
Abstract
BACKGROUND:
Cervical stabilization exercises and local vibration may improve proprioception and balance and prevent musculoskeletal problems.
OBJECTIVE:
To compare the effects of local vibration and cervical stabilization exercises on balance, cervical joint position sense, and muscle performance in healthy participants.
METHODS:
Forty-eight healthy male participants without neck pain were included. The participants were randomly divided into three groups: a home exercise program lasting eight weeks to the cervical stabilization group; 60 s of vibration to the neck muscles of the local vibration group and a control group. Balance, joint position sense, and muscle performance were evaluated twice in all subjects, before and after the intervention.
RESULTS:
Joint position sense error values were decreased in both the local vibration and cervical stabilization groups. Balance was improved (
CONCLUSIONS:
The methods used in the present study may be used for improving the proprioceptive and vestibular components of balance in individuals with musculoskeletal problems such as cervical disc herniation, cervical spondylosis, or neck pain. However, given the limitations, much more research is needed to firmly establish these recommendations.
Introduction
Many musculoskeletal problems arise as a result of postural disorders caused by multifactorial reasons. The cervical region is one of the most common areas where these problems occur. Cervical region disorders are the second most common type in the musculoskeletal system in the general population after the lumbar region and affect about 70% of them [1]. Currently, with the increasing use of devices such as computer monitors and smartphones, healthy people may experience mild to severe neck pain as well as structural and functional problems in the cervical region [2]. Panjabi et al. [3] emphasized the importance of mechanical stability in the cervical region. They estimated that the muscular system in the cervical region contributes about 80% of the mechanical stability of the cervical spine, while the osseoligamentous system contributes the remaining 20%. In people with neck pain, the maximal isometric strength and endurance capacity decrease in the cervical region muscles [4, 5]. Also, jerky and irregular cervical movements and poor joint position sense have been found in people with chronic neck pain [6]. Also, neck muscles, in particular, the suboccipital and deep flexor muscles have a high density of muscle spindles which contribute to neck proprioception; one of the information sources that help adjust postural balance. Impairment of the afferent information from these muscles has been shown to affect postural sway [7]. Therefore, when examining the causes of musculoskeletal disorders in the neck, besides insufficient muscle performance and strength, decreased proprioception and impairment of balance systems (visual, vestibular, and somatosensory) should be considered as well [1, 8].
The cervical region is one of the most affected regions among the musculoskeletal system sections due to the dense proprioceptors it contains. Proprioception is defined as sensory information about the position of the body and limbs, the force of movement, muscle tension, and physical pressure from the Golgi tendon organ, muscle spindle, vestibular system, and joint receptors [9, 10]. Proprioception plays an important role in ensuring the coordination of movements. When the proprioception input is disturbed, both position perception and the speed of movement may be affected. An impaired sense of proprioception can cause problems in terms of position sense and balance [1]. Evidence has shown that there are many proprioceptors in the deep group of cervical muscles such as the multifidus, longus colli, and longus capitis [1, 8]. Deep group cervical muscles, which perform their functions like a dynamic ligament, have an important role in the stability of the vertebrae as well as proprioceptive sense. The longus colli and capitis are located in the anterior part and the semispinalis cervicis and multifidus in the posterior part of the deep group muscles. These muscles prevent spasms and excessive contractions of the superficial neck muscles. The deep muscles thus preserve cervical lordosis and at the same time resist gravity and contribute to the maintenance of the cervical posture [11, 12]. Proprioceptive receptors, which are intensely present in the deep suboccipital muscles, are associated with the vestibular, visual, and somatosensory systems [13]. In the event of atrophy and fat infiltration of these muscles, impairment of the somatosensory and vestibular parameters of balance may occur as a result of decreased proprioceptive sense [14, 15]. Considering these characteristics of deep neck muscles, increasing the effectiveness of these muscles can prevent neck problems by increasing segmental stabilization, balance, and proprioceptive senses in the neck region.
Although different methods are used in the development of balance and proprioceptive sense, exercise is an important one [16]. Recent studies in this area have focused on multimodal exercise therapies including strength, endurance, and coordination training; proprioceptive training; relaxation exercises; stabilization exercises; and behavioral modifications [17, 18]. In problems such as nonspecific neck pain, whiplash associated disorders, and cervical disc hernia, it is observed that different exercise programs are used, which generally include exercise elements targeting the neck muscles and called neck-specific exercises [19]. Neck-specific exercises usually include the activity of deep cervical flexors, isometric neck exercises, home exercises with exercise bands, various breathing exercises and neck strengthening during physical activity [20]. Neck-specific exercise programs for the ventral and dorsal neck muscles, consisting of both neuromuscular and neck muscle endurance exercises, have positive effects on pain, joint position sense, endurance and strength [21].
Cervical stabilization (CS) exercises, one of the neck-specific exercises, are a frequently used approach [22]. CS exercises, which are different from ordinary exercises, are based on biomechanics, neurophysiology, and physiotherapy research [23]. Typically, CS training regimes are designed to target the deep muscles, especially longus colli, capitis and the suboccipital muscles [24]. These muscles have many sensory receptors that are responsible for central and reflex connections to the visual, vestibular, and postural control systems [25]. Therefore, these muscles can be thought to be effective on balance and proprioceptive sense. Thus, the main objective of this method is to improve body awareness, strength, endurance, coordination, and proprioception and ensuring posture correction [26, 27]. CS exercises use the basic principles of motor learning. The primary goal in stabilization exercises is to develop spinal awareness. Spinal control is first developed in easy patterns and then progresses to complex patterns. From simple functional activities to complex and unplanned activities, the main goal of this process is to maintain spinal stability automatically. Also, CS exercises include kinesthetic training and functional training [28].
Vibration is another method that contributes to the development of muscle strength, balance, and proprioception. Among the causes of the effect of vibration on muscle strength, several mechanisms have been assumed, including tonic vibration reflex theory, increased muscle temperature and blood flow, increased motor neuron excitability, increased hormone secretion and muscle hypertrophy [29]. Tonic vibration reflex is a sustained contraction of a muscle subjected to vibration. This reflex is caused by vibratory activation of muscle spindles muscle receptors sensitive to stretch [30]. Muscle-tendon vibration is a non-invasive method used to improve proprioceptive sense in humans. Applying muscle-tendon vibration activates the Ia afferents of the muscle spindle and in some cases may improve the joint position sense (JPS) [31]. Microneurography studies have shown that the greatest role in the proprioception sense is related to muscle spindles. Local vibration (LV) is a powerful stimulus for the muscle spindles [31, 32]. When the anatomical characteristics of the cervical vertebra are examined, muscle spindles are found extensively in the deep extensor and deep flexor muscles [33]. It has been suggested that vibration applications increase muscle strength and proprioception sense [34]. Beinert et al. [35] showed that vibration increases afferent input from primary muscle spindle endings may cause the central nervous system to rely more strongly on other sensory inputs such as vestibular or cutaneous information. This input might be beneficial for neck pain patients as they may suppress unreliable afferent input from muscle spindles. However, may be detrimental for healthy subjects who can normally rely on this information in acute period vibration intervention. Similarly, Wannaprom et al. [36] showed that vibration may alter cervical proprioception and/or vestibular input in the healthy group resulting in an imbalance in sensory afferent input. They also suggest that healthy participants may need to adapt their gait speed in the direction of vibration-induced illusion to compensate for the postural instability created. However, they also recommend that long-term vibration treatments applied to the neck muscles determine whether they cause long-term benefit.
In light of this information, CS exercise and LV applied to neck muscles can improve muscle strength, proprioception, and balance and prevent musculoskeletal problems. However, few studies are investigating the effects of these two applications on balance, proprioception, or muscle performance [21, 37] and there is no study comparing these two applications for the cervical region [38, 39]. Thus, the present study aimed to investigate the effects of CS exercises and LV applied to the neck muscles on JPS, balance, and muscle performance. It was hypothesized that CS and LV would improve JPS, balance, and muscle performance in healthy individuals.
Methods
The study was conducted with 48 healthy male participants (mean age 21.7
Design and participants
The study was planned as an assessor-blinded, parallel-group, randomized controlled trial with repeated measures. After the initial assessment, the participants individually randomized to one of three parallel groups (1:1:1) using a random numbers table. There were 18 participants in the CS group, 17 in the LV group, and 17 in the control group (Fig. 1).
CONSORT 2010 flow diagram of participants.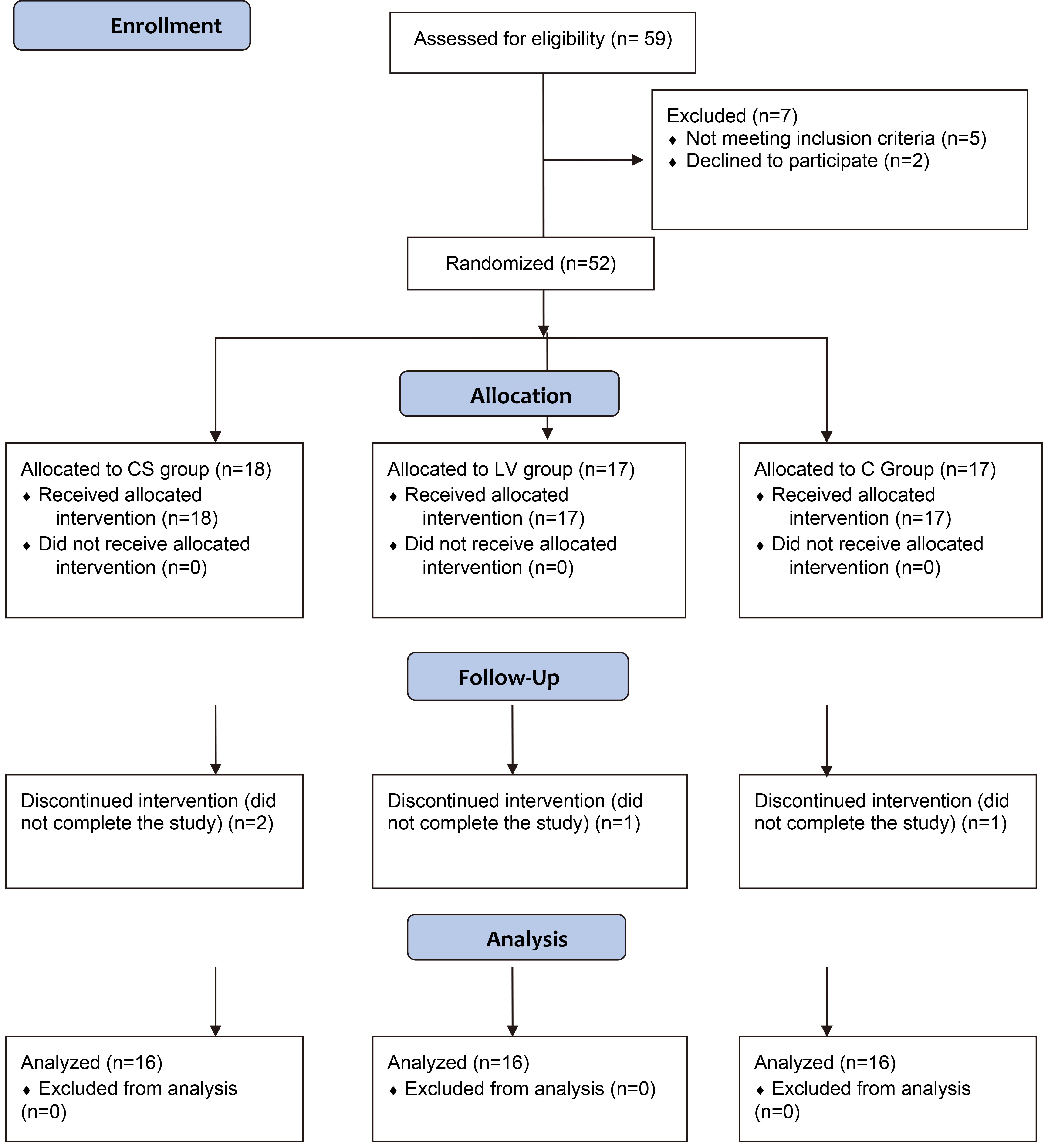
Healthy male subjects aged 18–30 years without neck pain in the previous six months were included in the study. Healthy participants were excluded if they had had any surgical treatment of the vertebral column or exercise therapy lasting at least three months or had an inflammatory or rheumatologic disease, history of malignancy, radiculopathy, myelopathy or other neurological disorders, or had a congenital orthopedic anomaly or had a vestibular, extremities and vertebral trauma history. According to the results of a pilot study and the balance scores from the Composite Balance Score (CBS) [40], a sample size of 16 in each group would provide a statistical power of 90% at a 0.05 level of probability.
Outcome measures were assessed before the first intervention session (baseline data) and immediately after the eight-week intervention period by the researcher. Clinical and demographic information including age, height, weight, and body mass index was recorded.
Balance (Computerized Dynamic Posturography)
The sensory organization test (SOT) is used to assess balance. In the present study, the SOT was performed with NeuroCom Smart EquiTest Computerized Dynamic Posturography. The SOT was developed to define the contribution levels of the three basic systems of balance (visual, vestibular, and somatosensory) to overall balance [41]. The SOT includes six test conditions, from easy to difficult. In the first three conditions, the platform of the device is fixed. In the first condition (SOT1), visual, somatosensory, and vestibular information is measured together.
Assessments: A. Balance assessment: Sensory organization test using with Computerized Dynamic Posturography B. Joint position sense assessment: Joint position sense error test using with Cervical Range of Motion Device C. Initial position of strength and endurance assessment.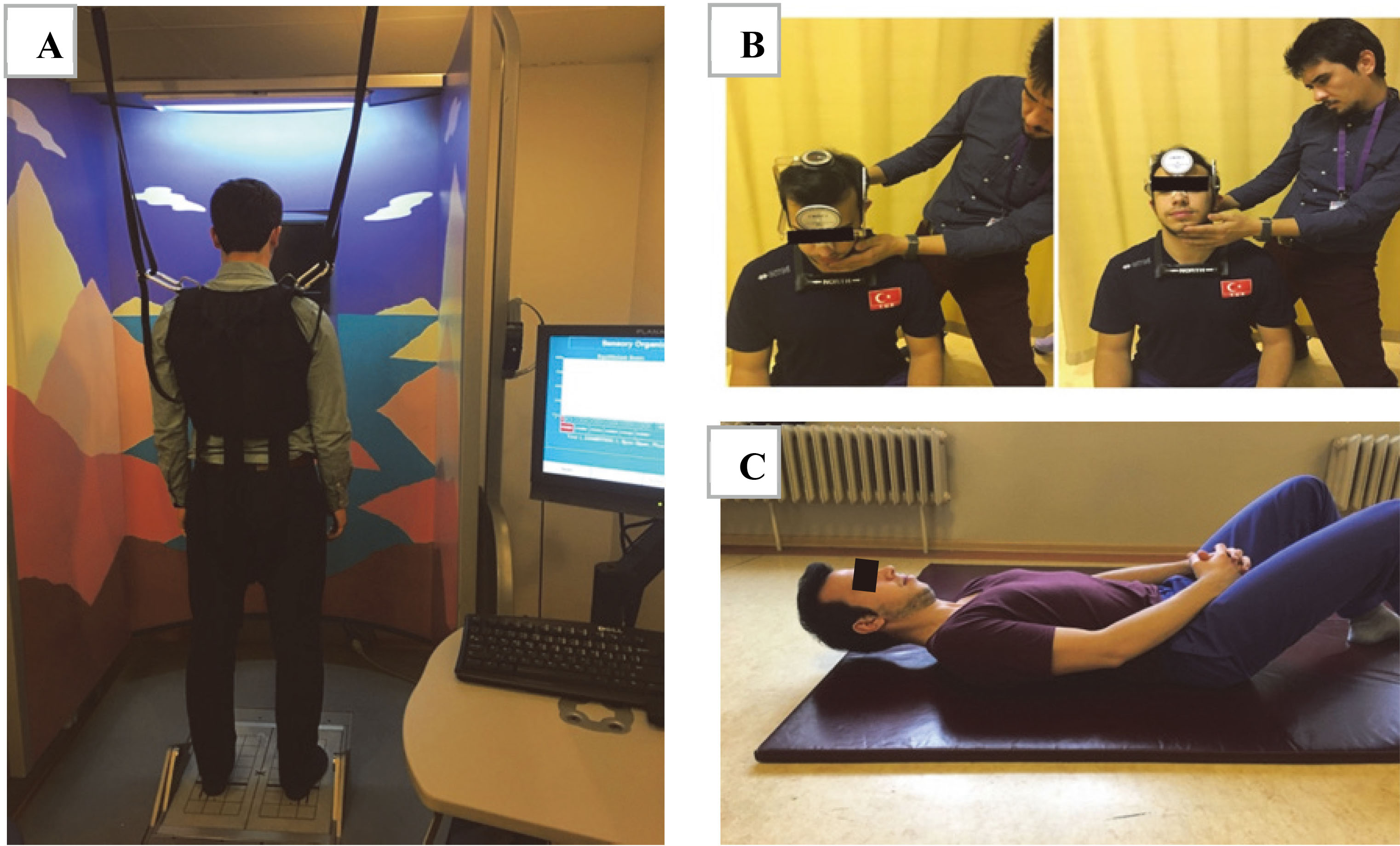
In the second condition (SOT2) the participant’s eyes are closed, while in the third condition (SOT3) the participant is given incorrect visual information and thus the level of the participants’ use of somatosensory information is tested. In the last three conditions, the platform of the device is mobile. In the fourth condition (SOT4), the participant’s eyes are open as the platform moves and thus the level of visual knowledge is tested. In the fifth condition (SOT5), as the platform moves, the participant’s eyes are also closed and thus the vestibular inputs are tested. Finally, in the sixth condition (SOT6), the participant’s ability to use vestibular information is tested by giving him or her a false visual stimulus while the platform is mobile [41]. In general, the SOT measures how well the participants can maintain their center of gravity when their visual, vestibular, and proprioceptive inputs are disrupted [42].
The participants began testing with their feet at shoulder width and the medial malleolus aligned with the axis of rotation of the platform. The researcher secured the participants using seat belts to prevent falls (Fig. 2). The participants performed three different trials in the six conditions, each lasting 20-s. The researcher noted the average of the three trials performed by the participants [43]. The participants scored between 0 and 100 for the 6 different conditions after the SOT. Full points from the SOT meant perfect balance. The researcher rated the scores of the participants in the 6 different conditions and the combined balance score, which shows the overall balance level of the participants, was calculated [41, 43].
Cervical Range of Motion 3 (CROM 3) was used to measure the participants’ JPS error. The cervical JPS error was evaluated in six different situations, namely flexion, extension, right lateral flexion, left lateral flexion, right rotation, and left rotation. As the researcher started the test, he told the participants to sit upright in a comfortable position with their arms at their sides and to look ahead. The researcher positioned the participant’s head slowly and passively to 65% of the maximum range of motion (Fig. 2). The aim of moving the head slowly was to reduce the effect of vestibular functions, which could change with age. The researcher held the participant at the point where he was positioned for three seconds and told him to feel his position. He then moved the participant’s head back to the neutral position. The researcher asked the participants to come actively and unaided this time to the maximum of 65% determined in the previous step. Then the degree of error between the point where the participant was active and the reference value previously set as passive was recorded. The measurement was repeated three times and the mean value of errors recorded [44, 45, 46].
Strength and endurance of cervical muscles
The researchers used a digital hand dynamometer to measure the strength of the cervical flexor and extensor muscles (Lafayette Instrument Company, USA). When measuring with a dynamometer, the position and methods were based on Lovett’s muscle test positions and method [47]. Resistance was applied from the frontal region for the cervical flexor muscles and the occipital region for the cervical extensor muscles. Each muscle test with the dynamometer was repeated three times. Between the repetitions, a one-minute break was taken for the participants to rest. The researchers noted that the highest results obtained in the measurements were used for statistical analysis. After each use, the device was returned to its previous settings and all values on the LCD screen were reset [48, 49].
Exercise intervention: A. Example of first level exercises B. Example of second level exercises C. Example of third level exercises.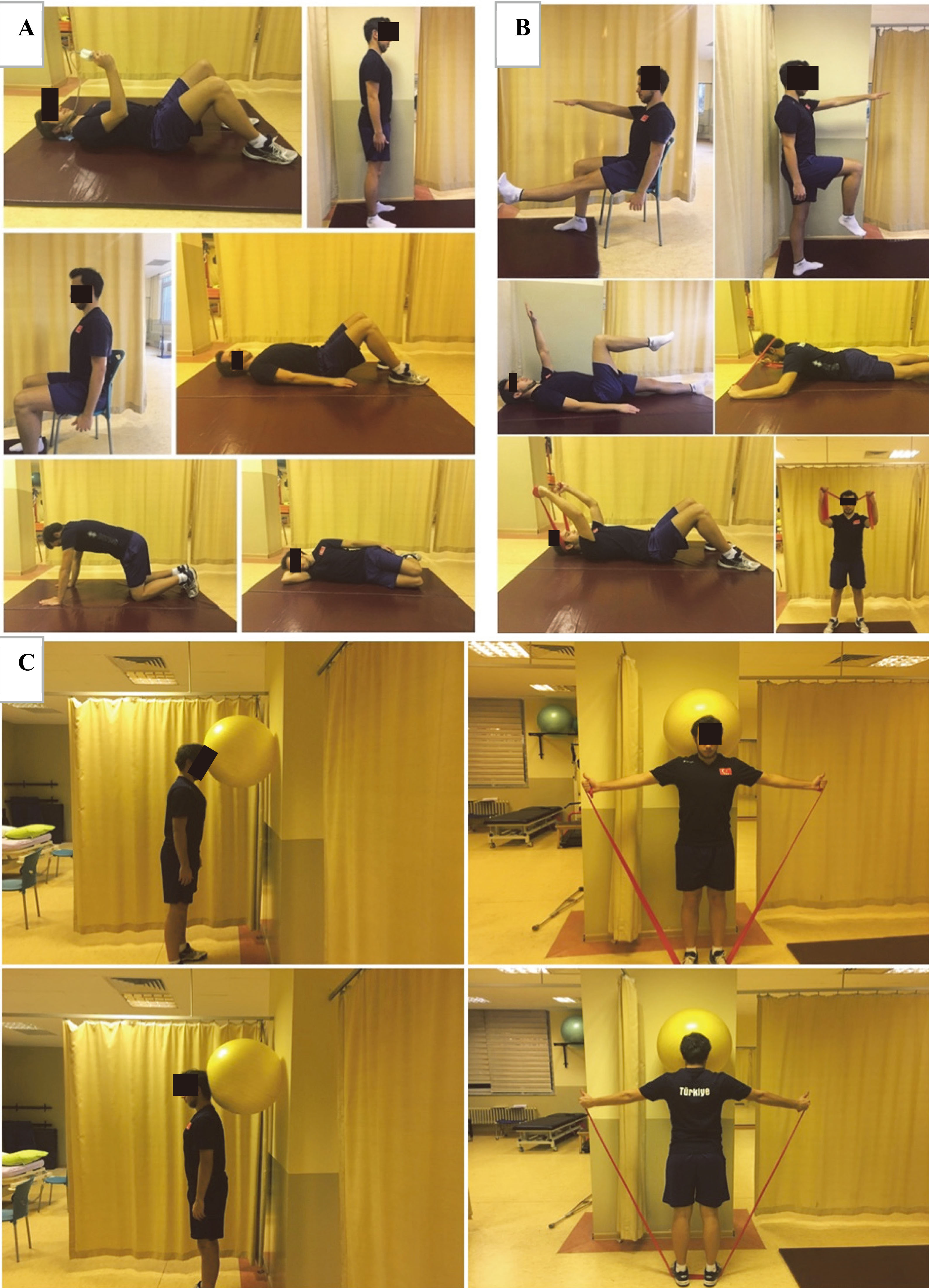
Measurement of the endurance of the deep cervical flexor muscles started with the participant in the supine position with his hands-free on his abdomen. The participant, with orders from the researcher, raised his head only a few centimeters off the ground. The researcher asked the participant to perform mild craniocervical flexion and to maintain this position. The pressure biofeedback device (Stabilizer
Cervical stabilization group
Participants included in the CS group performed CS exercises, which consisted of three levels and gradually increased in difficulty, as a home exercise program. Three phases of this specific rehabilitation can be viewed as a continuum for prescribing exercises [51].
The home exercise programs of participants were rearranged according to their weekly check-ups. The weekly check-ups were performed to understand how accurately the participants did the exercises and to determine their current levels for exercise progression. They were also asked to record their schedule for the days when they performed the exercises. Thus, the researchers gave and organized the CS group exercise programs weekly. The CS group performed the exercise program every day of the week, one session per day, and all the exercises were repeated 10 times. Participants were informed that they could contact the researcher (NK) who has approximately 30 years of experience in neurosurgical rehabilitation if they any discomfort while doing home exercises. The content of the training program is briefly explained below:
The researchers asked the participants to ensure craniocervical flexion and posture alignment before each exercise. First Level (Week 1–Week 3): The CS group was first informed about the biomechanics of the neutral spine and the correct position. The main aim of the first level exercises was to learn craniocervical flexion and to continue this exercise in all neurodevelopmental stages. The researcher showed the exercises to the CS group using slow movements to achieve motor control, to create kinesthetic awareness, and to increase endurance. Second Level (Week 4–Week 6): The second level exercises aimed to increase motor control using faster movements and to integrate craniocervical flexion and lower and upper extremity movements. It was aimed to control the movement at the conscious level. Then the resistance of the movements was increased with the help of elastic resistance bands. Third Level (Week 7–Week 8): In the third level exercises, elastic resistance bands and resistant, unpredictable exercise methods were used and subconscious control of movement was aimed. In this level of exercise, the participant tried to achieve dynamic balance by using an elastic resistance band and controlling a ball placed between the wall and his head. Functional exercises at this level increased the degree of load on the individual’s deep cervical muscles. The aim of the loading in the deep group muscles was to increase the subconscious control of movement (Fig. 3).
Local vibration group
In the LV group, LV was applied to the neck muscles of the participants 3 days a week for a total of 8 weeks. The application was performed with a portable LV device (Vibrasens; Techno Concept, France). The vibration was applied to the suboccipital region of the neck with the 7-centimeter probe of the device for 60 seconds for both sides in 80 Hz (Fig. 4).
Local vibration intervention on neck muscles.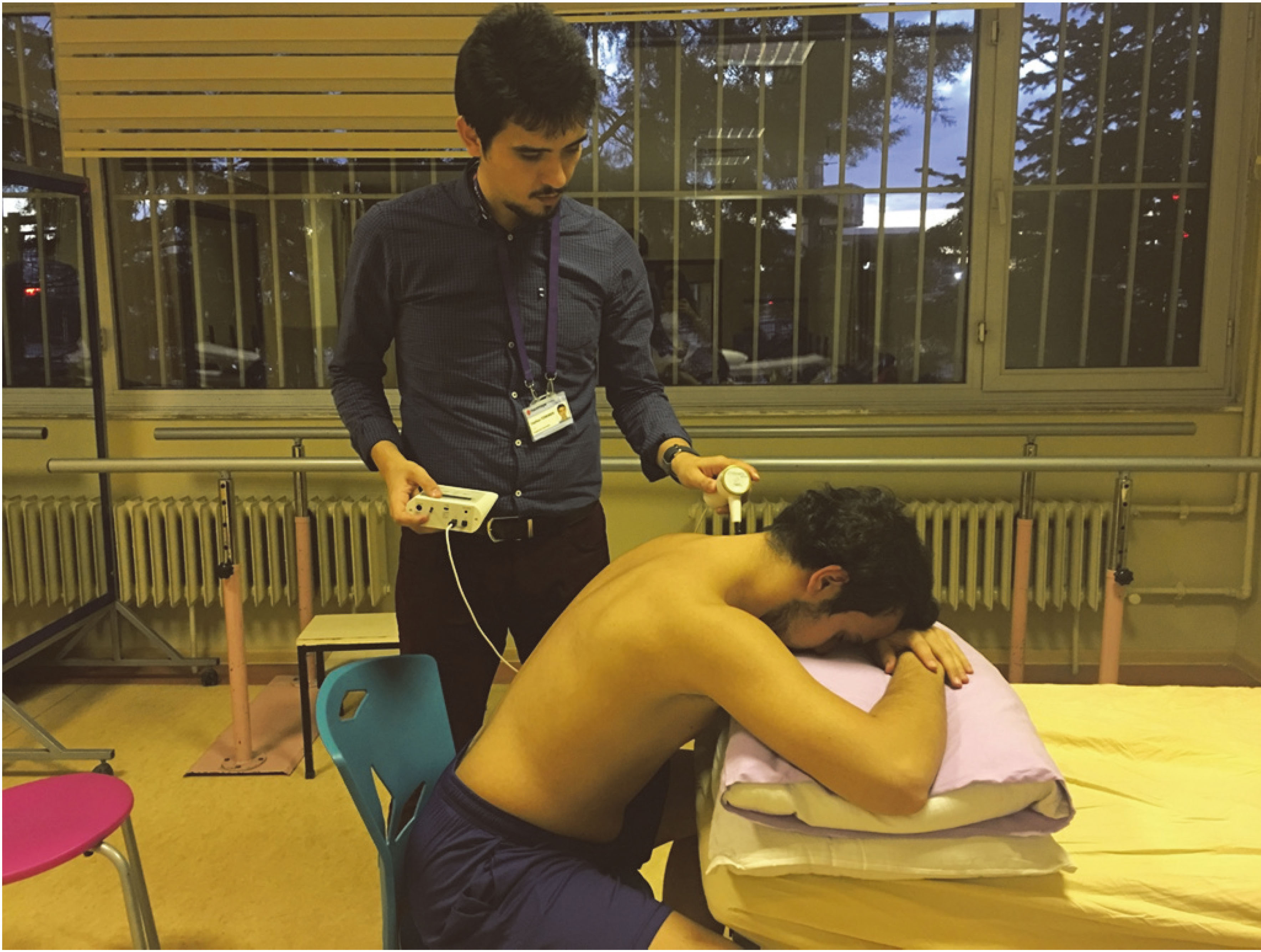
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 20 (IBM SPSS Statistics; IBM Corporation, Armonk, NY, USA). The one-sample Shapiro-Wilk test was used to evaluate the distribution of variables before test selection. Descriptive statistics were presented as medians for the non-normally distributed quantitative variables. Differences in continuous variables (age, height, weight, and BMI) among groups were analyzed by Kruskal-Wallis test. Comparisons of changes between the groups were also analyzed by Kruskal-Wallis test. The Mann-Whitney U test was performed to test the significance of pairwise differences using Bonferroni correction when overall significance was observed in the quantitative data.
Results
A total of 52 male participants were included in the study, 18 in the CS group, 17 in the CS group and 17 in the control group. In the CS group, two participants and in the LV group, one participant failed to give a reason for not participating in the study; and one participant in the control group left the study in the last measurement of the study because of difficulty with transportation (Fig. 1).
At the beginning of the study, the demographic (age, height, weight, and BMI) and clinical characteristics (SOT, JPS error, muscle strength, and muscle endurance) of the participants were similar in the three groups (
Baseline characteristics of the cervical stabilization, local vibration, and control groups
Baseline characteristics of the cervical stabilization, local vibration, and control groups
Comparison of changes in the sensory organization test between the local vibration, cervical stabilization, and control groups
The descriptive characteristics (age, height, weight, and body mass index) of the participants were examined and no difference was found between the groups (
Changes in balance (Computerized Dynamic Posturography)
The differences between the values of the participants before and after 8 weeks of intervention were compared between the groups. There were differences between the groups only in the SOT1 condition. When post-hoc analyses were performed for SOT1 status, it was found that the LV group had a greater improvement in this balance status compared to the CS and control groups (Table 2).
Changes in cervical joint position sense error
When the differences in JPS error scores before and after were examined in the groups, significant differences were seen in the flexion, extension, and left lateral flexion aspects.
Post-hoc analysis of the JPS error scores showed that the flexion score decreased more in the LV group compared to the control group, while both the LV and CS groups showed greater decreases in extension score compared to the control group. Similarly, the left lateral flexion score was significantly lower in both the LV and CS groups than in the control group (Table 3).
Comparison of changes in joint position sense error between the local vibration, cervical stabilization, and control groups
Comparison of changes in joint position sense error between the local vibration, cervical stabilization, and control groups
Comparison of changes in muscle strength and endurance between the local vibration, cervical stabilization, and control groups
When the differences between the groups were examined before and after, the cervical flexor muscle strength increased more in the CS group than in the LV and control groups. For muscle strength of the cervical extensors, the strength increase in the CS group was higher than that in the control group only. Similarly, the ventral endurance of the cervical region increased more in the CS group than in the control group (Table 4).
Discussion
In the present study, the effects of CS exercises and LV applied to the neck muscles on balance, muscle performance, and JPS error were investigated. The results showed that JPS error values decreased in both the LV and CS groups. Balance analysis showed improvement only in the LV group, whereas improvement in muscle performance parameters was only seen in the CS group.
Balance (Computerized Dynamic Posturography)
SOT1 is a condition in which the visual, vestibular, and mainly somatosensory information is used [52]. The increase in the SOT1 condition after 8 weeks of LV applied to the neck muscles may indicate that balance in the LV group is positively affected. The reason for this development can be explained by the rearrangement of sensory inputs in that region after LV applied to the neck muscles [53], because LV at 80–120 Hz is a good stimulus for the afferent fibrils of group Ia originating from muscle spindles [54]. Similarly, LV was applied to the neck muscles at 80 Hz in our study.
In the neck region, when multisensory inputs are damaged due to different reasons, individuals rely more on vestibular inputs while reducing their confidence in proprioceptive inputs [55]. LV applied to the neck muscles increases the integration of vestibular and proprioceptive information by providing somatosensory inputs and may positively affect the individual’s balance. Bruyere et al. showed that 6 weeks of vibration training applied to healthy women improved their balance according to their Tinnetti balance score and Time Up and Go (TUG) test scores [56]. Similarly, Cheng et al. found that whole-body vibration training applied to healthy men reduced postural oscillations and improved balance [57].
On the other hand, some studies have indicated a negative effect of local vibration applied to healthy individuals. Wannaprom et al. showed that standing balance was impaired immediately after vibration in healthy participants [36]. Similarly, Beinert et al. also observed a decrease in balance ability in healthy people immediately after applying vibration to the neck muscles [31]. Both studies have argue that vibration could alter cervical proprioception and/or vestibular access, thus causing an imbalance in sensory afferent access and excessive sensory noise in the sensorimotor system. However, these studies performed balance assessments only immediately after intervention and indicated that long-term effects should be assessed. During the balance assessment after vibration applied for 8 weeks, no similar results were observed in acute period balance impairment.
Joint position sense
It is well known that the deep cervical flexor and extensor muscles contribute to posture by providing head and neck stabilization [21, 58]. Individuals cannot maintain postural alignment in the event of weakening or imbalance of muscles in the anterior and posterior regions of the neck [59]. In these muscles, if the atrophy or imbalance process is prolonged, the sensitivity of muscle spindles decreases and proprioceptive sense loss occurs [60, 61]. Sanchez et al. showed that proprioceptive sense was reduced due to a lesser muscle mass, incomplete muscle activation and decreased muscle spindle sensitivity. These variations may have a negative effect on postural stability [62]. Muscle length changes slightly during vibration. Receptors in skin and joint can theoretically contribute to these sensations. However, results in muscle-tendon vibration and microneurography studies have demonstrated a major role of muscle spindles in proprioception [54]. Brumagne et al. demonstrated that multifidus muscle spindle input is critically important for vertebral position sense during sitting. In addition, joint receptors were mainly active at extreme joint angles, whereas muscle spindles fired throughout the full range of motion [32].
After vibration is applied to the muscles, activation of muscle spindles and polysynaptic pathways takes place [63]. In our study, the increase in the proprioceptive sense with decreasing JPS error values in the LV group can be explained by these effects of muscle spindles activation. We could find no studies that explored the effects of long-term LV applied to the neck muscles on proprioceptive senses. However, Piecha et al. [64] examined the effectiveness of whole-body vibration applied to healthy individuals for 4 weeks and found that postural stability improved in healthy individuals after training. They suggest that the improved proprioception and postural stability in patients might be due to improved synchronization of the firing of motor units, improved co-contraction of synergist muscles and increased muscle strength after vibration training. Similar effects were observed after eight weeks of local vibration application. While the JPS error values of the CS group decreased compared to those of the control group, these decreases were lower than those of the LV group. In contrast to our current results, previous studies indicated that CS exercises significantly improved JPS [45]. The reason for the less developed JPS in the CS group in the present study may be due to the fact that CS exercises were performed as home exercises without a supervisor (physiotherapist). Similarly, Hidalgo-Perez et al. suggested that CS exercises in asymptomatic individuals could not improve JPS sufficiently and that this result was caused by individuals doing the exercises as a home program [65]. When CS exercises are performed in the presence of a supervisor, motor learning and sensorimotor integration may improve more in individuals than when the exercises are performed at home.
Strength and endurance of cervical muscles
In the present study, LV application did not affect muscle performance in the neck region. Drummond et al. found that 5-minute LV applied to the elbow flexors together with the traditional strengthening method improved muscle strength after 12 weeks, but was not more effective than the conventional strengthening method [66]. Drummond considered that the increase in muscle strength was due to the activation of muscle spindle primary endings, as well as the effect of tonic vibration reflex on gamma motor neuron control. Xu et al. thought that strengthening exercises and LV applied to the biceps muscle for eight weeks increased the maximum voluntary force and this result was due to the increase in primary motor cortex activation with tonic vibration reflex [67]. In our study, CS exercises resulted in a significant increase in flexor and extensor muscle strength. França et al. thought that CS exercises combined with acupuncture increased cervical muscle strength in patients with neck spasm and this was caused by increased cortex stimulation as a result of motor learning [68]. Similarly, Suvarnnato et al. showed that semispinalis cervicis training, which is applied within the scope of CS exercises, provides a significant increase in neck-extensor muscle strength [69]. One possible mechanism to describe the effect of exercise in muscle strength is that muscle contraction from the exercise training stimulated mechanoreceptors, including the muscle spindle, Golgi tendon organ, and proprioceptors of joints. This observed increase in cervical muscle performance could be attributed to a change in the excitability of the motoneuronal pool or modification of the neural activation patterns for cervical movements [70]. However, in our study, LV intervention did not improve muscle performance possibly because it was not used together with any strengthening program. Another reason for this result is that the vibration applied to the neck muscles was shorter than that applied to other muscles [31, 71, 72].
Consequently, it was concluded that CS exercise was a better method to increase cervical muscle strength.
Study limitations
There are certain limitations of the present study. The first and most important limitation is that individuals can learn the working principles of the Computerized Dynamic Posturography device. The learning effect that occurs in individuals can be confused with the improvements in the balance as a result of interventions.
Second, the effectiveness of the interventions was measured only immediately after the intervention program. There is a need to investigate the long-term impact of these interventions. The LV group was followed up by the supervisor, while the CS group performed a home program. These differences between the intervention groups can be considered another limitation. Also, there were differences in frequency and duration between both interventions in our study. While LV intervention was performed three days a week and 2 minutes, CS training was performed every day of the week and the mean intervention time was 40 minutes. These different intervention times could be the last limitation of this study. The main reason for these differences was that the optimum frequency and duration varied according to the type of intervention. Perri et al. [73] showed that high frequency and duration (5–7 days per week, at least 30 minutes per day) of exercise increases the benefits of exercise without a deleterious effect. Di Giminiani et al. [74] also, showed that the vibration intervention can be designed as three days a week for eight weeks. On the other hand, in studies investigating the effects of one-session neck muscle vibration on proprioception and strength, it has been observed that the duration of the intervention usually does not exceed five minutes [75, 76].
Conclusion
According to our results, CS exercises and LV may have positive effects on balance, cervical JPS, or muscle performance in healthy individuals. The methods used in the present study may be considered appropriate to improve the proprioceptive and vestibular components of balance in individuals with musculoskeletal problems such as cervical disc herniation, cervical spondylosis, or neck pain.
Author contributions
CONCEPTION: Ceyhun Türkmen, Nezire Köse, Sevil Bilgin and Songül Aksoy.
PERFORMANCE OF WORK: Ceyhun Türkmen, Büşra Altın, Hatice Çetin and Esra Dülger.
INTERPRETATION OR ANALYSIS OF DATA: Ceyhun Türkmen, Nezire Köse, Songül Aksoy and Büşra Altın.
PREPARATION OF THE MANUSCRIPT: Ceyhun Türkmen, Nezire Köse and Sevil Bilgin.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Ceyhun Türkmen, Nezire Köse, Sevil Bilgin, Hatice Çetin, Esra Dülger, Büşra Altın and Songül Aksoy.
SUPERVISION: Nezire Köse, Songül Aksoy and Sevil Bilgin.
Ethical considerations
The selection and recruitment were conducted by the Declaration of Helsinki and all subjects signed a written informed consent form before their inclusion in the study. The study received ethics approval from Hacettepe University Non-interventional Clinical Research Ethics Boards (approval no: GO15/716-04, date: 02.12.2015), Clinical HYPERLINK “http://Trials.gov” Trials.gov ID: NCT03464214).
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors acknowledge the collaboration of participants and associations involved in this study.
Conflict of interest
No potential conflict of interest was reported by the authors. The authors, their immediate family, and any research foundation with which they are affiliated have received no financial payments or other benefits from any commercial entity related to the subject of this article.