logistic regression model (Table 3) we have used sex (men, women), previous injury (yes/no) and strength ratio ER/IR of the dominant shoulder (normal, abnormal) to predict injury occurrence. The model was statistically significant (
The receiver operating curve for classifying healthy players using the strength ratio between external and internal rotators of the dominant shoulder.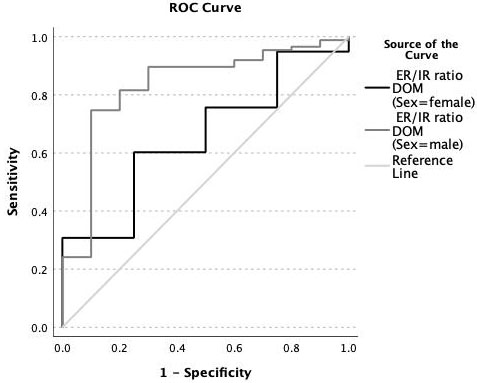
The main findings of our study have shown that dominant IR and ER muscles in uninjured male and female volleyball players, are significantly stronger compared to those of the non-dominant shoulder, resulting in symmetrical ER/IR strength ratio of both shoulders. However, in the injured male volleyball players significantly stronger IR of dominant shoulder, was not followed by concomitantly stronger ER, resulting in a significantly lower ER/IR ratio of the dominant shoulder during preseason testing. Additionally, the logistic regression model indicates that the normal strength ratio represents an important protective factor for shoulder injuries in volleyball when controlled for sex and previous shoulder injury. When preseason results were compared between injured and uninjured players, it was shown that injured players had significantly weaker external rotators (
Compared to the only prospective study about rotator cuff strength and shoulder injury so far [12] which concluded that the eccentric maximal strength developed by the IR and ER groups was found to represent a protective factor in the volleyball players (respective odds ratios
Despite the noticeable differences between men and women, we have not been able to show that the occurrence of shoulder joint injuries varies between the sexes, although the absolute number of injured male volleyball players was 2.5 times higher than that of female volleyball players. This is in agreement with previous findings that excluded sex as an independent risk factor for shoulder injuries in volleyball [6].
The difference in strength and strength ratios findings between the sexes could otherwise be explained by (a) the number of hand swings during a single point (in women the point lasts longer, and there is usually more ball exchange between the sides, which also means the need for more swings in women compared to men) [17]; (b) there could be differences in the amount and specificity of strength training between the sexes (Table 1; 413 vs 311 h of training per year in men vs women, respectively), and (c) there could be sex-related differences in the biomechanical execution of the spike. For example, during maximum shoulder external rotation, potential energy is also stored in trunk rotation [6] and female volleyball players could be weaker in this segment and therefore rely more on the shoulder girdle than on the torso rotators in the desire for the best possible quality of offensive spikes.
This last hypothesis could be partly supported by the fact that the values of the ER/IR ratio actually differed between the sexes. In uninjured volleyball players these values were between 0.60 and 0.65, and in uninjured female players between 0.70 and 0.78. This was also shown by the Forthomme et al. [12] where ER/IR strength ratio for men and women was 0.68 and 0.80, respectively. Even studies on adolescent volleyball players [18] have shown that strength ratio is higher in girls then in boys. Compared with values from previous research, the classical references [19, 20] appear to be sufficient for a protective effect in men, while somewhat more recent guidelines [15], appear to be more suitable for women. The higher strength ratio in females actually supports our hypothesis that women could be relying more on shoulder girdle for spiking than on the trunk rotation.
Conclusion
Based on our findings, we conclude that the inclusion of systematic strengthening of the external rotators of the shoulder is necessary, especially for male volleyball players, as part of measures for the prevention of shoulder injuries. While strong internal rotators are necessary for optimal performance, strong external rotators are obviously necessary for optimal health of the shoulder in volleyball. Strength and conditioning coaches should therefore pay more attention to match strong internal rotators with strong external rotators.
Author contributions
CONCEPTION: VH, ED, TS
PERFORMANCE OF WORK: PP, AH
INTERPRETATION OR ANALYSIS OF DATA: VH, TS
PREPARATION OF THE MANUSCRIPT: VH
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: VH, ED, PP, AH, TS
SUPERVISION: ED
Ethical considerations
National Medical Ethics Committee (no. 63/07/12) has approved the study on July 31
Funding
The study was supported by Slovenian Research Agency, grant number P5-0147.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
All authors declare no conflict of interest. Given his role as an Editorial Board Member, Vedran Hadžić had no involvement nor access to information regarding the peer review of this article.