
Abstract
BACKGROUND:
The cardiovascular response to resistance training is influenced by different variables such as intensity and volume.
OBJECTIVE:
To compare the effects of resistance training sessions differing in level of effort on blood pressure and arterial stiffness.
METHODS:
Thirty-two men performed 3 sets at 75% of 1-RM during the bench press and squat exercises to failure (
RESULTS:
A main effect of time (
CONCLUSIONS:
Training to failure should be discouraged to avoid acute increases in blood pressure and arterial stiffness.
Introduction
Cardiovascular diseases are one of the leading causes of mortality and disability worldwide [1]. High blood pressure has been considered as one the main risk factors to develop cardiovascular diseases [2]. More recently, a marker of arterial ageing known as arterial stiffness has also been proposed as a relevant risk factor for cardiovascular diseases [3]. Given the huge economic burden derived from cardiovascular diseases [4], identifying modifiable behavioural patterns and non-pharmacological interventions that may contribute both to controlling blood pressure and to delaying the arterial stiffening process inherent to aging has received considerable research attention [5].
Aerobic-based exercise has proven to be beneficial for reducing both blood pressure and arterial stiffness [6], Several meta-analyses have also shown that blood pressure may be decreased as a result of both [7, 8] chronic and acute (i.e., within 24 hours after a single session) [9] exposure to resistance training. However, the effect of resistance training on arterial stiffness is not conclusive. Indeed, both increases and decreases in arterial stiffness have been reported for healthy young adults as a result of either chronic [8, 10] or acute [11, 12] exposure to resistance training. There is compelling evidence that resistance training is the most effective method to increase muscular strength [13], which is negatively associated with the emergence of cardiovascular diseases [14] and positively with life expectancy [15]. Therefore, it is very important to elucidate how the different resistance training variables (e.g., choice of exercises, intensity, volume, movement velocity, etc.) can be manipulated to enhance both muscular strength levels and arterial stiffness.
The time elapsed between the end of a resistance training session and the measurement of arterial stiffness may be one of the factors that explain the variance in previous findings regarding the acute effect of resistance training on arterial stiffness. An increase in arterial stiffness has been reported within the 20 minutes after completing a resistance training session [12, 16, 17], while a decrease in arterial stiffness has been found after 30–60 minutes [11]. These results suggest that arterial stiffness may require more time than blood pressure until returning to (or going below) baseline levels following a resistance training session [9]. In this regard, it would be interesting to determine the immediate (e.g., after 5–10 minutes) and delayed (e.g., after 24 hours) effects of resistance training on both blood pressure and arterial stiffness.
Another factor that may contribute to explain the variance between the findings of previous studies examining the acute effect of resistance training on arterial stiffness is the level of effort incurred during resistance training (i.e., number of repetitions performed with respect to the maximum possible number of repetitions). Traditionally, resistance training sets have been performed to muscular failure (i.e., maximizing the level of effort) to develop muscle mass and strength [18]. However, there is currently evidence that training to failure does not provide the optimal stimulus to maximize muscular strength levels [18, 19]. Indeed, performing only half of the maximum possible number of repetitions has been recommended as a possible strategy to obtain comparable, if not higher, improvements in muscular strength while reducing the fatigue induced by training [18, 20]. Therefore, it would be important to elucidate whether the acute changes in arterial stiffness may also be modulated by the level of effort incurred during resistance training.
The aim of the present study was to investigate the immediate and delayed effects of a resistance training session differing in the level of effort on blood pressure and arterial stiffness [5, 21, 22, 23, 24]. It was hypothesized that both blood pressure and arterial stiffness would increase immediately after training compared to baseline values, but will decrease 5-min and 24-h after training. The scarce number of similar studies did not allow us to formulate any hypothesis regarding the possible influence of the level of effort on blood pressure and arterial stiffness.
Methods
Participants
An a priori power analysis was used to compute the required sample size for the interactions of the ANOVAs using the G Power software (version 3.1.9.4, Heinrich Heine University, Düsseldorf, Germany) considering a medium effect size of 0.25, an alpha of 0.05, a power of 0.95, 2 groups, 4 measurements, and the correlations between repeated measures of 0.60. A total sample size of 30 participants was deemed suitable. Therefore, we recruited 32 young physically active men who volunteered to participate in this study by providing verbal consent. They were randomised into two groups of 16 participants: low level of effort (age
Study design
A single-blind randomised study design was used to examine the immediate and delayed effects of a resistance training session differing in the level of effort on blood pressure and arterial stiffness. Participants were randomised into high-effort and low-effort training groups, and the researcher who performed the assessments of blood pressure and arterial stiffness before and after training was blind to the experimental group. Each participant attended the laboratory on three separate days. The first session was used for anthropometric measurements, familiarise the participants with the testing protocols, and estimate the one-repetition maximum (1RM) during the bench press and squat exercises. In the second session a resistance training session was held consisting of 3 sets at the 75% 1RM during the bench press and squat exercises. The only difference between the experimental groups was that the high level of effort group performed all sets to muscular failure, while the low level of effort group performed approximately half of the maximum possible number of repetitions per set. Blood pressure (systolic blood pressure [SBP], diastolic blood pressure [DBP], and mean arterial pressure [MAP]) and arterial stiffness (pulse wave velocity [PWV]) were measured in the second session before training (Pre), immediately after training (Post 1), and 5 minutes after training (Post 2). The same variables were measured at rest in the third session which was held 24 hours after the completion of the resistance training session (Post 3).
Procedures
Assessment of the one-repetition maximum
Height (Seca 213, Hans & Ruth, Barcelona, Spain) and body mass (Seca 869, Seca Ltd., Hamburg, Germany) were assessed at the beginning of the session. The 1RM during the bench press and squat exercises was estimated consecutively using standard testing procedures through the individual load-velocity relationship [27, 28]. A standardised warm-up based on 5 minutes of jogging, joint mobility exercises, and 1 set of 5 repetitions against an external load of 20 kg was performed before the initiation of the incremental loading test used to estimate the bench press 1RM. Another set of 5 repetitions against 20 kg was performed as a specific warm-up prior to the initiation of the incremental loading test used to estimate the squat 1RM. The initial external load of the incremental loading test was set at 20 kg for both exercises and was progressively increased in 10 kg until the attained mean velocity was lower than 0.50 and 0.70 m
The bench press and squat exercises were performed in a Smith machine (Multipower Fitness Line, Peroga, Murcia, Spain) coupled with a linear velocity transducer (T-Force system; Ergotech, Murcia, Spain). The bench press exercise was performed lying in a supine position over a bench, holding the bar with arms spread to a position slightly wider than the shoulders, and performing an isometric pause of 1–2 seconds with the bar in contact with the chest prior to executing the concentric phase at the maximum possible velocity. The squat technique involved the participants standing with their knees and hips fully extended, and the barbell held across the top of the shoulders and upper back. Participants squatted until their thighs were parallel to the floor and immediately after they performed the concentric phase at the maximum possible velocity.
The individual relationship between absolute load (kg) and mean velocity was established by means of a linear regression for each exercise. The 1RM was estimated from the individual load-velocity relationships as the load linked to a mean velocity of 0.17 and 0.33 m
Comparison of blood pressure and arterial stiffness between the different training groups and time points
Comparison of blood pressure and arterial stiffness between the different training groups and time points
Results are presented as mean
Participants performed a standardised warm-up consisting of 5 minutes of jogging, joint mobility exercises, and 3 sets of 4 repetitions during the bench press and squat exercises against three incremental loads (30% 1RM, 50% 1RM, and 70% 1RM). Thereafter, participants followed one of the two protocols (low-effort or high-effort). Both groups performed 3 sets of bench presses followed by 3 sets of squats at the 75% 1RM with a 3-minute rest in between sets and exercises. The difference between the experimental groups was that the high level of effort group performed all sets to muscular failure, while the low level of effort group stopped the set when execution velocity decreased 20% for the bench press and 15% for the squat as compared to the fastest repetition of the set, thereby performing approximately half of the maximum possible number of repetitions per set. Participants were instructed to perform all repetition at the maximum possible velocity.
Blood pressure and arterial stiffness measurements
Ambulatory Blood pressure (SBP, DBP, and MAP) and arterial stiffness (PWV) were measured 4 times in both groups: before training (Pre), immediately after training (Post 1), 5 minutes after training (Post 2), and 24 hours after training (Post 3). According to the evaluation protocol recommended for the used assessment device (i.e., Mobil-O-Graph PWA; I.E.M., Stolberg, Germany), all measurements were taken with participants sitting on a chair, both feet resting completely on the floor, palms face up and the cuff located on the left arm [12].
Statistical analyses
Descriptive data are presented as means and standard deviations (SD). The normal distribution of the data (Shapiro-Wilk test) and the homogeneity of variances (Levene test) were confirmed (
Standardized differences (95% confidence intervals) in systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), and pulse wave velocity (PWV) observed for the low-effort and high-effort groups.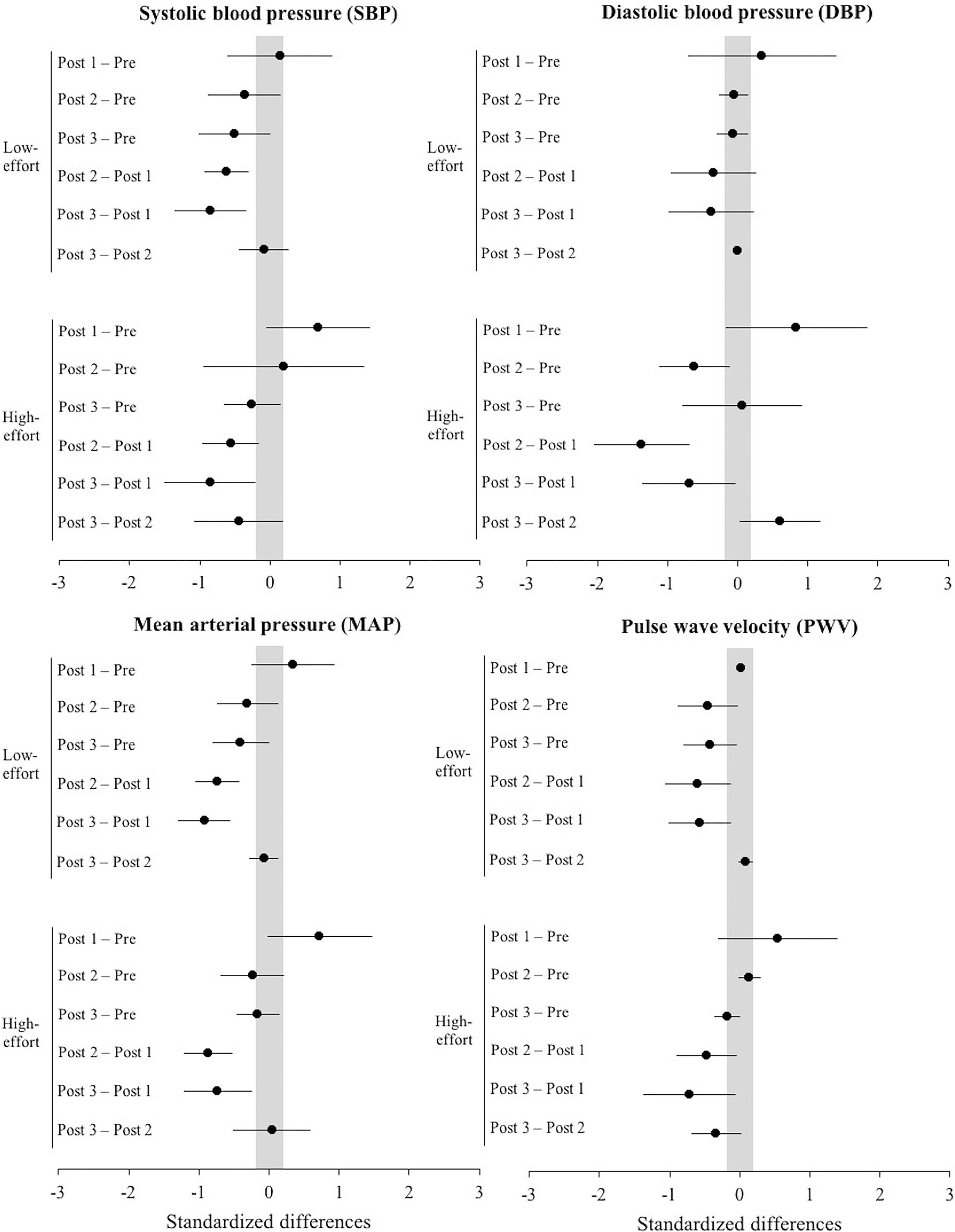
Standardized differences (95% confidence intervals) in systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), and pulse wave velocity (PWV) between the low-effort and high-effort groups. The changes were calculated for the three measurements collected after training (Post 1, Post 2, and Post 3) with respect to the pre-training data (Pre).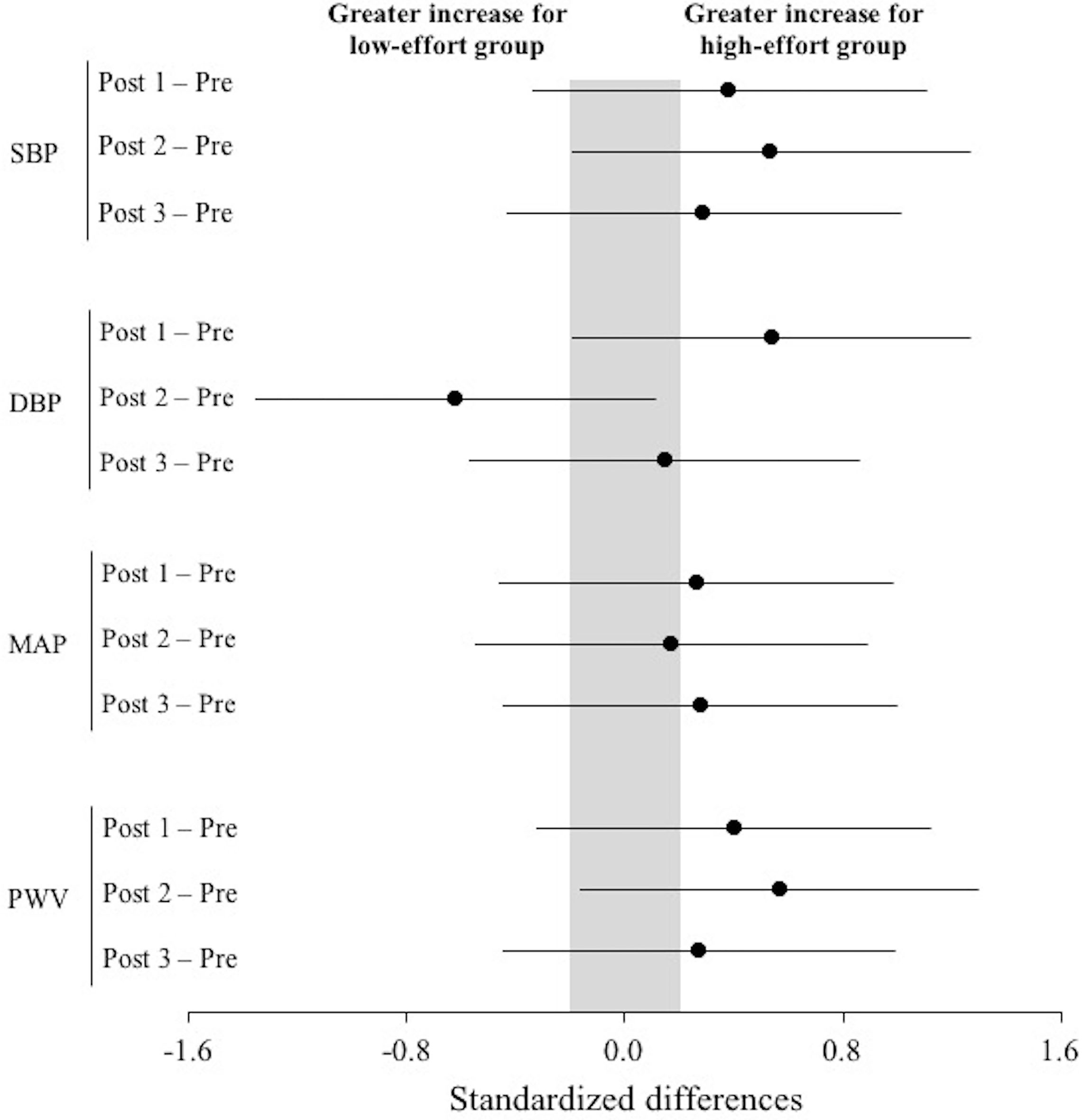
All dependent variables (SBP, DBP, MAP, and PWV) revealed a significant main effect of time (
Regardless of the training group, small to large higher values of all variables were generally observed immediately after training (Post 1) compared to the other time points (i.e., Pre, Post 2, and Post 3) (Fig. 1). When the changes with respect to Pre values were compared between the high-effort and low-effort groups (Fig. 2), it was observed that the increases for the high-effort group were higher than a ES of 0.20 compared to the low-effort group at Post 1 for SBP, DBP, MAP and PWV, at Post 2 for SBP and PWV, and at Post 3 for SBP, MAP, and PWV. The correlations at the different time points between SBP and MAP ranged from 0.85 to 0.94, between SBP and PWV ranged from 0.94 and 0.97, and between MAP and PWV ranged from 0.79 to 0.94.
Discussion
This is the first study to examine the immediate and delayed effects of a resistance training session differing in the level of effort on blood pressure and arterial stiffness. The level of effort was objectively monitored by the loss of velocity during each resistance training set [23]. Supporting our hypothesis, both groups reported an increase in the magnitude of all dependent variables immediately after the resistance training session (Post 1), while they returned to baseline levels (or even lower) 5 minutes (Post 2) and 24 hours (Post 3) after completing the resistance training session. Interestingly, the magnitude of the changes in SBP and PWV were always meaningfully higher (ES
Even though both groups performed the resistance training session against the same relative load (75% 1RM) and the repetitions were always performed at the highest possible velocity, it appears that performing approximately half the maximum number of repetitions per set has some acute positive effects on arterial stiffness as compared to performing repetitions until reaching muscular failure. It should be noted that the low-effort group presented lower increments in SBP and PWV during all post-training measurements compared to the high-effort group. These findings are consistent with those previously reported that suggest that resistance training to muscular failure pose a cardiovascular threat [17, 27, 29]. Consequently, the results of the present study suggest that, from a health perspective – and more specifically for cardiovascular health –, it may be beneficial to reduce the level of effort during resistance training session. Thus, performing half the maximum number of repetitions per set could be effective to increase strength level [22, 24], while avoiding the potential adverse effects of training to failure. However, in line with previous studies [18, 20], we also observed that blood pressure and arterial stiffness returned to baseline levels 5 minutes and 24 hours after completing the resistance training session.
Some studies have reported an increase in PWV when exercising against low and moderate loads (
Several studies have advised against resistance training due to its possible negative effect on cardiovascular health [10, 12, 26]. However, it is plausible that these negative effects have been caused by the high level of effort demanded in training (i.e., repetitions performed to failure). Therefore, since training to failure is not necessary to promote strength training adaptations [18, 19], it could be recommended to reduce the level of effort (e.g., performing half the maximum number of repetitions per set) during resistance training to avoid the undesirable effects of training to failure on health parameters. Our data support that performing 3 sets of an upper-body exercise (bench press) followed by 3 sets of a lower-body exercise (squat) against the 75% 1RM may induce positive effects on blood pressure and arterial stiffness when the level of effort is reduced. The main limitation of the present study could be the use of young physically active men as study participants. In this regard, it would be advisable to conduct similar studies with other populations (e.g., older adults and cardiovascular patients) to elucidate whether the present findings could be extrapolated to health condition groups. In addition, more studies are required to explore the acute effect of different levels of effort and exercises and, more importantly, the chronic effects of different types of resistance training on arterial stiffness.
Conclusions
Both training groups reported an increase in blood pressure and arterial stiffness immediately after the resistance training session, while blood pressure and arterial stiffness returned to baseline levels 5 minutes and 24 hours after completing the resistance training session. Regardless of the post-session measurement (i.e., Post 1, Post 2, and Post 3), SBP and PWV were lower for the low-effort group. Therefore, the reduction of the level of effort during resistance training seems to be associated with lower values of blood pressure (especially SBP) and arterial stiffness. The results of this study suggest that performing half the maximum repetitions for a given set could not only be beneficial in terms of sports performance, but could also yield positive effects in cardiovascular health. However, these results remain to be confirmed in other age groups, females, or cardiovascular patients.
Author contributions
CONCEPTION: Manuel Antonio Rodríguez-Perez and Manuel Alcaraz-Ibáñez.
PERFORMANCE OF WORK: Manuel Antonio Rodríguez-Perez and Daniel Lorente-Camacho.
INTERPRETATION OR ANALYSIS OF DATA: Manuel Antonio.
Rodríguez-Perez, Manuel Alcaraz-Ibáñez and Amador García-Ramos.
PREPARATION OF THE MANUSCRIPT: Manuel Antonio Rodríguez-Perez, Manuel Alcaraz-Ibáñez and Amador García-Ramos.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Manuel Antonio Rodríguez-Perez, Manuel Alcaraz-Ibáñez, Daniel Lorente-Camacho and Amador García-Ramos.
SUPERVISION: Manuel Antonio Rodríguez-Perez, Manuel Alcaraz-Ibáñez and Amador García-Ramos.
Ethical considerations
This research was approved by the Ethics Committee of the University of Almería, reference UALBIO2018/008. All participants granted informed consent to participate in the study.
Funding
This work was supported by Ministerio de Economía y Competitividad (MINECO), Spain, Plan Nacional de I
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
None to declare.