
Abstract
BACKGROUND:
Knee osteoarthritis (KOA) is one of the most common chronic diseases impacting millions of elderly people.
OBJECTIVES:
The study compared the effects of two intensities of partial blood flow restriction (BFR) with low-intensity resistance training on quadriceps strength and cross-sectional area (CSA), and pain in people with knee osteoarthritis (PwKOA).
METHODS:
Thirty-five PwKOA, aged 50–65, participated. Quadriceps CSA was measured by ultrasonography, quadriceps strength – by isokinetic dynamometry and pain by VAS. These outcome variables were obtained at the beginning of the study and re-evaluated eight weeks after the intervention.
RESULTS:
An interaction effect was present for quadriceps CSA (
CONCLUSION:
A combination of 70% of total occlusion pressure with 30% 1RM could be beneficial in PwKOA in improving pain, and increasing the quadriceps strength. The changes in the quadriceps strength could be a predictor for knee pain.
Keywords
Introduction
One of the most common prevailing chronic diseases impacting millions of people worldwide is Knee osteoarthritis (KOA). The rate of KOA in populations is high, especially in older people. It is caused by aging, overuse, trauma, and other serious factors and leads to degenerative morphological changes. In Saudi Arabia, the incidence of KOA is 90% in older adults [1, 2, 3] and nearly 14 million adults in the US [4]. KOA results in wear and tear of articular cartilage, bony changes, and development of excess bony prominent called osteophytes. Additionally, knee pain, effusion, and knee joint dysfunction, which are common in KOA, can influence the patient’s quality of life and may lead to distress [5]. In certain countries, KOA costs society economically about 3% of the total national product throughout frequent missing of work-days due to knee pain [6].
Quadriceps weakness can attribute biomechanically to the occurrence of symptomatic KOA and the progression of cartilage degeneration [7]. It has been indicated that patients with KOA had weak quadriceps muscle [8]. Basically, resistance training exercise (isometric, isotonic, and isokinetic exercise) and aerobic exercise enhance the joint function and pain in PwKOA [9]. The American College of sports medicine recommended that resistance training should be conducted to increase the muscle strength by 60% to 70% 1-repetition maximum (1RM) and 70% to 85% 1RM to induce muscle hypertrophy [10]. It was reported that for enhancing muscle CSA, power in healthy young, and older adults the resistance should use 60–80% of 1RM at 2–4 sets of 8–12 repetitions [11]. Strengthening exercises may load the knee joint and exacerbate symptoms for PwKOA. However, decreasing resistance used in strengthening exercise to a level that does not increase the symptoms may not be sufficient to induce muscle hypertrophy [12] and increase muscle strength [13].
Blood flow restriction (BFR) training involves the application and administration of pressure by a pneumatic cuff proximal to the target muscle during strengthening exercises [14] to impede the venous outflow while keeping the arterial blood flow [15]. During occlusion in BFR, substrates like glucose and free fatty acid are rigorously diminished. Consequently, additional motor units (MUs) may have to take place progressively to maintain at least the force development without a drop [16]. Besides augmentation of motor units, BFR could enhance protein generation through phosphorylating the mammalian target of rapamycin (mTOR). The end product of S6 Kinase (S6K1) regulates mRNA translation, which is responsible for muscular hypertrophy [17]. It was found that training with BFR at 20%–30% of 1RM produces muscle hypertrophy and increases muscle strength more than the same training without BFR. Since training with low-intensity resistance exercises with concurrent BFR is a less painful technique, it could be beneficial for PwKOA [14, 18].
The amount of BFR plays a crucial role in augmenting the effect of low intensity of resistance training (RT). Eighty percent of BFR either continuously or intermittently with RT using 20% of 1RM for 12 sessions could improve activation of the biceps and triceps in healthy men [19]. Another study investigated the concurrent effect of 50% of BFR with low intensities of 1RM in healthy older men. A previous study revealed that BFR increased cross-sectional area (CSA) of thigh muscles [17]. However, the combination of partial blood flow restriction and the intensity of 1RM needed to enhance the power and volume of the quadriceps is still controversial. Thus, the present study aimed to compare two intensities of partial blood flow restriction associated with low-intensity resistance training aiming to produce a significant increase in quadriceps strength and CSA, as well as improving pain of symptomatic elderly PwKOA.
Material and methods
Participants
A total of fifty-six community-dwelling ambulatory Saudi Arabian male patients, aged 50–65 with symptomatic KOA, were eligible for this study. Participants were included if they: (a) diagnosed with KOA and Kellgren-Lawrence radiographic grade from 1 to 4; (b) aged between 50–65 years. Exclusion criteria were as follow: (a) performing routine physical exercises during the past six months; (b) suffering from health problems related to the musculoskeletal system or the cardiovascular diseases, which, in turn, negatively affecting the exercise training; (c) Visual Analog scale (VAS) scoring less than 1 or greater than 8; (d) taking non-steroidal anti-inflammatory drugs during the past three months; (e) injection by intra-articular hyaluronic acid and corticosteroids infiltration over the past six months. All patients signed a consent form by fulfilling the information sheets provided to each patient. Research Ethics Committee (No: RHPT 020005) in Physical Therapy and Health Rehabilitation department, College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Saudi Arabia granted ethical approval for this study. All procedures followed guidelines described by the (Declaration of Helsinki, 1964).
Study design
This was a randomized clinical trial following the CONSORT guidelines between October 2019 and March 2020 at the Outpatient Clinic and biomechanics lab in the College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Saudi Arabia. Quadriceps strength and CSA, and pain were evaluated before and after the treatment intervention by an independent assessor who was blinded to the treatment allocation.
Study plan and randomization
Patients were recruited and allocated randomly into two groups. Based on the randomized block design, a drawing sealed non-transparent envelope with a specific code for each envelope was chosen by all participants for either group (group A and group B) under the supervision of a blinded independent assessor. Patients in Group A received partial BFR (50% of total occlusion pressure) while patients in group B, partial BFR (70% of total occlusion pressure) was administered. Half of the patients in each group underwent one of the low-intensity resistance training (10% of 1RM or 30% of 1RM), and the second half trained with the other intensity. The treatment intervention continued for eight weeks.
Outcome measures
Outcome measures were cross-sectional area (CSA) in cm
Assessment procedures
Measurement of 1RM
Familiarization sessions were delivered to all patients one week before the 1RM testing session. A Quadriceps exercise chair (Indiamart
The patients were instructed to grip the side armrests firmly, placed on the bench correctly, and perform steady slow knee extension throughout its full range of movement. If the patient accomplished two repetitions successfully at the first attempt, the load was raised (2.5–5.0%) for the second attempt [20]. Nearly two to three min of rest were given between each attempt to gain recovery. If the patient failed to complete a single repetition, a second attempt was achieved by decreasing the load. This method was repeated until the load corresponding to a maximum repetition had been achieved.
Determination of the arterial occlusion pressure
To determine the total occlusion pressure, the patient laid down for 10 min. of rest to assist in promoting the hemodynamic stability. A digital blood pressure monitor model (Omron, M6 comfort, Vietnam) was used to measure the blood pressure (BP) and pulse rate (PR), taking into consideration an accuracy of (3) mmHg for BP and (5) % for PR [21, 22]. The therapist instructed the patient to lie supine position while resting comfortably. A vascular Doppler probe using brightness mode (B-mode) with high-frequency linear array transducer (10–15 MHz) was attached to Doppler ultrasound (HI vision Avius ultrasound unit; Hitachi; Japan). The probe was placed over the posterior tibial artery to measure its auscultatory pulse. For the determination of the total occlusion pressure, a narrow air (6 cm
Quadriceps CSA
During the scanning by the B-mode axial-plane Doppler ultrasound attached with a linear 5 MHz transducer, the patient was in a supine lying position with the leg extended and rested on the examination table. The scanning was done at the midpoint between the greater trochanter and lateral joint line of the knee and precisely aligned to the fascicle plane to visualize fascicles on the ultrasound screen obviously. The average of three scanned captures of quadriceps CSA was set. The scanning was executed by an expert sonographer who performed many trials of scanning before real capturing. The same sonographer scanned all patients throughout the study.
Pain score measurement
Knee pain was evaluated with a Visual Analog Scale (VAS) and self-filled by the patient. The patient placed a line perpendicular to the VAS line at the point that described the pain intensity [23].
Quadriceps muscle strength
For familiarization, the patient visited the laboratory at least once before undergoing testing. An isokinetic dynamometer (CSMI Humac 2009, Cybex II, II+, version 129, USA) was utilized to measure maximal voluntary isometric contraction (MVIC) with at 60
Treatment procedures
Resistance training program
Two days after assessing the patient’s 1RM, patients were included in the familiarization session. The patients performed the 45
Sample size calculation
The sample size calculation was determined based on estimated effect size (
Statistical analysis
All analyses were conducted using the SPSS version 23.0 (IBM, Chicago, IL, United States). Data are presented as mean
Results
Out of 56 potentially eligible participants, 40 patients met the inclusion criteria. They took part in the randomization phase, but only 35 patients completed the study, and their data were analyzed (18 patients in group A and 17 patients in group B). Flowchart of participants’ dropout and exclusion is depicted (Fig. 1).
There were no significant differences in the demographic characteristics and baseline scores of 35 analyzed patients. Group A and group B were homogenous regarding all anthropometric measures (i.e., age, weight, height, BMI and duration of illness (Table 1).
Patients’ baseline characteristics and scores
Patients’ baseline characteristics and scores
Data are presented as mean (SD); BMI body mass index, VAS visual analog scale.
Flow chart of patients’ participation.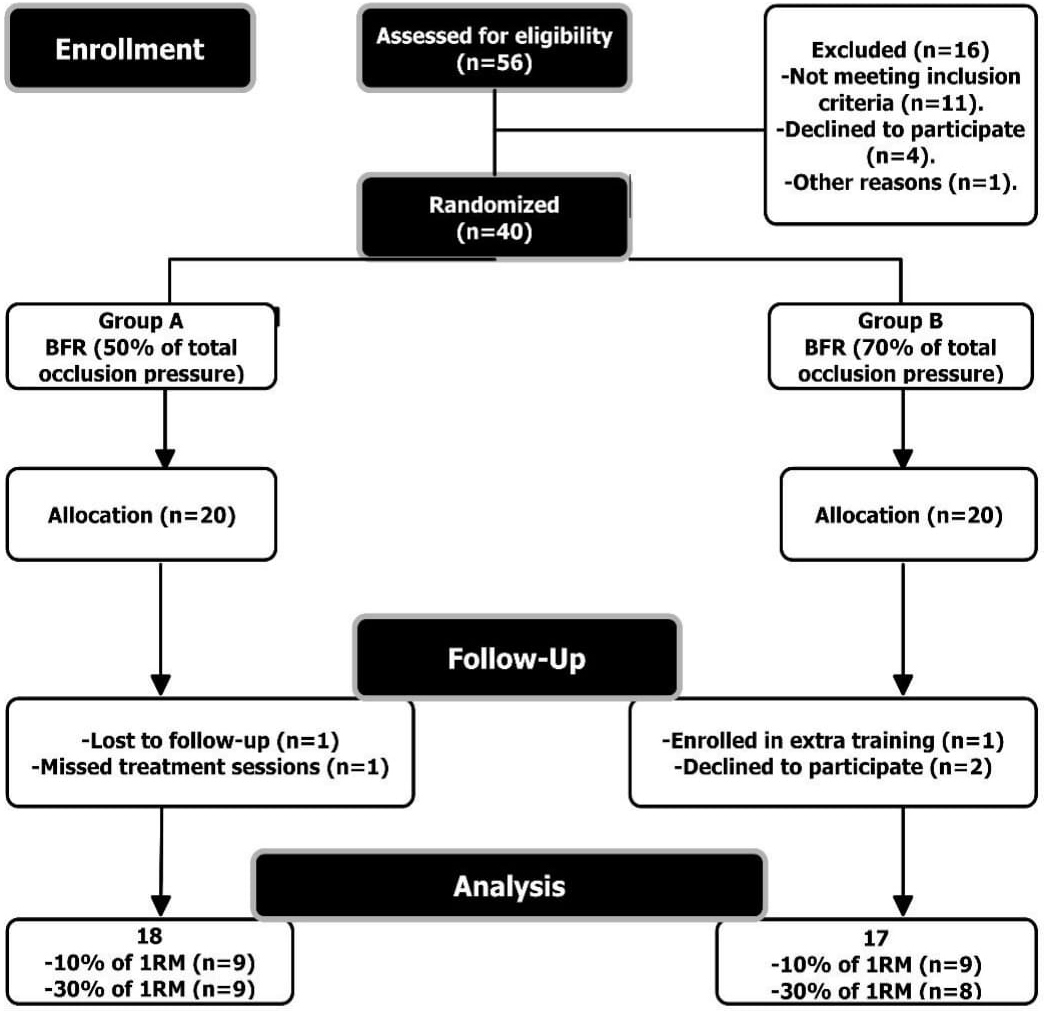
Although there was a small significant interaction effect of BFR and low-intensity resistance training on quadriceps CSA, F (1, 31)
The interaction effect between blood flow restriction and low-intensity resistance training on the cross-sectional area of the quadriceps muscle.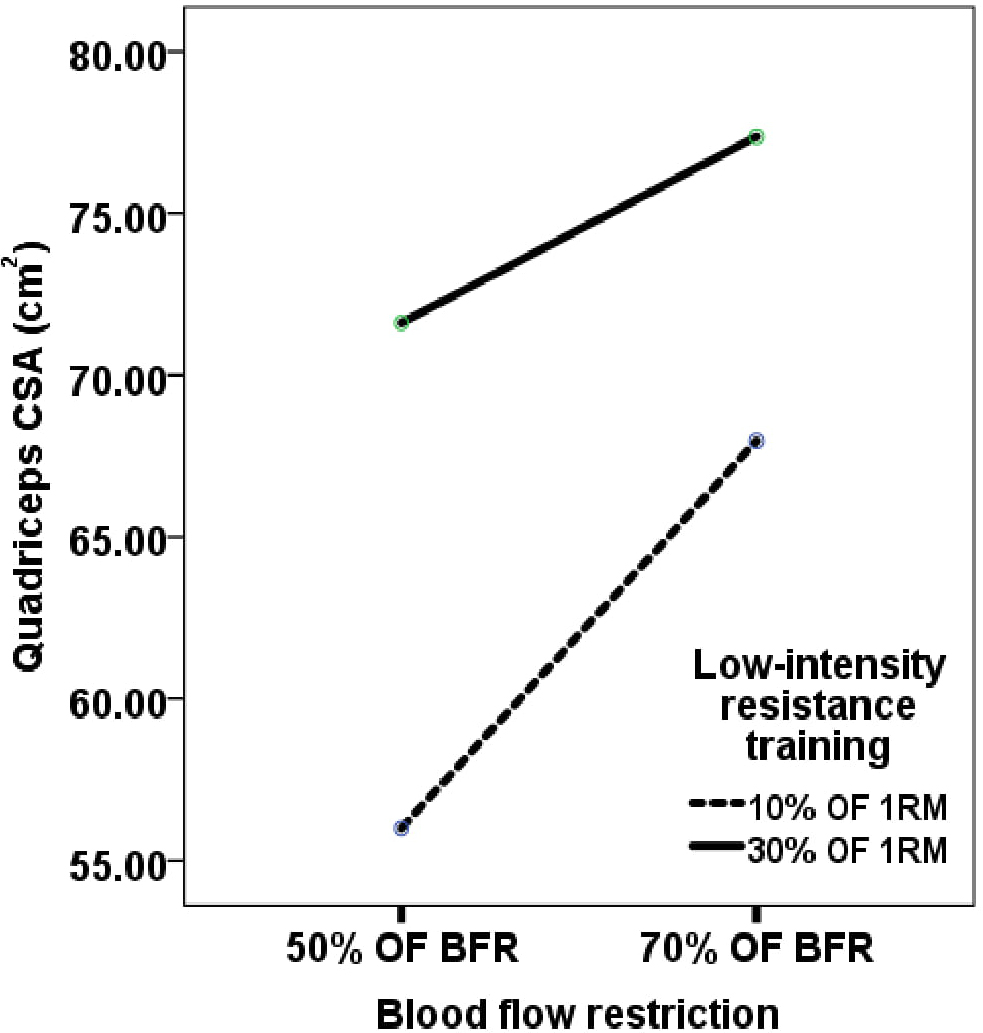
The strength of quadriceps improved using 70% of total occlusion pressure associated with 30% of 1RM more than 10% of 1RM, indicating a significant interaction effect as F (1, 31)
The interaction effect between blood flow restriction and low-intensity resistance on the quadriceps strength.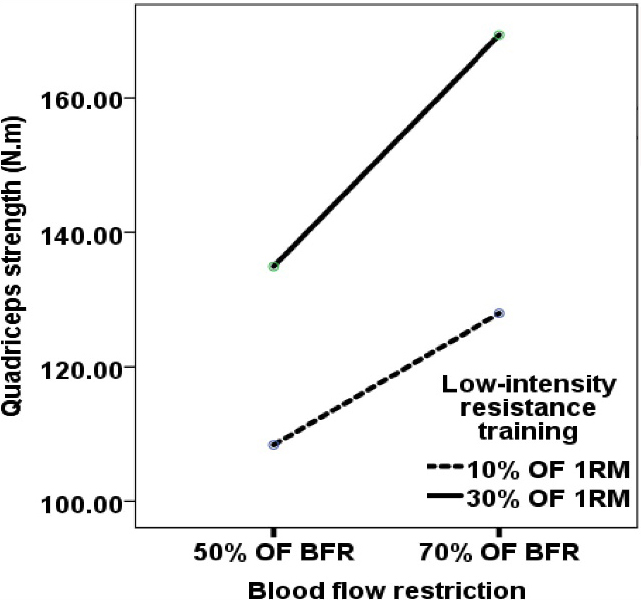
Pain changes of knee joint in response to the effect of blood flow restriction with low-intensity resistance training.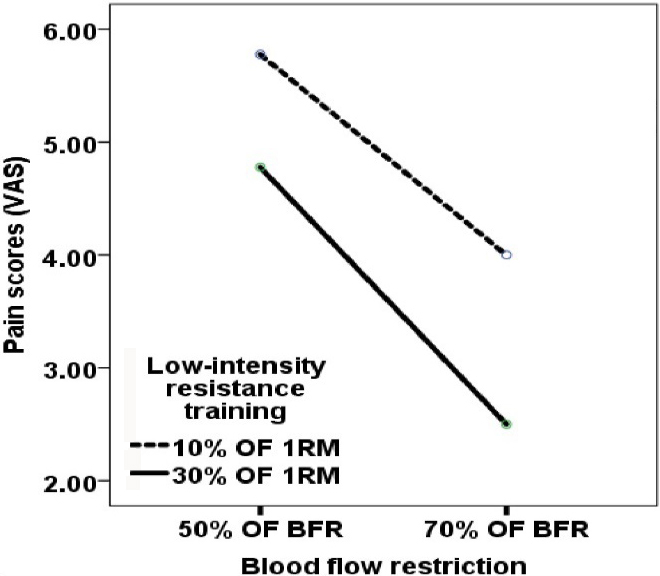
The main effect of partial BFR on knee pain revealed that the pain was reduced significantly through partial BFR, F (1, 31)
The knee pain and its relation with quadriceps CSA and strength
Knee joint pain was moderately and negatively correlated with both quadriceps CSA and quadriceps strength (
Discussion
The main finding of this study is that using a partial BFR (70% of arterial occlusion pressure) concurrent with the low-intensity resistance training of quadriceps muscle (30% of 1RM) yields an effective combination for increasing quadriceps CSA and strength and improving knee pain.
Rehabilitation specialists, dealing with older people are well aware of the phenomena of sarcopenia and dynapenia, the decrease in muscle mass and strength, respectively. With progressing age, skeletal muscle mass diminishes substantially at a rate of 3–8% per decade after the age of 30 [26], 1–2%/year older than 50 years [27], and 0.8–0.98%/year around the age of 75 [28]. As a result, thus, the mechanical stress on joints and bones is reduced mandating the application of resistance training in older people and which may be realized, by low-intensity resistance training associated with BFR [26].
In this context, a recent study compared different arterial occlusion pressures (40% Vs. 80%) concurrently with different low-load resistance training (10%–15%–20% 1RM) on surface Electromyography (sEMG), isometric moment and thickness of the elbow flexors. The authors declared that muscle growth could be achieved through higher blood flow restriction pressures, especially when low-load resistance training was used [29]. In the present study, it was noted that the greater the amount of BFR (70% of total occlusion pressure) associated with increased intensity of 1RM (30% of 1RM), the larger was the increase in the quadriceps CSA and its strength. This increase might be the result of the accumulation of inorganic phosphate by a significant amount inside the muscle leading to muscle fatigue, which induces recruitment of fast-twitch muscle fibers to reserve force generation resulting in muscle hypertrophy [30].
Another explanation for increasing the quadriceps CSA and its strength is increased circulation of growth hormone (GH), which stimulates the liver to produce Insulin-Like Growth Factor (IGF-1), consequently, enhances muscle protein synthesis [31]. Loenneke et al. [32] observed that 50% of estimated arterial pressure had a larger effect on muscle activation compared with 40%. Also, parallel to BFR, increasing low-intensity resistance training to 40% of 1RM produced greater recruitment of fast-twitch muscle fibers compared to 20% of 1RM [33]. A previous study supported the results of our study i.e., resistance training using BFR (80% of total occlusion pressure) with 30% of 1RM, conducted at two sessions/week for six weeks, enhanced the electrical activity of the quadriceps and therefore reflected on increased quadriceps moment and local endurance [34].
The probability of augmenting more motor units (MUs) in the patients of group B (BFR
Interestingly, previous studies stated that 50% of arterial occlusion pressure concurrent with resistance exercises could not enhance muscle activation and moment [35]. Loenneke et al. [36] concluded that in active young participants (18–35 years), low to moderate BFR (40–50% of arterial occlusion pressure) was enough to maximize the benefits of BFR, whereas 60% of arterial occlusion pressure did not yield any additional augmentation in knee extensors strength and activation. This finding is inconsistent with our study showing a positive effect of 70% of total occlusion pressure over 50%, in combination with either 10% or 30% of 1RM. We suggest that these conflicting findings were due to the expected sarcopenia and dynapenia among our elderly participants compared with the active young participants in Loenneke’s study. Elderly people might need to be trained with BFR
The relatively long treatment duration (8 weeks) in the current study, using low-load resistance training with partial BFR, had a significant effect on the outcome measures. Segal et al. found that four weeks of BFR augmented with low resistance training (30% of 1RM) did not reveal significant differences in thigh muscle power in men at risk or with KOA. They speculated that there was a need to complete longer durations of low-load resistance training with BFR to obtain higher strength gains than low-load training alone [7]. Another study confirmed that training at 20% to 30% of 1RM associated with BFR was sufficient to cause a significant increase in strength: to 33.4% in leg press and 26.1% in knee extension after 12 weeks of training [37].
Additionally, the number of sessions per week could have a definite effect on increasing the CSA and strength of the quadriceps. In the present study, three training sessions were conducted every week, probably accounting for the quite high percentage of improvement in the quadriceps CSA and its strength. The current study showed that the increase of CSA and strength of the quadriceps muscle were (31% and 38.47%), respectively, in patients (group A) who underwent low-intensity BFR (50% of arterial occlusion pressure). A previous study that used low-load resistance training (20–30% 1RM) with BFR (50% of arterial occlusion pressure) but two sessions per week, observed improvements in quadriceps CSA and its strength by 6% and 15.75%, respectively [20].
Decreasing the CSA of the quadriceps is considered a hallmark of the knee pain, especially in those with KOA. In our study, the results revealed that the smaller CSA of the quadriceps, the higher was the pain score (
In the present study, the strength and CSA of the quadriceps manifested a moderate correlation with knee pain. However, only strength could predict the level of pain in the knee and alteration in quadriceps strength could be a predictable risk factor for KOA. According to the results of our study, the average baseline of patients’ quadriceps strength was 90.73 N
In terms of limitations to the study, the choice of the male gender only could affect the generalizability of the study; however, we focused on men patients in order to avoid the discrepancy of muscle strength and muscle size between males and females and the possibility of faulty interpretation of results.
Conclusion
Based on the current results, partial blood flow restriction associated with low-intensity resistance training has a positive impact on muscle size and strength. A combination of 70% of total occlusion pressure with 30% 1RM could be beneficial in elderly PwKOA for improving pain, increasing the quadriceps strength, and its cross-sectional area. Furthermore, the changes in the strength of the quadriceps muscle could be a valid predictor for the pain level in these patients.
Author contributions
CONCEPTION: Waleed S. Mahmoud and Ahmed Osailan.
PERFORMANCE OF WORK: Ahmed S. Ahmed and Ragab K. Elnaggar.
DATA COLLECTION: Waleed S. Mahmoud, Ragab K. Elnaggar and Ahmed Osailan.
DATA ANALYSIS: Waleed S. Mahmoud and Ragab K. Elnaggar.
DATA INTERPRETATION: Ahmed S. Ahmed, Ragab K. Elnaggar and Nadia L. Radwan.
PREPARATION OF THE MANUSCRIPT: Waleed S. Mahmoud, Ahmed Osailan and Ahmed S. Ahmed.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Ragab K. Elnaggar and Nadia L. Radwan.
Ethical considerations
All patients signed a consent form by fulfilling the information sheets provided to each patient. Research Ethics Committee (No: RHPT 020005) in Physical Therapy and Health Rehabilitation department, College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Saudi Arabia granted ethical approval for this study. All procedures followed guidelines described by the (Declaration of Helsinki, 1964).
Funding
The authors are grateful to the Deanship of scientific research at Prince Sattam bin Abdulaziz University, Saudi Arabia, for financial support to carry out this work. Project No. 2019/03/10318.
Footnotes
Acknowledgments
The authors are grateful to the Deanship of scientific research at Prince Sattam bin Abdualziz University, Saudi Arabia, for accomplishing this work.
Conflict of interest
There is no conflict of interest to declare.