
Abstract
BACKGROUND:
Blood flow restriction (BFR) resistance training (RT) has garnered recent interest, but female-specific data remains scarce.
OBJECTIVE:
The purpose was to examine the effects of 2-wks of low-load concentric, isokinetic, reciprocal forearm flexion and extension training, with and without BFR on perceptual responses, performance fatigability, and muscular strength.
METHODS:
Twenty women were assigned to a BFRT or a non-BFRT group. Each group trained at 30% of concentric peak moment. Each session consisted of 75 concentric, isokinetic, reciprocal forearm flexion extension muscle actions. RPEs were recorded following each set. Pretest and posttest maximal voluntary isometric contraction (MVIC) force was measured, and percent decline was defined as performance fatigability.
RESULTS:
The RPE values (
CONCLUSIONS:
2-wks of low-load concentric, reciprocal forearm flexion and extension training resulted in similar training-induced changes in perceptual responses, performance fatigability, and muscular strength between BFRT and non-BFRT. These findings may reduce concerns of increased perceptual responses following BFRRT compared to non-BFRRT.
Introduction
It is well known that there is historical and current sex bias in biomedical research, which results in significantly lower reporting of data related to women [1]. Recent studies [2, 3, 4, 5] investigating the effects of blood flow restriction resistance training (BFRRT) and BFR aerobic training on perceptual as well as behavioral responses, however, have utilized primarily male samples. Thus, additional research in women is needed to understand the efficacy of low-load (
Previous investigations [15, 16, 17, 18, 19] have examined ratings of perceived exertion (RPE) following BFRRT. For example, Loenneke et al. [17] examined 15 men who on average reported significantly higher RPE values following 2 sets of low-load (30% 1RM) bilateral leg extensions to failure with BFR than without occlusion (6 vs. 5 RPE units, respectively, on the Borg CR-10 Scale). Mattocks et al. [16] recently examined 40 participants across 8 weeks of progressive BFRRT and non-BFRRT and reported that there was a significantly greater reduction in RPE for the BFR group compared to the non-BFR group. Due to the study design (i.e. increasing the number of sets across training sessions), however, the authors [16] only analyzed the RPE value from the first set of each session, which was presented as a limitation. Thus, how RPE changes across set for occlusion and non-occlusion conditions in women remains unknown. Hollander et al. [20], however, have examined RPE on a repetition-by-repetition basis to estimate a metabolic break point (RPE
Human performance and the ability to continue exercise are limited by the perception of fatigue and the overall exercise-induced decrease in force or power of a muscle, termed performance fatigability [22]. Performance fatigability has recently been reviewed in the context of its manifestation and its relevancy pertaining to sex-related differences [22]. It has been suggested that inducing performance fatigability through performing repetitions to failure was necessary to elicit maximum increases muscular strength [23, 24], but this notion remains debatable. In theory, the ability to attenuate performance fatigability would promote the maintenance of force throughout a work bout and training session, which would likely lead to greater improvement in strength via increased exercise volume over time [25]. In conjunction with this concept, Hureau et al. [26] have hypothesized that exercise training may “raise” an individual’s tolerance to sensations associated with the cessation of exercise, which would result in greater magnitude of performance fatigability. Currently, however, little is known regarding the relationship between BFRRT and performance fatigability as well as how this relationship contributes to muscular adaptations in women. For men, however, Evans et al. [27] reported that 4-wks of plantar flexion (3
Short-term low-load BFRRT has been used to investigate changes in muscular strength [6, 32]. For example, Abe et al. [32] demonstrated that 2 weeks of BFRRT at 20% 1RM resulted in a 16.8% increase for barbell squat strength. Abe et al. [32], however, used a variable cuff pressure across training sessions, so it remains unknown if short-term BFRRT with a constant cuff pressure elicits similar increases in muscular strength as well as if there are concurrent changes in perceptual and performance fatigability responses in women. Therefore, the purpose of the present study was to examine the effects of 2 weeks of low-load concentric, isokinetic, reciprocal forearm flexion and extension training, with and without BFR, on perceptual responses, performance fatigability, and muscular strength in women. Based on previous studies [7, 16, 18, 29], it was hypothesized that: 1) BFRRT would result in greater acute and chronic RPE values than non-BFRRT; 2) Performance fatigability would increase as a result of both BFRRT and non-BFRRT; and 3) BFRRT and non-BFRRT would elicit similar increases in forearm flexion and extension strength.
Methods
Participants
Twenty recreationally active women [33] with no known cardiovascular, metabolic, or muscular diseases volunteered to participate in this investigation. The subjects were a part of a large multi-dependent variable study, but there is no overlap between the current study and previously published data [34]. Furthermore, in the present study, the women were randomly assigned to either the BFRRT group (
Timeline of investigation. Note: Changes in maximum strength reflect the mean increases from pretraining MVICs 1 to pretraining MVICs 2. Changes in performance fatigability reflect the mean differences between the percent decline from pretraining MVIC 1 to post-training MVICs 1 and the percent decline from pretraining MVICs 2 to post-training MVICs 2.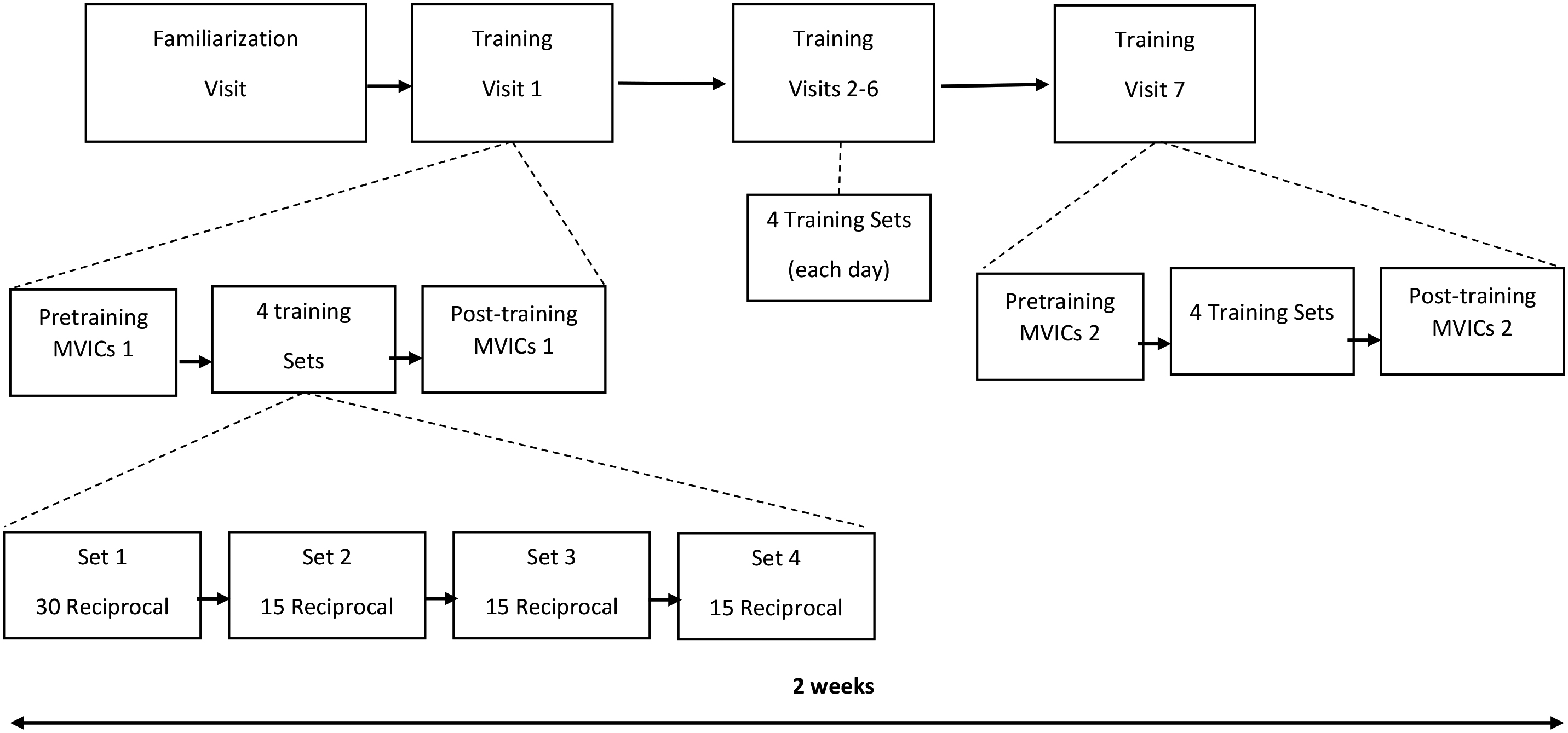
This was a randomized, repeated-measures, between-group, parallel design investigation (Fig. 1). Women were separated into two different groups: a BFRRT and a non-BFRRT group. The BFRRT group wore a cuff on their upper arm at a pressure of 40% of the lowest pressure necessary to completely occlude the arterial inward flow, which completely occluded venous return from the training limb. Each group completed the same training 2-wk program, which consisted of reciprocal concentric forearm flexion-extensions at a load of 30% maximum for each respective muscle action (i.e. 30% flexion maximum and 30% extension maximum). During each day of training, the participants completed 4 sets (1
Familiarization visit
During the familiarization visit, the subjects’ height (Cardinal Detecto 439 Mechanical Beam, Webb City, MO USA) and body mass (Cardinal Detecto 439 Mechanical Beam, Webb City, MO USA) were recorded. The subjects were oriented to their seated position on the isokinetic dynamometer based on manufacturers recommendations (Biodex System 3; Biodex Medical Systems, Inc. Shirley, NY, USA). Once positioned on the dynamometer, the subjects performed isometric and concentric, isokinetic, forearm flexion and extension muscle actions at submaximal and maximal intensities. The training arm of each participant was randomized so that there were an equal number of participants training their dominant and non-dominant arm (Dominant arm was defined as the arm used to throw a ball). The subjects were oriented to the training procedures by performing reciprocal concentric-only isokinetic forearm flexion and extension muscle actions at 30% of their forearm flexion concentric peak moment and forearm extension concentric peak moment. During all visits, the subjects were able to visually track moment production on a digital monitor. All concentric, isokinetic muscle actions were performed at 120
Training visits
Each training session consisted of 75 concentric, isokinetic, reciprocal forearm flexion-extension muscle actions performed over four sets (1
Blood flow restriction
During all training session sets (i.e. 1
Ratings of perceived exertion
Following each training set, the subjects were asked to provide an RPE value that corresponded to the OMNI-RES [36, 37]. Thus, the subjects provided a total of 4 RPE values per training visit. Prior to the first training visit, the subjects were familiarized and permitted to ask questions regarding the OMNI-RES. Also, prior to the first set of each training visit, the subjects were reminded to be attentive to sensations such as strain, intensity, discomfort, and fatigue felt during the set when providing a post-set RPE value [21].
Statistical analyses
Independent
A. Individual subject (unique symbols) and mean (collapsed across Muscle Action and Group) (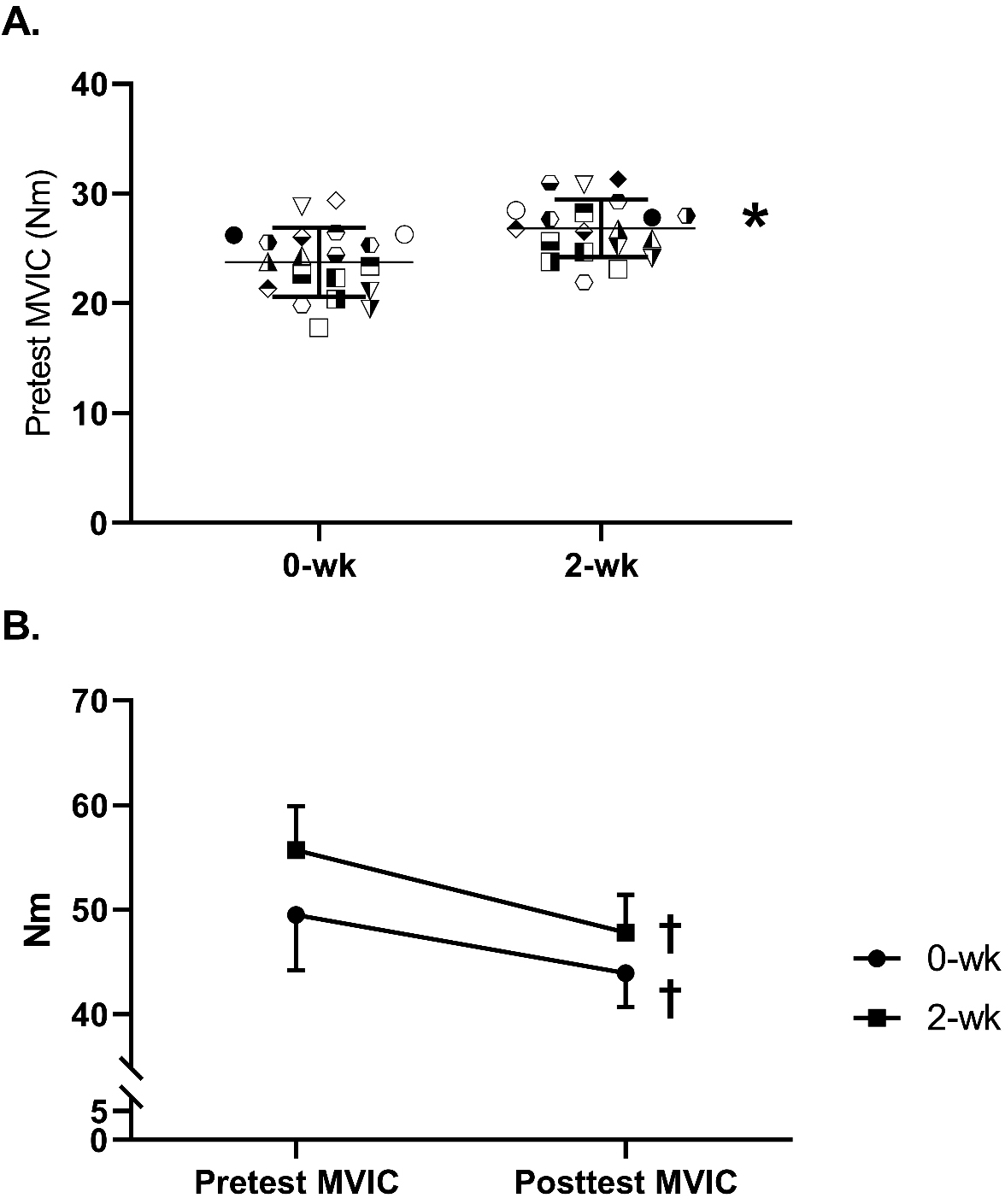
The pairwise comparisons (collapsed across Group) of the RPE values reported following each set resulting from the seven (i.e. one for each Training Visit) follow-up 1-way repeated measures ANOVAs
Daily training loads, performance fatigability, and strength
For daily concentric, isokinetic forearm flexion training loads, there was no significant (
Ratings of perceived exertion
There was no significant (
Discussion
The purpose of the present study was to examine the effects of low-load concentric, isokinetic, reciprocal forearm flexion and extension training, with and without BFR on perceptual responses, performance fatigability, and muscular strength. The primary findings of this study were that following short-term training: 1) There were no differences in the RPE values between the BFRRT and non-BFRRT groups; 2) performance fatigability increased in response to training, but there was no difference between groups or muscle actions; and 3) the BFRRT and non-BFRRT groups exhibited similar increases in forearm flexion and extension MVIC strength.
The current results indicated that there were no differences between the BFRRT and non-BFRRT groups for the perceptual responses across the short-term training. These findings are not consistent with a recent study [16] which examined multiple sets of dynamic constant external resistance (DCER) forearm flexion and leg extension muscle actions under four different conditions which included a training intensity of 15% 1RM with no BFR, 15% 1RM plus 40% of arterial occlusion, 15% 1RM plus 80% of arterial occlusion, or 70% 1RM with no BFR across 16 training sessions. Unlike the present study, the findings of this study indicated that low-load BFRRT reduced the perception of exertion to a greater extent than training without BFR. Several methodological differences, such as the use of a different tool for assessing the RPE, could account for the observed discrepancies. However, another study [17] reported that when unilateral leg extensions were performed at 15% 1RM to volitional failure, there were no differences in RPE values following one set with (40% or 80% of arterial occlusion) or without BFR. Thus, the current findings are in general agreement with those reported in [18] by demonstrating that there were no differences in the perceptual responses between BFRRT and non-BFRRT following short-term training of concentric, isokinetic, reciprocal forearm flexion and extension training.
In the current study, RPE increased across most of the sets during each training visit (Table 1). For all training visits, the mean RPE values after set 4 were significantly greater than those of set 1 and 2. These findings suggested that both training groups (BFRRT and non-BFRRT) experienced similar increases in sensations such as strain, intensity, discomfort, and fatigue by the end of set 4 [21]. It has been demonstrated that RPE values are influenced by metabolic stress via group III/IV muscle afferents [38]. This increase in metabolic stress has been proposed as potential mechanism for eliciting favorable muscle adaptations following BFR training [7, 13]. The current results, however, did not demonstrate any differences in RPE values, MVIC increases, or changes in performance fatigability between the BFRRT and non-BFRRT groups, which may have been indicative of similar degrees of metabolic stress between the two groups [38]. Pinto et al. [15] demonstrated that 3 sets of 10 repetitions of DCER in bilateral leg extension mode resulted in a significantly greater blood lactate (i.e. metabolic stress) response at an intensity of 65% 1RM with no BFR compared to 20% 1RM plus BFR. In addition, it has recently been suggested [39] that the BFR cuff pressure should be set above 40% of arterial occlusion to induce metabolic stress as indirectly indicated by increases in deoxyhemoglobin via near-infrared spectroscopy. Thus, perhaps the intensity (30% 1RM) and cuff pressure (40% of arterial occlusion) used in the current study for the concentric, isokinetic, reciprocal forearm flexion and extension training were not sufficient to elicit a difference in metabolic stress between the BFRRT and non-BFRRT group, which was reflected by the similar self-reported perceived exertion values.
The current investigation found that after completing 7 of the training prescriptions (i.e. 75 repetitions) of the low-load BFRRT or non-BFRRT there was an increase (collapsed across Group and Muscle Action) in performance fatigability (Fig. 2B). Previously, Mayhew et al. [29] reported that a 12-wk linear periodization non-BFRRT program resulted in a 35.5% increase in performance fatigability. The authors [29] attributed this effect to an interaction of training-induced neural, muscular, and metabolic adaptations. Given the short duration of the current study, however, it was hypothesized that neural factors (i.e. voluntary activation) specific to the mode (BFRRT and non-BFRRT) or muscle action (flexion and extension) primarily contributed to the increase in performance fatigability [40, 41]. Of note, this is the first investigation to examine performance fatigability following BFRRT in women. Previous studies [12, 35, 42], however, have reported a greater magnitude of performance fatigability following a single bout of BFRRT than non-BFR conditions. For example, Husmann et al. [12] examined performance fatigability following multiple sets (1
The results of the current study indicated that there was no difference between the BFRRT and non-BFRRT groups for increases in maximal strength (MVIC). Following the 2-wks of BFRRT or non-BFRRT (6 training visits), there was a 13.1% increase (collapsed across Muscle Action and Group) in MVIC strength (Fig. 2A). Following 6–8 weeks of RT, it has been reported that there was no difference in the increase of strength [8, 45] between low-load unilateral leg extension with and without BFR. Fahs et al. [45] reported that following 6-wks of low-load (30% 1RM) unilateral DCER leg extension training, BFRRT and non-BFRRT conditions elicited an equal increase (
The current study was unable to determine if the strength gains were a result of hypertrophy or neural adaptations. This should be considered a limitation. Additionally, we did not record the work expanded in each individual repetition during training and hence it is unclear if the peak moment or work performed contributed more to RPE.
Conclusions
In summary, 2-wks of low-load concentric, reciprocal forearm flexion and extension training resulted in similar training-induced changes in perceptual responses, performance fatigability, and muscular strength between BFRRT and non-BFRRT. Future studies are needed to determine the work-RPE relationship as well as the underlying mechanisms related to strength adaptations following short-term training BFRRT training in women. However, the current findings may be used to reduce concerns of increased perceptual responses following BFRRT compared to non-BFRRT.
Author contributions
CONCEPTION: Joshua L. Keller, Ethan C. Hill, and Terry J. Housh.
PERFORMANCE OF WORK: Joshua L. Keller and Ethan C. Hill.
INTERPRETATION OR ANALYSIS OF DATA: Joshua L. Keller, Ethan C. Hill, Terry J. Housh, Cory M. Smith, John Paul V. Anders, Richard J. Schmidt, and Glen O. Johnson.
PREPARATION OF THE MANUSCRIPT: Joshua L. Keller, Ethan C. Hill, Terry J. Housh, Cory M. Smith, John Paul V. Anders, Richard J. Schmidt, and Glen O. Johnson.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Joshua L. Keller and Ethan C. Hill.
SUPERVISION: Terry J. Housh, Richard J. Schmidt, and Glen O. Johnson.
Ethical considerations
All procedures were conducted in accordance with the Declaration of Helsinki. The study was approved by Institutional Review Board (ID#: 20180918559EP). All subjects signed a written informed consent prior to testing.
Funding
Nebraska NASA Space Grant.
Footnotes
Acknowledgments
We would like to thank all the participants for their time and for volunteering to comply with the protocol of the study as well as the Nebraska NASA Space Grant for funding this study.
Conflict of interest
The authors have no conflict of interest and the results of the present study do not constitute endorsement of the product by the authors.