
Abstract
BACKGROUND:
Active interventions for pes planus, including short-foot exercises (SF) and toe-spread-out exercises (TSO), aim to continuously support the medial longitudinal arch (MLA) by activating the abductor hallucis (AbdH) muscle. However, compensatory movements, such as ankle supination and/or plantar flexion, often occur during these exercises.
OBJECTIVE:
To examine the effects of a novel exercise, i.e., the toe-tap (TT) exercise on AbdH activity and MLA angle.
METHODS:
A total of 16 participants with pes planus participated in this study. Participants performed SF, TSO, and TT exercises. Electromyographic activity of the AbdH and MLA angle during three AbdH contraction exercises were recorded using surface EMG system and digital image analysis program, respectively. The differences in outcome measures among the three exercises were analyzed using one-way repeated-measures analysis of variance.
RESULTS:
The EMG activity of the AbdH was significantly greater during the TT exercise compared to the SF and TSO exercises. The MLA angle was significantly smaller during the TT exercise compared with the SF and TSO exercises.
CONCLUSIONS:
These findings suggest that the TT exercise could be effective in activating the AbdH and increasing height of the MLA, as part of a sports rehabilitation program for individuals with pes planus.
Introduction
Pes planus is defined as lowering or flattening of the medial longitudinal arch (MLA) [1]. Pes planus is associated with foot malalignment, manifested as excessive pronation of the foot, rear foot valgus, and abduction of the midfoot on the rearfoot [1, 2, 3, 4]. Pes planus is also responsible for overuse injuries, including tibialis posterior tendinitis [5], patellofemoral pain syndrome [2], and plantar fasciitis [1, 6]. Therefore, clinicians should consider interventions that increase the MLA angle to prevent overuse injuries related to pes planus.
The MLA is supported not only by passive structures such as the plantar fascia and spring ligament, but also by intrinsic muscles, including the abductor hallucis (AbdH), and extrinsic muscles, including the tibialis anterior and tibialis posterior [1, 7, 8]. Muscle contraction of the AbdH, which originates in the calcaneus and inserts into the medial great toe, results in abduction and flexion of the first metatarsophalangeal (MTP) joint [1], which moves the origin and insertion points of AbdH close, and consequently increases and supports the MLA [7, 8, 9, 10, 11]. Previous studies showed that fatigue of the AbdH [12], and decreased muscle activity therein [13], resulted in increased navicular drop (ND) (i.e., decrease in MLA angle) in the standing position, which shows the important role of the AbdH in supporting the MLA. Although extrinsic muscles can be overactivated to compensate for a weakened AbdH in individuals with pes planus [14, 15], prolonged overactivation of extrinsic muscles results in muscle fatigue and microtrauma, consequently contributing to tendinitis and/or overuse injury [11, 16, 17, 18]. Thus, AbdH strengthening exercise programs should support the MLA and prevent secondary injuries in individuals with pes planus.
To strengthen the AbdH, the short-foot (SF) exercise, which entails pulling the first metatarsal head toward the heel without toe flexion, and the toe-spread-out (TSO) exercise, which entails flexion and abduction of the first and fifth MTP joints, are often prescribed and performed in the sport and rehabilitation field [9, 19, 20, 21]. Previously, Jung et al. [9] demonstrated that the SF exercise effectively facilitated AbdH activation compared to the toe-curl exercise, which involves flexing the first to fifth interphalangeal (IP) and MTP joints. This effect is due to the fact that SF exercise does not require toe IP flexion caused by contraction of the long toe flexors. Kim et al. [20] reported that the TSO exercise was more effective for AbdH activation than the SF exercise as a result of an additional primary physioanatomical action (i.e., abduction of the first MTP) of the AbdH during the TSO exercise. However, the TSO exercise does not fully reflect the secondary action of the AbdH muscles, such as flexion of the first MTP, because the proximal phalanx of the great toe moves from an extended to neutral position during TSO exercises [20]. Therefore, to induce maximal effort in the AbdH, a novel exercise that incorporates both actions (e.g., abduction and flexion of the first MTP) of the AbdH muscle is required.
A newly developed exercise, called the toe-tap (TT) exercise, was designed to activate AbdH based on the physioanatomical actions of the AbdH muscle. The TT exercise is performed by abducting and flexing the first MTP joint with the sole of foot resting on an inclined wooden board. During the TT exercise, the toes are placed outside the front edge of the inclined wooden board, which allows for flexing of the first MTP joint while abducting the first MTP joint.
When the goal of an exercise is to strengthen the muscle, it has been recommended to activate the muscle to greater than 40% of the maximum voluntary isometric contraction (MVIC) [22, 23]. However, it remains unclear whether sitting SF exercises can stimulate AbdH muscle strength adaptation due to the variation in AbdH muscle activity (range:
Methods
Participants
A total of 16 participants (8 males and 8 females) with pes planus participated in this study. To determine pes planus, the alignment of dominant foot (i.e., kicking leg side) was examined [14]. Pes planus was assessed according to scores on the ND test [14, 24, 25]. The ND test scores were measured twice, and the average was used to define pes planus (ND
General characteristics of the subjects
General characteristics of the subjects
The required sample size was calculated based on the effect sizes (mean difference/pooled standard deviation, calculated using G-Power software) in our pilot study, which included five subjects, because the effects of the TT exercise on AbdH muscle activity have not been demonstrated previously. The results of the pilot study indicated that at least 15 participants would be required to detect a difference in AbdH muscle activity between exercises with a power of 0.80 at a significance level of 0.05, based on an effect size of 0.7. Prior to the experiment, all participants were given a thorough explanation of the intervention protocols, and all signed an informed consent form approved by the Institutional Research Review Committee of Inje University.
Surface electromyography (EMG) signals indicating AbdH muscle activity were collected and analyzed using a 2EM instrument (4D-MT; Relive, Gimhae, Korea). The sampling rate was 1,000 Hz. The raw signal was filtered using a bandpass digital filter between 0 and 500 Hz. The root-mean-square (RMS) values were calculated. Prior to data collection, the skin was cleaned with alcohol to optimize electrical conductance by reducing skin impedance. The electrodes were placed approximately 1–2 cm posterior to the navicular tuberosity and anterior to an imaginary line drawn over the anterior margin of the medial malleolus, with a 20 mm distance between center-to-center electrodes [9, 26]. The ground electrode was attached to the medial malleolus. The MVICs were measured to normalize the EMG data using the following manual muscle-testing position: an examiner applied resistance to the medial side of the proximal phalanx of the great toe while maintaining a neutral heel position. The participant was asked to perform maximal abduction of the great toe against the resistance provided by the examiner [20]. EMG data were collected for 5 s, with 3 s of data used to determine the mean MVIC amplitude (the first and last seconds of EMG data were removed). MVIC measurements were performed twice for each participant, and the mean value of two MVIC trials was used for normalization. A 1-min rest was provided between MVIC trials to reduce muscle fatigue.
The AbdH muscle activity data were recorded for 5 s when performing each AbdH contraction. Each exercise was repeated three times, and the mean EMG activity of the AbdH (middle 3 s of each trial) was calculated. The mean AbdH muscle activity of three test trials for each exercise was expressed as a percentage of the mean MVIC (%MVIC) and used for data analysis.
Measurement of the medial longitudinal arch angle.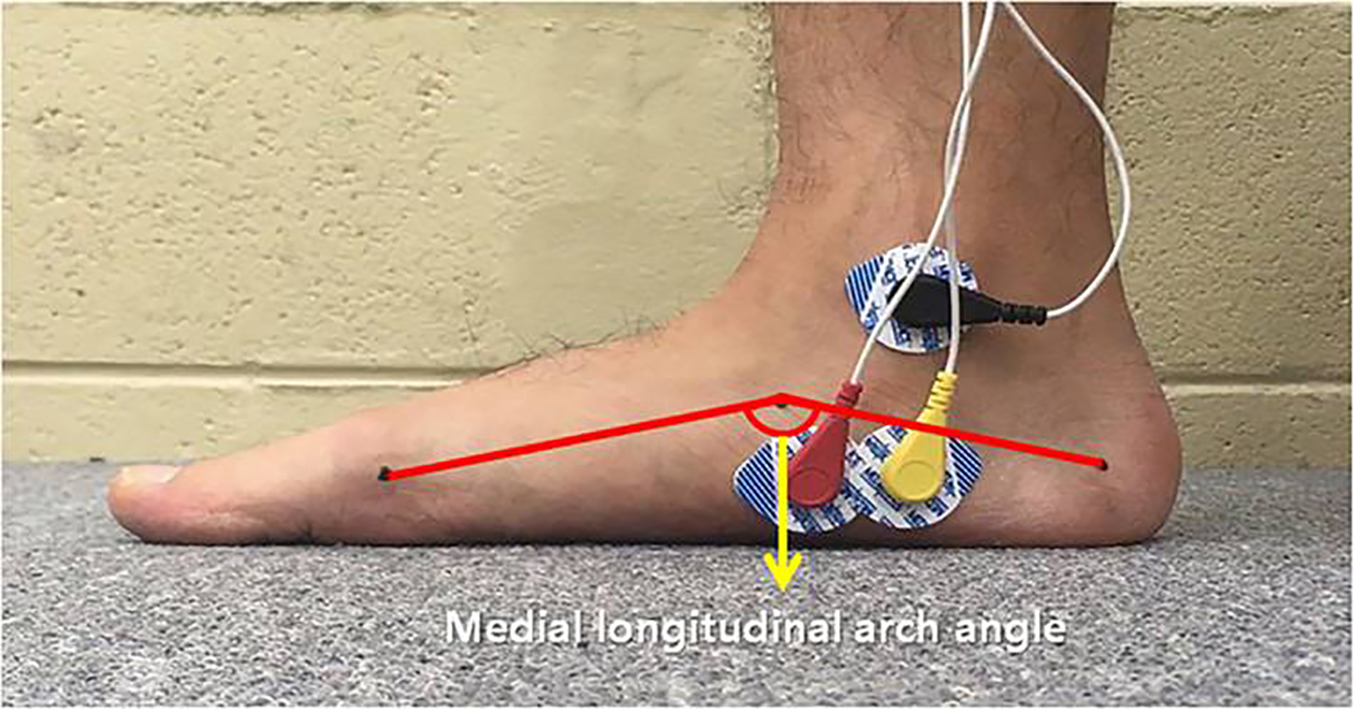
Short-foot exercise (A) and toe-spread-out exercise (B).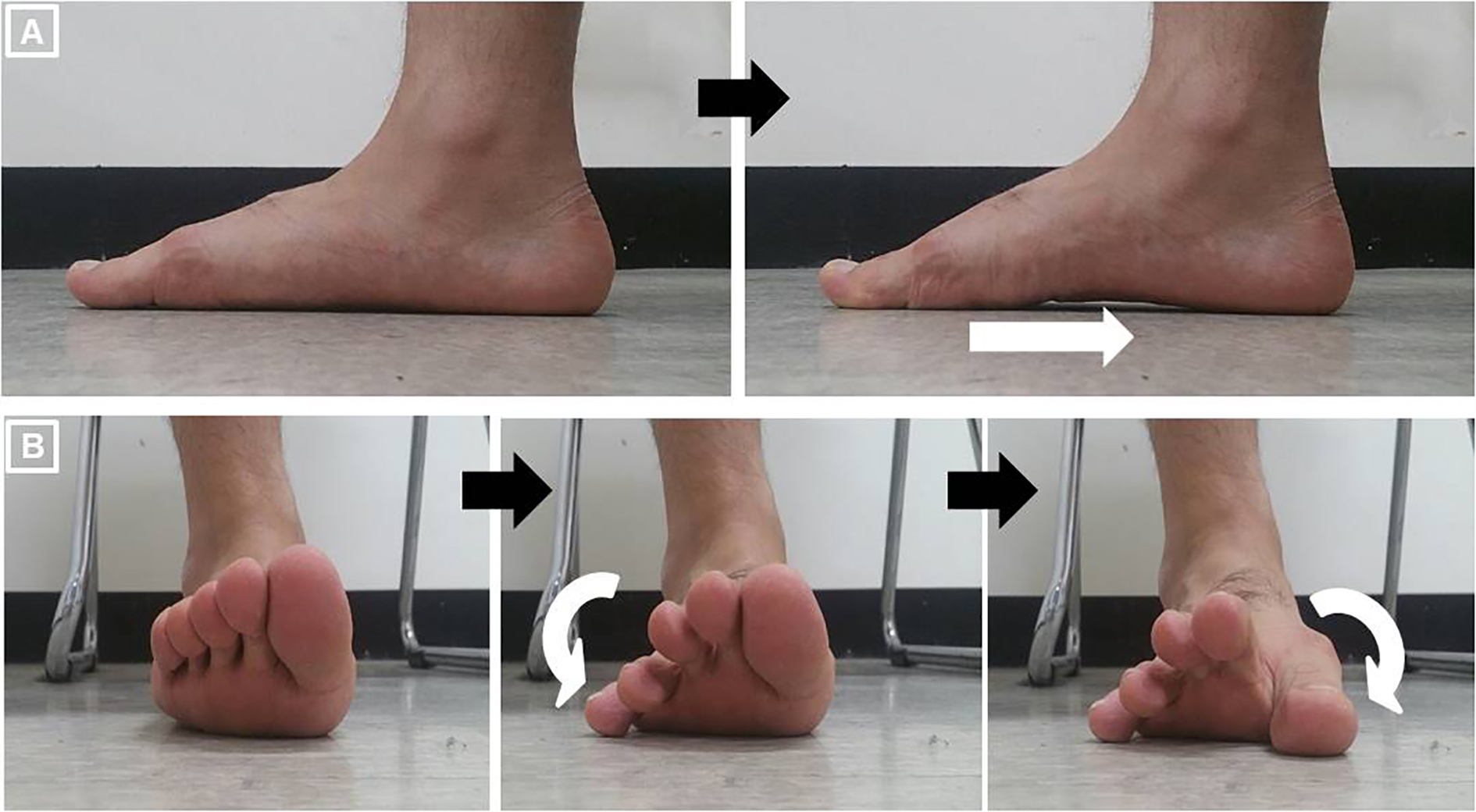
Frontal view (A, C) and sagittal view (B, D) of the toe-tap exercise.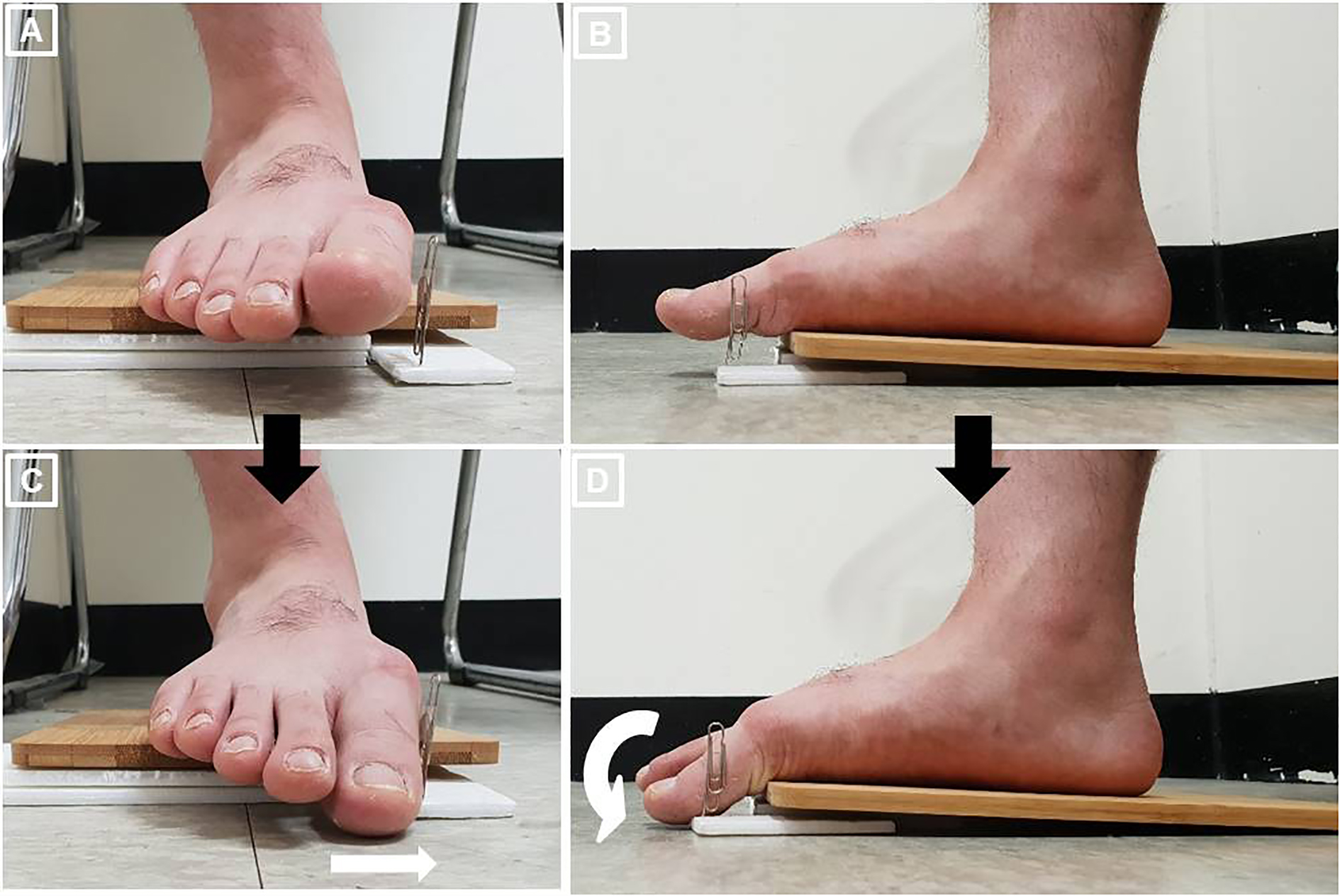
To measure the MLA angle, the examiner placed the participant’s foot on the floor, with a neutral ankle and subtalar joint position while in the sitting position, and then marked the medial side of the calcaneus, medial aspect of the first metatarsal head, and navicular tuberosity in the test foot [14, 19, 27]. According to previous studies [9], the medial side of the calcaneus was 30 mm from the most posterior region of calcaneus and 30 mm from the floor in females, while it was 40 mm from the most posterior region of calcaneus and 35 mm from the floor in males. The first metatarsal head was palpated where the most prominent head was located distal to the first metatarsal bone, while the navicular tuberosity was palpated approximately 1 inch distally and 1 inch anteriorly from the medial malleolus [28]. The landmarks of the medial aspect of the first metatarsal head and navicular tuberosity were determined as the midpoint of the medial aspect of each palpated bony structure. The landmarks were finally marked where both examiners who had significant experience in motion capture technology. A smartphone camera (iPhone SE; Apple, Cupertino, CA, USA) was placed 0.5 m from the medial side of the foot to take images of the marked points during the exercises. To minimize noise from electrical equipment, the smartphone mode was changed to flight mode [29]. The smartphone was placed parallel to the floor, with its lens placed at the level of the navicular tuberosity. All images (4,032
Comparison of abductor hallucis muscle activity and medial longitudinal arch angle among three abductor halluces contraction exercises
Comparison of abductor hallucis muscle activity and medial longitudinal arch angle among three abductor halluces contraction exercises
Abbreviation: AbdH, abductor hallucis; MVIC, maximal voluntary isometric contraction; MLA, medial longitudinal arch; SF, short-foot; TSO, toe-spread-out; TT, toe-tap.
Compensatory ankle plantar flexion movements (A: elevation of the rear edge of the wooden board, B: elevation of calcaneus) during the toe-tap exercise. 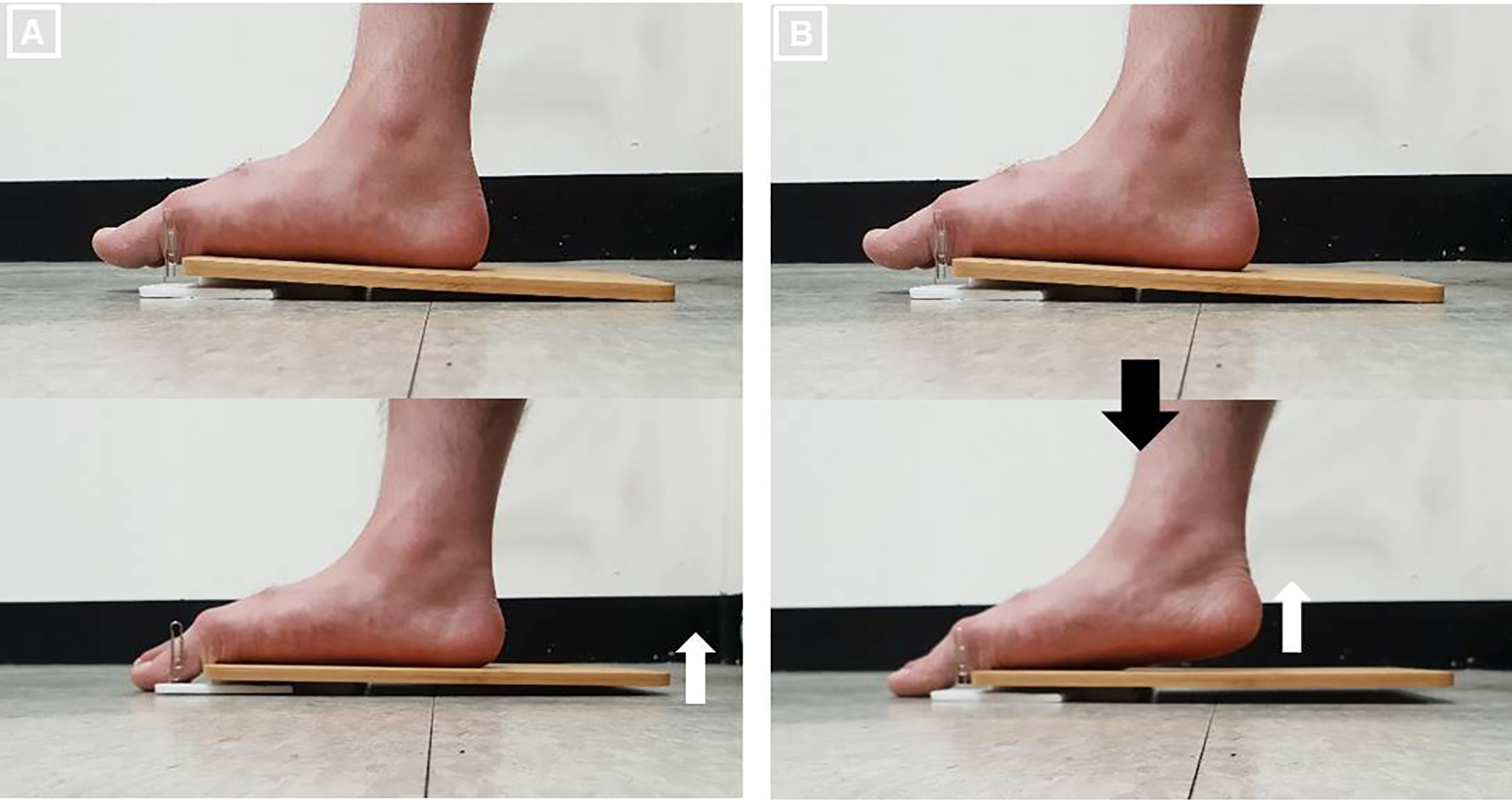
The intra-class correlation coefficients (ICCs) of outcome measures were assessed in our reliability study. The ICCs indicated very high reliability of AbdH muscle activity (SF exercise: 0.855, TSO exercise: 0.934, TT exercise: 0.920) and MLA angle (SF exercise: 0.978, TSO exercise: 0.954, TT exercise: 0.989).
All participants performed three AbdH contraction exercises (SF, TSO, and TT exercises) in a randomized order. During all exercises, the participant was seated on a chair with 90
For the SF exercise, each participant moved the first metatarsal head toward the heel without toe flexion, to shorten the foot in an anterior-posterior direction while the forefoot and heel remained on the floor, with a neutral ankle and subtalar joint position [14, 19] (Fig. 2A). For the TSO exercise, each participant extended all toes while the metatarsal heads and heel remained on the floor. each participant was instructed to lower the little toe in the lateral direction, and then to lower the great toe in the medial direction while maintaining the ankle and subtalar joint in the neutral position [20] (Fig. 2B).
Although the SF and TSO exercises were performed in a neutral ankle position, to perform the TT exercise the test foot was placed on an inclined wooden board (30
Before the test period, participants practiced all AbdH contraction exercises under the supervision of the principal examiner until they were able to perform the exercises correctly without compensatory movements. During the test period, participants were asked to perform each exercise with maximum effort; three repetitions of each AbdH contraction exercise were performed, with each being held for 5 s.
Statistical analyses
The Shapiro-Wilk test was performed to test the normality of the distribution of the outcome measures. A one-way repeated-measures analysis of variance was used to assess the statistical significance of differences in AbdH activation and the MLA angle. If a significant main effect of EMG activity or MLA angle was found, the post-hoc analysis using the Bonferroni correction was performed. The data are expressed as the mean
Results
Data on AbdH EMG activity and MLA angle during the AbdH contraction exercises are shown in Table 2. All outcome measures showed a normal distribution (
Discussion
The findings of this study indicate increased AbdH muscle activity during the TT exercise compared to the SF and TSO exercises (
Another possible explanation for the increased AbdH muscle activity seen during the TT exercise is the effects of tactile feedback. Because isolated abduction of the hallux is difficult to perform [20, 26, 32], it is not easy to maintain (or recognize) abduction of the hallux during exercise. In this study participants were instructed to touch the fixed target pin during the TT exercise which may help guide abduction of the great toe and thus influence AbdH muscle activity.
In the present study, all exercises were performed in the neutral subtalar position without unwanted ankle plantar flexion, but it was difficult to rule out isometric contraction of the plantar flexors during the exercises. Previous study reported increased muscle activity of the extrinsic ankle plantar flexors (e.g., the gastrocnemius and soleus) during maximum toe flexion while maintaining a neutral ankle joint position [33]. These findings suggest that unwanted contraction of the extrinsic ankle plantar flexors can occur during flexion of the MTP joint although visible ankle plantar flexion did not occur. It has been suggested that selective activation of the AbdH is complicated due to the lack of requirement for selectively activating the AbdH during daily activities [32, 34]. Ankle plantar flexion movement is considered one of the compensatory movements in AbdH activation exercises [34]. Therefore, it is possible that the plantar flexors, commonly used in daily activities, may be recruited to compensate for AbdH activation during movements of the first MTP joint and first metatarsal head in the TSO and SF exercises, respectively. In contrast to these exercises, TT exercises were performed on an inclined wooden board, which allowed for visible detection of excessive plantar flexion force during exercise by monitoring elevation of the rear edge of the wooden board from the floor. Thus, it is possible that TT exercises minimize unwanted extrinsic plantar flexor activation, which causes increases in AbdH muscle activity. However, we did not measure changes in the activation of the extrinsic plantar flexors in this study; thus, this hypothesis should be explored in a future study.
The MLA angle decreased significantly during the TT exercise compared to the SF and TSO exercises in the present study (
In general, intrinsic muscles play a more important role in segmental dynamic stability and postural control than extrinsic muscles [21, 35]; thus, exercises strengthening the intrinsic muscles, especially the AbdH (which is a dynamic elevator of the MLA), should be emphasized in the clinical setting. The SF exercise has been suggested to strengthen the AbdH in previous studies [9, 14, 21]. However, a relatively large standard deviation of AbdH muscle activity was reported during the SF exercise in previous studies (approximately 18–20% MVIC) [9, 14, 20], as well as in the present study (approximately 18–19% MVIC). These findings may be attributed to variability among subjects in the ability to recruit the AbdH muscle during the SF exercise, due to the unfamiliar movements involved in that exercise [34]. However, the standard deviation of AbdH muscle activity was smaller during the TT exercise (approximately 8–9% MVIC) compared to the SF exercise, while AbdH muscle activity was about two times greater in the TT exercise than the SF exercise. These findings suggest that the TT exercise is easier and more efficient for increasing AbdH muscle activity.
Because this study is the first to investigate the TT exercise, there are no previous studies to which the results can be compared. However, the TT exercise requires only a physioanatomical action of the AbdH, as it is performed by flexion and abduction of the first MTP joint. Also, compensatory ankle plantar flexion force can be easily identified by movement of a wooden board during the TT exercise. Although it has been reported that muscle training (e.g., EMG biofeedback training) is effective to prevent compensatory movements and facilitate selective muscle contraction [36], it is difficult to apply these training methods in the clinical setting due to time and cost constraints. On the other hand, the TT exercise requires only an inclined wooden board to prevent compensatory movement; thus, it is assumed that the TT exercise can be easily applied and utilized in clinic.
This study has several limitations. First, we did not measure the activity of other intrinsic and extrinsic foot muscles, although the MLA is affected by various foot muscles. Also, we did not examine the long-term effects of the TT exercise on the EMG activity of the AbdH or the MLA angle. Thus, future studies should determine the long-term effects of the TT exercise on the EMG activity of various intrinsic and extrinsic foot muscles, and on the MLA angle. Second, we only obtained ND test scores when recruiting participants. Additional studies are required that include other characteristics (e.g., foot size, MLA angle in a relaxed position, and foot posture index) of participants to provide more context for our results. Finally, we did not completely control for the noise and distortion associated with smartphone imaging.
Conclusions
The current study indicates that AbdH muscle activity significantly increases during the TT exercise compared to the SF and TSO exercises, while the MLA angle is significantly decreased, similarly. Thus, TT exercise may be more effective than either of SF and TSO in activating the AbdH and increasing the MLA angle in individuals with pes planus. Thus, clinicians should consider the TT exercise when designing training programs to increase AbdH muscle activity and the MLA angle in individuals with pes planus.
Author contributions
All authors contributed equally to this work.
Ethical considerations
Prior to the experiment, all participants were given a thorough explanation of the intervention protocols, and all signed an informed consent form approved by the Institutional Research Review Committee of Inje University.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
None declared.