
Abstract
BACKGROUND:
Although the medial and lateral hamstrings are clearly distinct anatomically and have different functions in the transverse plane, they are often considered as one muscle during rehabilitation.
OBJECTIVE:
The purpose of the study was to compare the electromyographic (EMG) activity between the prone position and the supine position during maximal isometric contraction and to additionally confirm the effect of submaximal isometric contractions on EMG activity of medial and lateral hamstrings, and force.
METHODS:
In the prone position, EMG activities of the long head of biceps femoris (BFLH) and semitendinosus (ST) were measured during the maximal isometric contraction. In the supine position, hip extension force with EMG activity were measured during the maximal and the submaximal isometric contractions.
RESULTS:
EMG activity in the prone position was significantly decreased in the supine position. In the supine position, there was a significant difference between the BFLH and ST during the maximal isometric contraction, but not during the submaximal isometric contractions.
CONCLUSIONS:
The dependence on the hamstrings could be relatively lower during hip extensions. When the medial and lateral hamstrings are considered separately, the lateral hamstrings may show a more active response, with increased muscle length, in clinical practice.
Introduction
Stretching is a widely practiced technique to prevent exercise-induced strain injury in the muscles of the lower extremity, especially the hamstring muscles. Stretching not only can increase flexibility and muscle performance but can also reduce the risk of injury [1, 2, 3, 4]. Currently, among the many stretching techniques, proprioceptive neuromuscular facilitation (PNF) stretching requiring an isometric contraction is the most widely used along with static stretching in both research and practice [5, 6, 7]. However, the tension force caused by the stretching is not transferred to the only targeted soft tissues. Force is sometimes transferred to unwanted tissues that are already highly mobile, which induces joint instability. Moreover, even if the force is accurately transferred to the targeted muscle, it may not produce the expected effect [8, 9]. In particular, two-joint muscles such as the hamstrings are multifunctional and require a clear understanding of the mechanism that produces and transfers force to them and to each individual joint involved.
The hamstrings consist of 4 muscles: long head of biceps femoris (BFLH), short head of biceps femoris (BFSH), semitendinosus (ST), and semimembranosus (SM). Except for the BFSH, which crosses only the knee joint, the hamstrings originate from the ischial tuberosity and are inserted on both sides of the tibia and fibula. Based on the location of insertion, hamstrings are divided into the medial hamstrings (MH) and lateral hamstrings (LH). Owing to their anatomical location, hamstring muscles are mainly involved in flexion and extension of the knee and hip joints and additionally have a tibial rotation function [10]. Despite the different anatomical characteristics, muscle fiber orientations, and physiological characteristics, the treatment strategy in clinical practice often tends to be established with the hamstrings considered as a single muscle. The same method is used in the quantitative and qualitative evaluation of the hamstrings even under different conditions. The roles of hamstrings acting as knee flexors and/or hip extensors and the differences between MH and LH, must be considered.
Consort flow diagram.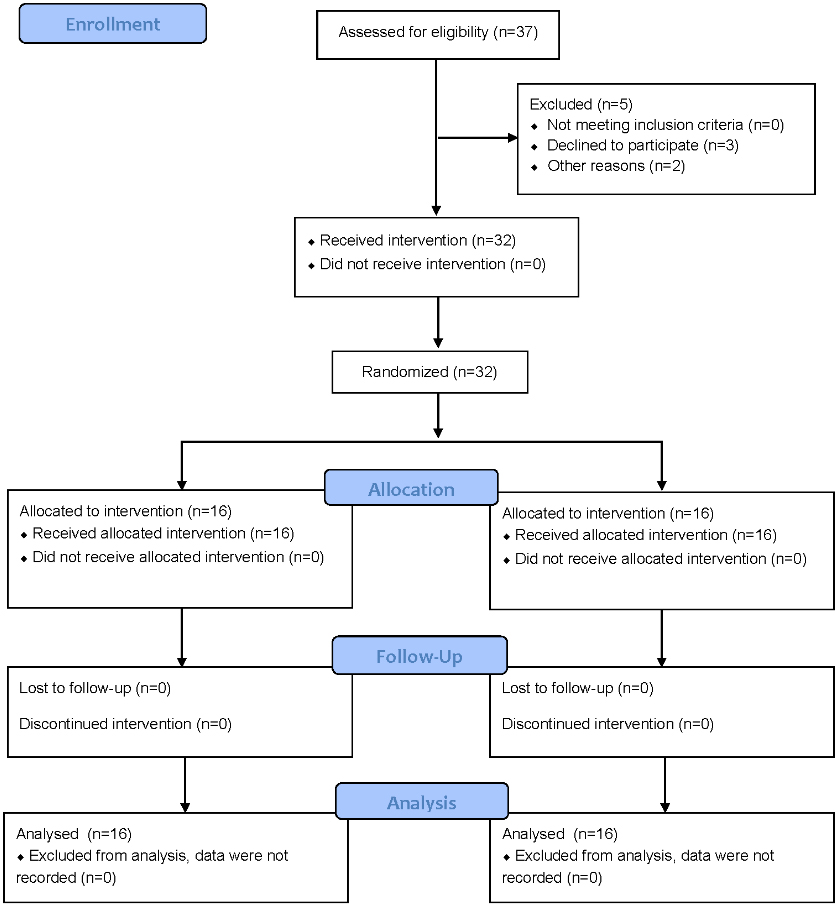
In clinical practice, manual muscle testing (MMT) for the hamstrings is generally conducted in the prone position with knee flexion [11, 12]. As trunk and pelvic movements are limited, the hamstrings act as knee flexors in the prone position. Meanwhile, stretching to increase hamstring flexibility is mostly performed in the supine position with the straight leg raise (SLR) [5]. Because the knee joint reaches full extension and is locked, the hamstrings function as hip extensors in the supine position. Although some studies have considered movements in the hip and knee joints together, hip joint movements were mostly performed in the seating or prone position, which is different from the method used in real clinical settings [13, 14]. Furthermore, although the electromyography (EMG) activity of the hamstrings during high-intensity contractions is different from that during moderate- to low-intensity contractions, most studies have conducted tests during maximal voluntary contraction (MVC). Past studies have indicated that, in the quadriceps muscle, activation patterns of the vastus medialis and vastus lateralis were influenced by the contraction intensity [15].
The present study aimed therefore (i) to compare the EMG activity between the prone position (used in MMT), in which the hamstrings act as knee flexors, and the supine position (used in stretching), in which the hamstrings act as hip extensors, and (ii) to additionally confirm the effect of submaximal isometric contractions on EMG activity of MH and LH.
Subjects
A total of 37 individuals volunteered for the experiment. Those with a neurological problem affecting the lower extremity or pain in the hip and knee joints were excluded. Five individuals were excluded from the final participants; two participants were excluded due to knee joint pain and three participants declined to participate the study before starting and study-related activities. A total of 32 participants (18 men and 14 women, age 21.50
Instrumentation
The Delsys-Trigno Wireless EMG system (Delsys Inc., Boston, MA, USA) was used for EMG measurements. In the present study, the sampling rate was set at 2,000 Hz, the band pass filter was set at 20–450 Hz, and a 60-Hz notch filter was used to remove any noise from electrical signals. EMG data were collected using Delsys EMGWorks Acquisition (Delsys Inc.) and analyzed using Delsys EMGWorks Analysis 4.3.1.0. The measured EMG signals were processed using the root mean square method. Each task was performed a total of 3 trials for 5 seconds each, with the middle 3 seconds used to calculate the mean values. The skin was shaved before the experiment. EMG electrodes were placed at 50% on the line between the lateral epicondyle of the femur and the ischial tuberosity for biceps femoris and between the medial epicondyle of the femur and the ischial tuberosity for semitendinosus (Fig. 2a). Placements of EMG electrodes were in accordance with the “Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles” recommendations [16].
Placement of the surface electromyography electrodes (a) and the measurements in the prone position (b) and supine position (c).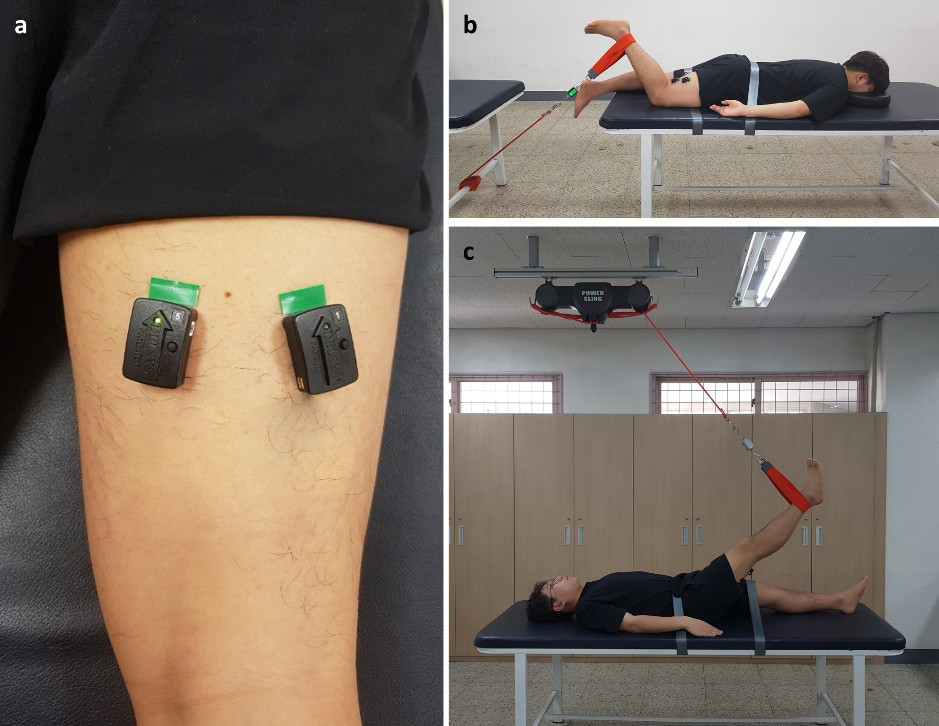
To measure muscle force during maximal voluntary isomeric contraction (MVIC) in EMG, the present study used the tension gauge (Re-live Inc., Jeonju, Korea) connected to the sling. The measured values were saved every 0.25 second, and the middle 3 seconds in the measured 5 seconds were used to calculate the mean values.
A universal goniometer was used for hip and knee joint angle measurements in the prone and supine positions.
Before starting the main experiment, each participant walked on the treadmill for five-minutes as a warm-up. After taking a break, participants lied on the treatment table in the prone position. The strap was used to firmly secure the non-dominant leg and pelvis in order to prevent unnecessary movements during the measurement. Only the dominant leg was used for measurement. During MVIC in the MMT position (knee joint at 60
Statistical analysis
Normality of the data was assessed by Shapiro-Wilk test. The independent t-test was used to compare EMG activity between the BFLH and ST and between group A and group B. The paired t-test was used to compare EMG activity in the same muscle between different intensities. A p-value of 0.05 was used to indicate statistical significance, and SPSS version 25.0 (Statistical Package for the Social Sciences, Chicago, IL, USA) was used for all calculations.
Results
There was no statistical difference in physical characteristics (age, height, and weight) between the 2 participant groups (Table 1).
Characteristics of participants
Characteristics of participants
Data are expressed as mean
Changing from the prone to the supine position resulted in a large decline in EMG activity (Table 2). The % MMT of BFLH sharply declined to 46.73% in group A and 40.07% in group B, with no significant difference between the groups (
Percent MMT (%) in the supine position as compared with the prone position
Percent MMT (%) in the supine position as compared with the prone position
Data are expressed as mean
The EMG activity in the MH and LH at the same contraction overall showed no large difference. At P100, however, the EMG activity of the BFLH was 43.40
EMG activity changes depending on stretching intensity
In the supine position, the hip extension force was 92.92
Percent Max (%) of submaximal isometric contractions as compared with maximal isometric contractions in the supine position
Percent Max (%) of submaximal isometric contractions as compared with maximal isometric contractions in the supine position
Data are expressed as mean
Changes in functional involvement required for the hamstrings to act as hip extensors or a knee flexor
Changing the position from prone to supine resulted in a decrease in % MMT: 40.07–46.73% in the BFLH and 28.17–33.15% in the ST. A reduction of EMG activity can occur because of a decline in muscle force output or motor unit recruitment. Muscle length is highly likely to have influenced the muscle force, as it largely affects the individual sarcomere length during joint movements [19, 20, 21]. When the position was changed from prone to supine, the knee joint was changed from 60
In some studies, however, the muscle length did not significantly influence EMG activity or its effect was not large; thus, muscle length alone likely cannot sufficiently explain a 60–70% decline in EMG activity [23, 24]. The understanding that multi-joint muscles have complex multiple functions is required. Bi-articular hamstrings can assign different roles to each joint, unlike single-joint muscles, and the magnitude of involvement required from each joint may vary. In this study, the axis of rotation was changed from the knee joint to the hip joint as the position was changed from prone to supine, and the functional role of the hamstrings changed from knee flexor to hip extensor. Considering the anatomical locations of the hamstring muscles and their connection to surrounding muscles, it is difficult to conclude that the hamstrings have the same level of dependence on both joints. In other words, the magnitude of involvement required for each joint can be different. In hip extension, the gluteus maximus and the extensor head of the adductor magnus are also involved as primary hip extensors along with the hamstrings [25]. In particular, the gluteus maximus has a high magnitude of involvement [26, 27, 28]. The fact that other hip extensors have a high magnitude of involvement in hip extension movements means that the dependence for the hamstrings could be relatively lower in hip extension. The relatively high EMG activity in the prone position might indicate that the preferred role of the hamstrings is as knee flexors rather than as hip extensors. Worrell et al. (2001) measured the EMG activity changes in the hamstrings when the hip and knee joints were at 0
EMG activity differences in the medial and lateral hamstrings under the same condition (contraction intensity)
The hamstrings are divided into the MH and LH depending on the anatomical location and are also involved in tibial rotation [10]. Although there have been some studies on the differences in MH and LH EMG activity during maximal isometric contraction, studies investigating muscles during submaximal isometric contractions have been limited. In a previous study, the activation patterns of the medial and lateral components of the quadriceps femoris were influenced by the contraction intensity [15]. The experimental results in the present study showed that the % MMT of the BFLH, which belongs to the LH, was significantly higher than that of the ST, which belongs to the MH, at P100 performed in the supine position. According to Ericson (1988), in ergometer cycling, which requires movements in the hip and knee joints, it was observed that the MH played a major role in knee flexion, whereas the LH played a key role in hip extension, supporting the results of the present study [29]. Another reason would be that the LH had some advantage over the MH in muscle length, which was extended when the LH produced force. The ST and SM maintain or increase EMG activity along with increasing knee flexion angles; however, the BFLH tends to show decreased EMG activity [30, 31]. If a major variable is the muscle length under the same conditions, the MH may be more useful than the LH in producing force in a shorter muscle length.
As compared with EMG activity measured during maximal isometric contractions in the supine position (P100), the EMG activity percentage of the MH and LH during submaximal isometric contractions showed that the ST had a slightly higher percentage at both P60 and P20. However, it was not because the EMG activity of the ST (numerator) was higher but was because P100 (denominator) was relatively lower, which meant that the dependence on ST was relatively lower than that of BHSH while the hamstrings act as hip extensors.
Effect of different stretching intensities on EMG activity in the given muscle length
Table 3 shows the EMG changes in accordance with different stretching intensities (performed only in the supine position, not in the prone position). As the position was not changed, they were all measured in the given muscle length. Because other variables, including the moment arm as well as the muscle length, were the same, the changes in EMG activity were resulted from the different muscle contraction intensities. In most previous studies, the submaximal intensity experiment was conducted in the knee joints. In a study that used the isokinetic dynamometer to measure MVC, followed by 50% of MVC and 25% of MVC at submaximal intensities, a similar decrease in both the MH and LH was observed [30]. Another study, which used cuff weight loads up to 1–7% of the body weight in the knee joint and applied different resistance levels, found that as external resistance increased, the EMG activity in the LH increased whereas that in the MH decreased ) [32]. As mentioned earlier, however, the hamstrings act as hip extensors in addition to acting as knee flexors. It is necessary to investigate the EMG changes at different intensities when the hamstrings function as hip extensors. According to the present results, both muscles showed a significant decline in EMG activity at submaximal intensities against the maximal intensity. Specifically, at P60, which required 60% of the maximal force, the MH and LH showed a % Max of 58.09–61.84%, which indicated a percentage decline in EMG activity that is very similar to the decline in force. However, at P20, which required 20% of the maximal force, both the MH and LH showed 36–46% activity on EMG, which indicated a smaller decrease than expected. The above indicates that the hamstrings have a characteristically high magnitude of involvement at low-intensity. The tension gauge measured not only the extension force produced from the hamstrings but also the force of other hip extensors combined. The consistently high EMG activity at low-intensity suggests that the involvement of other hip extensors was relatively lower. As the hamstrings are generally known to be important in high-intensity exercise, it is easy to presume that they have the characteristics of fast muscle fibers. According to the study of fiber type proportion, however, type I fibers accounted for 66.9% of the BFLH, which showed a very high proportion of slow muscle fibers [33]. The classification based on myosin heavy chain composition also indicated that IIX accounted for 17.4%, which showed a very low proportion of fast muscle fibers [34]. The high proportion of slow muscle fibers and the low proportion of fast muscle fibers demonstrate that the hamstrings are largely involved in movements that require repeated low-intensity contractions.
This study is limited in that no gravitational correction was applied. However, this might not be significant because all the procedures were performed under the same conditions. In each subject, EMG measurement was performed during maximal and submaximal isometric contraction at the same hip flexion angle. Thus, even if gravity affected the measurement, its effect was equally applied.
Conclusion
If general training is required for the overall muscles of the lower extremity, it is recommended to cause movements in the hip and knee joints together. However, if selective training is required for the hamstrings in the supine position, a low-intensity training program may be recommended to minimize the involvement of other hip extensors. When the MH and LH are considered separately, the LH may show a more active response, with increased muscle length, whereas the MH can show such response in a shorter muscle length.
Author contributions
CONCEPTION: Wootaek Lim.
PERFORMANCE OF WORK: Dasom Oh.
INTERPRETATION OR ANALYSIS OF DATA: Dasom Oh and Wootaek Lim.
PREPARATION OF THE MANUSCRIPT: Dasom Oh.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Wootaek Lim.
SUPERVISION: Wootaek Lim.
Ethical considerations
The present study was conducted after obtaining approval from the Institutional Review Board of Woosong University (Approval number: 1041549-180419-SB-59, Date: April 19, 2018). The participants were fully informed about the experiment and provided informed consent for their participation.
Funding
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2017R1C1B5076885); and the Woosong University 2019 Academic Research Funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors report no conflict of interest.