
Abstract
BACKGROUND:
Dynamic knee valgus (DKV) is a known risk factor for acute and chronic knee injuries and is more frequently diagnosed in females. A real-time single-leg squat test (SLST) could screen for DKV to prevent injuries.
OBJECTIVE:
To compare the differences in lower extremity strength and range of motion (ROM) in female soccer athletes with and without DKV during an SLST.
METHODS:
Eighteen subjects with DKV (DKV group) and 18 subjects without DKV (control group) during a single-leg squat were included. Hip strength (flexion, extension, abduction, adduction, internal rotation, and external rotation) was measured with a hand-held dynamometer. Hip ROM (internal and external rotation), and ankle ROM (dorsiflexion with the knee flexed and extended) were measured. Independent t-test was used to compare the averages of the groups.
RESULTS:
There were significant differences in hip abduction to adduction strength ratio (DKV: 1.48
CONCLUSION:
The hip abduction to adduction strength ratio and gastrocnemius and soleus flexibility may be associated factors in dynamic knee valgus and therefore should be assessed and treated, if indicated, as a possible preventive measure in female athletes with this variation.
Introduction
Dynamic knee valgus (DKV) movement during exercises can predict risk of injury, especially anterior cruciate ligament (ACL) sprains [1, 2, 3]. Also, an ACL sprain increases the chance of knee instability, meniscus tear, and knee osteoarthritis [4]. DKV also increases the chance of chronic injuries such as patellofemoral pain [5]. Contralateral pelvic drop, knee valgus, femoral internal rotation, and tibial internal rotation movements occur during weight-bearing maneuvers with DKV [6]. The knee joint should perform flexion and extension in the sagittal plane; however, frontal plane knee motion such as valgus knee movement is an abnormal pattern that increases the risk of knee injuries [7, 8]. DKV occurs to a higher degree in females compared to males when performing single-leg squats [9, 10]. Asymmetry of unilateral hip rotation, weaker hip abduction, and external rotation strength are predictive factors for abnormal knee movements in dynamic situations; rather than the Q-angle which is a static anatomical characteristic in females [11].
Dynamic movement-based assessments are applied to predict injury risks for pre-participation screening [12]. Three-dimensional (3D) motion analysis is the gold standard method to analyze knee movement; however, it is expensive, time consuming, and not suitable for large number screening [13]. Real-time observational screening is easy to apply, and is a low-cost assessment of knee valgus [14]. Ekegren et al. [15] reported that observational risk screening to evaluate DKV is a practical and cost-effective method, and highly reliable. Two-dimensional (2D) single-leg squat test (SLST) is commonly applied on the field and in the laboratory due to enhanced practicality to test DKV [14, 16]. Also, the reliability of the SLST is very good (0.78–0.89) [17].
Identifying the risk factors of DKV is important for the design of knee injury prevention programs [18]. Hip muscle strength is related to DKV during SLST; however, there are differences between sex [11, 19]. Although several studies have investigated strength and range of motion (ROM) differences with DKV during SLSTs, those studies did not distinguish the differences between sex. Therefore, the influence of strength and ROM in SLSTs may not be clearly identified [9, 20, 21]. Testing DKV during a single-leg squat is important for female athletes because they present a 2 to 10 times greater ACL sprain incidence rate than males [22, 23]. Therefore, the purpose of this study was to investigate strength and ROM differences in SLST with or without DKV in females.
Methods
Subjects
Sixty-one recreational female soccer athletes were recruited for initial SLST screening from 3 university soccer clubs in Seoul, Korea. The subjects were healthy individuals, aged from 19 to 22 with no injuries experienced in the previous 6 months. Subjects who had undergone lower extremity surgery within 2 years were excluded. The demographic information of both groups is presented in Table 1. A consent form was given to all subjects prior to participation in this study. The CHA university’s Institutional Review Board approved the study prior to testing (2020/10/5).
Physical characteristics of subjects (M
SD)
Physical characteristics of subjects (M
*Values are group mean
A real-time SLST was applied in this study. The investigator was a certified athletic trainer who had 14 years of experience on the field with SLST. The subjects walked on a treadmill at 4 km/h for 5-m for a warm-up. The subjects were then asked to remove their shoes to eliminate any effect these could cause [24], and were then asked which foot they used to kick a ball to decide on the dominant leg.
Real-time single-leg squat test. (a) dynamic knee valgus. (b) control.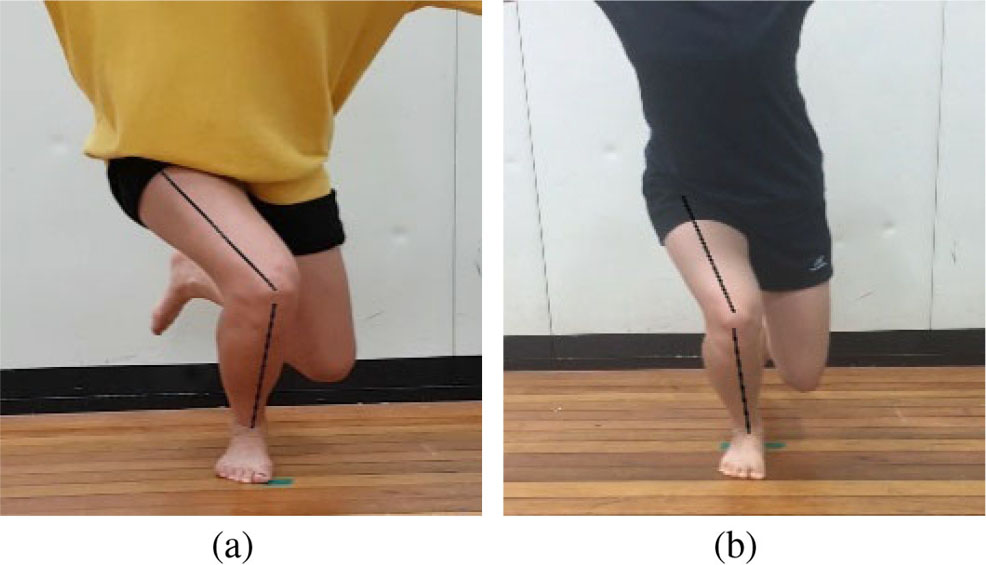
Subjects stood with the dominant foot’s second toe facing forward while the other knee was flexed to 90
The investigator was a certified corrective exercise specialist who had 15 years of experience on the field and 7 years of research experience with hand-held dynamometer strength measurement. A calibrated MicroFET2 hand-held dynamometer (Hoggan Health, Salt Lake City, UT, USA) was used to measure hip strength [25]. The intraclass correlation coefficient of hip strength measurement with hand-held dynamometer was 0.96 (95% CI, 0.80–0.99) [26]. The SLST investigator and the hip strength measurement investigator were blinded from each result.
For hip internal and external rotation strength, the subject sat on the edge of a table with the knees and hips flexed at 90
For hip abduction strength, the subject was positioned side lying with the test hip superior, abducted approximately 20
For hip adduction strength, the subject was positioned side lying with the test hip inferior. The non-test hip and knee were flexed at 90
The subject was asked to sit on a table to measure hip flexion strength. The subject’s arms were crossed with hands on shoulders. The investigator placed the dynamometer 3 cm superior to the patella and the subject was asked to push against it.
Hip extension strength was measured with the subject prone with the test side knee flexed to 90
Subjects practiced each measurement 3 times prior to performing the measurements twice, with a 1-m rest between. The average of the 2 measurements was recorded. Strength data were normalized to body mass by the following formula: (strength/body weight)
Hip internal/external ROM and ankle dorsiflexion ROM tests
A digital inclinometer (Sincon, Bucheon, Korea) was used to measure all ROM. For hip internal and external rotation, the subject lay prone with the pelvis stabilized with a belt on the table. The non-test side hip was abducted 30 degrees, and the test side knee was flexed to 90
Ankle dorsiflexion was measured with a universal goniometer with the knee extended and flexed. For the knee flexed test, the subject lay prone with the knee flexed to 90
Sample size calculation
The sample size was calculated by G-power 3.1 software (Franz Faul, Germany) based on data for strength and ROM from a previous study [19]. Considering a
Statistical analysis
Descriptive statistics were used to present the data. Distribution curves were assessed for normality. Independent samples
Normalized peak isometric strength percent between groups (%kg/ body mass)
Normalized peak isometric strength percent between groups (%kg/ body mass)
*
Ratios of the isometric hip strength between groups (%kg/body mass)
*
Range of motion values between groups
*
Hip strength
Normalized peak isometric strength data is provided in Table 2. There was no significant difference in hip strength between the 2 groups. The ratios of the isometric hip strength data are provided in Table 3. There was a significant difference in abduction to adduction strength ratio between the groups (DKV: 1.48
Hip rotation ROM and ankle dorsiflexion ROM
Hip rotation and ankle dorsiflexion ROM data are presented in Table 4. There were significant differences in ankle dorsiflexion ROM with the knee flexed (DKV: 17.22
Discussion
The purpose of this research was to investigate differences of hip strength and ankle ROM between DKV and control groups in female soccer athletes. While the landing error scoring system (LESS) or the tuck jump test are used to screen dynamic leg alignment in athletes, the SLST is easier, more practical, and a reliable test [24]. We used the SLST to differentiate whether subjects presented with DKV or a normal angle. We found that athletes with DKV presented with decreased hip abduction to adduction strength ratios and ankle dorsiflexion ROM with the knee flexed and extended.
Weak hip strength is known to be one of the important factors of knee injuries [1, 9, 25, 27]. DKV could lead to ACL injuries in athletes, especially females [7, 9, 15]. Therefore, it is important to screen for DKV to prevent knee injuries. However, our results indicated that the DKV and control groups did not reveal significant hip strength differences. Previous studies report similar results with different tests such as the drop double leg squat test, lateral step-down test, and forward lunge test [21, 29]; however, none of the previous studies differentiate their results with respect to sex. We only recruited female soccer athletes, and were able to present similar results. Thus, neuromuscular control of the hip joint may have affected DKV during the SLST rather than the strength of specific muscles [19]. Further studies are needed to identify whether neuromuscular control has a role in DKV using electromyography.
Hip muscle strength ratio is significantly different in DKV with regards to double leg squat performance [20]. We found that there was a significant difference (
There was no significant hip rotation ROM difference between the groups. This result is similar to other DKV studies, and hip rotation ROM may not be considered as a factor for DKV [19, 32]. There were significant ankle dorsiflexion ROM differences between the groups, with the knee flexed (
There are several limitations to this study. First, the study measured DKV only with SLST and did not include other types of tests for comparison. The results of other tests such as drop landing, double leg squat, lateral step-down test, and forward lunge test should be investigated. Second, we did not measure knee displacement in scale data to see the relationship. Lastly, we did not verify foot alignment during SLST. Excessive foot pronation could affect the results of the SLST.
Conclusion
Our results indicate that female soccer athletes with DKV present decreased hip abduction to adduction strength ratio and ankle dorsiflexion ROM with the knee flexed and extended. To prevent ACL sprains and PFP, training programs should include hip abduction and adduction ratio improvement, and gastrocnemius and soleus stretching to increase flexibility of the single-leg squat.
Author contributions
CONCEPTION: Young Jin Jo.
PERFORMANCE OF WORK: Young Jin Jo and Young Kyun Kim.
INTERPRETATION OR ANALYSIS OF DATA: Young Jin Jo and Young Kyun Kim.
PREPARATION OF THE MANUSCRIPT: Young Jin Jo and Young Kyun Kim.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Young Kyun Kim.
SUPERVISION: Young Kyun Kim.
Ethical considerations
IRB approval number: 1044308-202006-HR-024-02, CHA University; IRB approval date: 2020.10.5., Conditional accepted date: 2020.7.28. Written informed consent was obtained from each subject.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare no conflicts of interest.