
Abstract
BACKGROUND:
In recent years, power assist suits have been used in nursing and rehabilitation scenarios. The external assistive force might disturb the user’s motor control system during the process of assisted training using power assist suit, thus affect the progress of rehabilitation. With the consideration of the non-negligible physiological differences between upper limbs, this study focused on the physiological responses of the two arms against the external assistive force.
OBJECTIVE:
To investigate and contrast the impact of assistive force on dominant and non-dominant arms during unilateral isometric elbow flexion.
METHODS:
Participants were instructed to adjust force exertion to a target value based on the visual feedback. Task performances including muscle activity of agonist and antagonist muscles, force steadiness and rated perceived exertion were evaluated at multiple workload and assistive load conditions.
RESULTS:
No significant differences in muscle activity of agonist and antagonist muscles between the two arms. In contrast, the dominant arm showed a higher assist efficiency at a low assistive level, whereas the non-dominant arm had a lower level of force fluctuation during a unilateral force matching task.
CONCLUSIONS:
Both arms could utilize the assistive force to reduce muscle activity. However, the two arms showed different abilities in response to external assistive force. This indicates distinct motor control strategies for each arm and implicates the necessity of side-individualized rehabilitative approach for achieving a better training effect.
Background
The power assist suit (PAS), a wearable machine that augments human physical capabilities, has been applied in nursing and rehabilitation scenarios [1]. As a complementary tool to therapist, PAS can be integrated to drive the impaired limb in rehabilitation training [2] or be used as an assistive device in daily life [3]. This kind of motion assistive device will be more widely acceptable in the near future. Recently, research on PAS has focused not only on mechanical development but also on its clinical efficacy. Studies that compared the long-term effects of robotic therapies with conventional occupational therapy indicated similar levels of improvement in motor control capabilities of the two training methods [4], thus confirming the effectiveness and applicability of PAS-based training. Nevertheless, most of these studies mainly focused on the training effect at the final stage, and research on human-PAS interactions during operating progress is still insufficient.
Humans are capable of modulating physical output based on the feedback of the muscle tension and their own experiences. However, when an external assistive force is applied, the physical output could be different from what was expected. This gap might disturb the motor control system [5], influence the training effect and prolong the training progress. Accordingly, such human physiological interactions with robotic assistance devices must be considerate during the development of PAS.
This research focuses on the PAS for the upper limbs, since high functioning upper limbs are crucial for quality of life. When performing daily behaviors, humans preferentially use one arm over the other for tasks such as opening a drawer or using a broom. Daily preferential use was shown to alter physiological and mechanical properties of skeletal muscle. It has been reported that during submaximal isometric flexion of the first dorsal interosseous muscle, motor units in the dominant hand show lower average firing rates and recruitment thresholds compared to the non-dominant hand, which suggest higher mechanical effectiveness of motor units in the dominant hand [6]. Additionally, the dominant limb shows stronger isometric muscular strength and better skill performance and learning rate due to preferred use over time [7, 8]. Moreover, from the perspective of the motor control mechanism, movements of the dominant hand are controlled mainly by the brain hemisphere contralateral to that hand, whereas the non-dominant hand is controlled by both hemispheres [9, 10]. Because of interhemispheric transmission delays, the non-dominant arm has disadvantage in performance, such as movement speed and accuracy, compared to the dominant arm [11].
However, some studies indicated that dominant and non-dominant arms have different specialties during unilateral movements due to their different control strategies. Functional magnetic resonance imaging (fMRI) showed that the right arm is controlled by the left motor cortex, which specializes in dynamic control and predictable situations, while the left arm is controlled by the right motor cortex, which specializes in impedance control and unpredictable situations [9, 12]. Correspondingly, studies comparing the performance of the two arms during target reaching movements found lower average muscle activity in the dominant arm, which suggests that the dominant arm more effectively anticipates task dynamics; the non-dominant arm more accurately compensated for an unexpected load, indicating that the non-dominant arm specializes in the control of the steady-state position [13, 14].
It is still difficult to determine whether the dominant arm is superior, or if the two arms have advantage in specific aspects of control, since the underlying neural mechanisms of handedness remain incompletely understood. Notwithstanding this lack of data, task capability and motor control strategies of the two arms are distinct to some degree, which might cause a difference in physiological responses to external assistive force between the two arms. On the other hand, isometric exercise, which movements are simple and applicable to all age groups, has been proved to be effective to improve ability in muscular-neuron disease sufferers [15, 16]. Therefore, the first objective was to investigate the physiological adaptability during unilateral isometric elbow flexion of each dominant and non-dominant arm against assistive force. The second objective was to evaluate bilateral arm performance through analysis of electromyography of agonist and antagonist muscles and force exertion steadiness. The comparison between the dominant and non-dominant arms may give insight into the training strategy of PAS-assisted rehabilitation.
Materials and methods
Experimental participants
Thirteen healthy male university students were recruited (Table 1). Handedness of each participant was assessed using the Edinburgh Handedness Inventory [17]. All participants gave written informed consent and the experiment was approved by the Ethics Committee of the Faculty of Design, Kyushu University, Japan.
Characteristics of participants (
13)
Characteristics of participants (
Experimental set-up for unilateral isometric elbow flexion with assistance.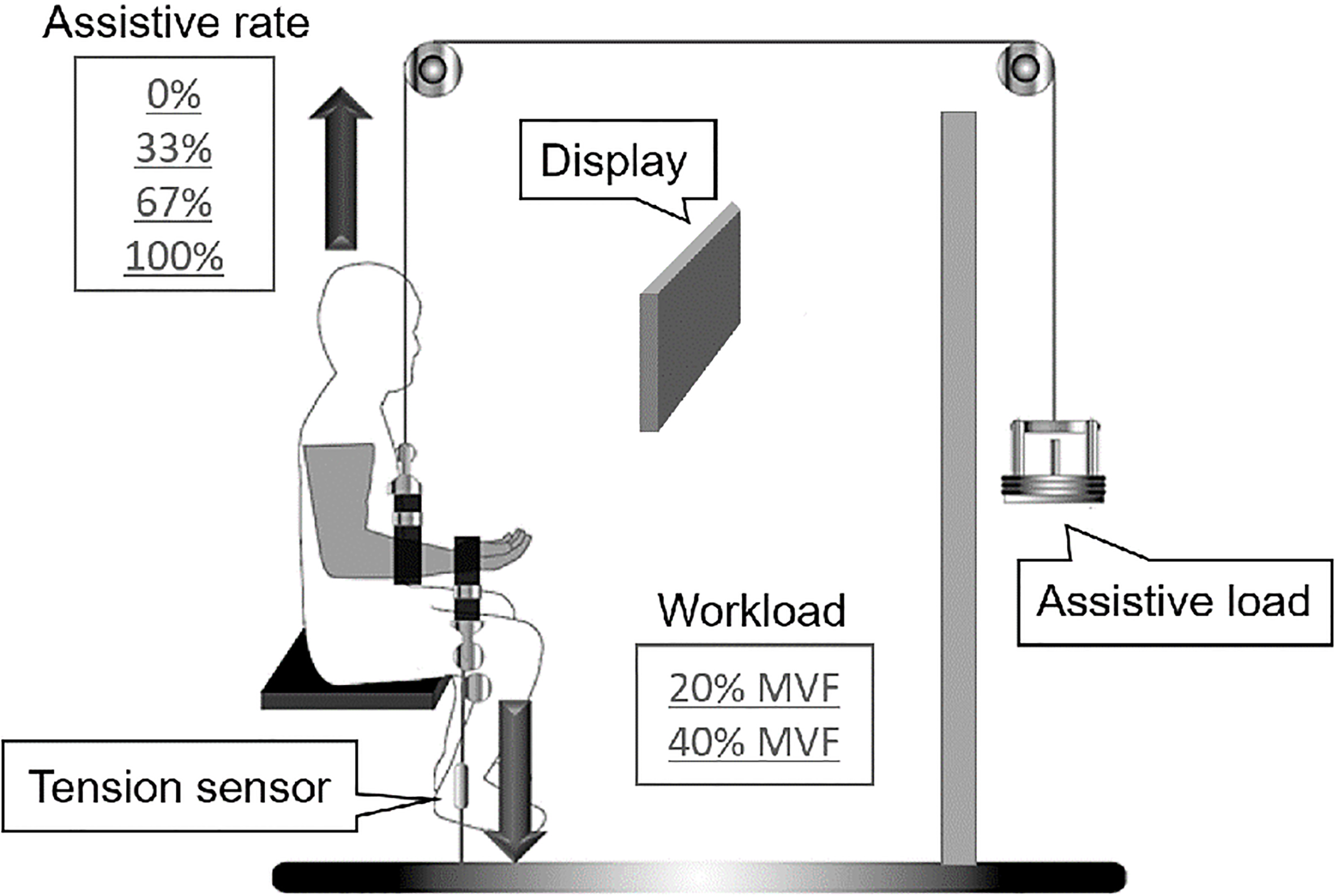
Figure 1 illustrates the experimental setup. Participants sat upright in an armless chair facing a monitor. The value of force exertion was shown on the monitor in real time, and each participant was instructed to adjust it to a target value. The dominant or the non-dominant arm was positioned at 90
A strap was fastened on the wrist to connect the forearm to a tension sensor that acted as workload and force measurement. Another strap was fixed in the middle of the length of the radius to support the forearm by connecting the forearm to assistive load through a fixed pulley system [5]. The height of the monitor was adjusted to eye level, and each participant affirmed that the value of force displayed on the monitor was clearly visible. A barrier was placed between participant and assistive load to prevent participants from anticipating the degree of assistance.
Experimental conditions
First, the maximum force that the arm can generate during isometric elbow flexion was identified. Workload conditions were determined based on the maximum force (20% and 40% maximum force), and four levels of assistive load were determined based on the workload conditions equal to 0%, 33%, 67%, and 100% workload. With the combination of workload and assistive load conditions, participants performed 8 trials in counterbalanced order.
Experimental protocol
Participants were asked to avoid high-intensity exercise that could cause muscle fatigue and influence task performance before the experiment day. Before the experiment, participants changed clothes into short-sleeved shirts and short pants that had been prepared. The experimental session consisted of a maximal isometric voluntary contraction (MVC) task and submaximal force matching task. The MVC task included the measurement of the maximal isometric voluntary force (MVF) and the maximal amplitude of the surface electromyography (sEMG) of biceps brachii (BB) and triceps brachii (TB). The submaximal force matching task with assistance was performed immediately after MVC. The dominant and non-dominant arms performed the experimental tasks in random sequence.
MVC task
Participants were instructed to maintain their arm positioned at 90
Force matching task with assistance
During the force matching task, participants were asked to maintain a workload that equals 20% and 40% MVF for 30 seconds with their elbow flexion maintained at 90
Two phases of the force matching task with assistance.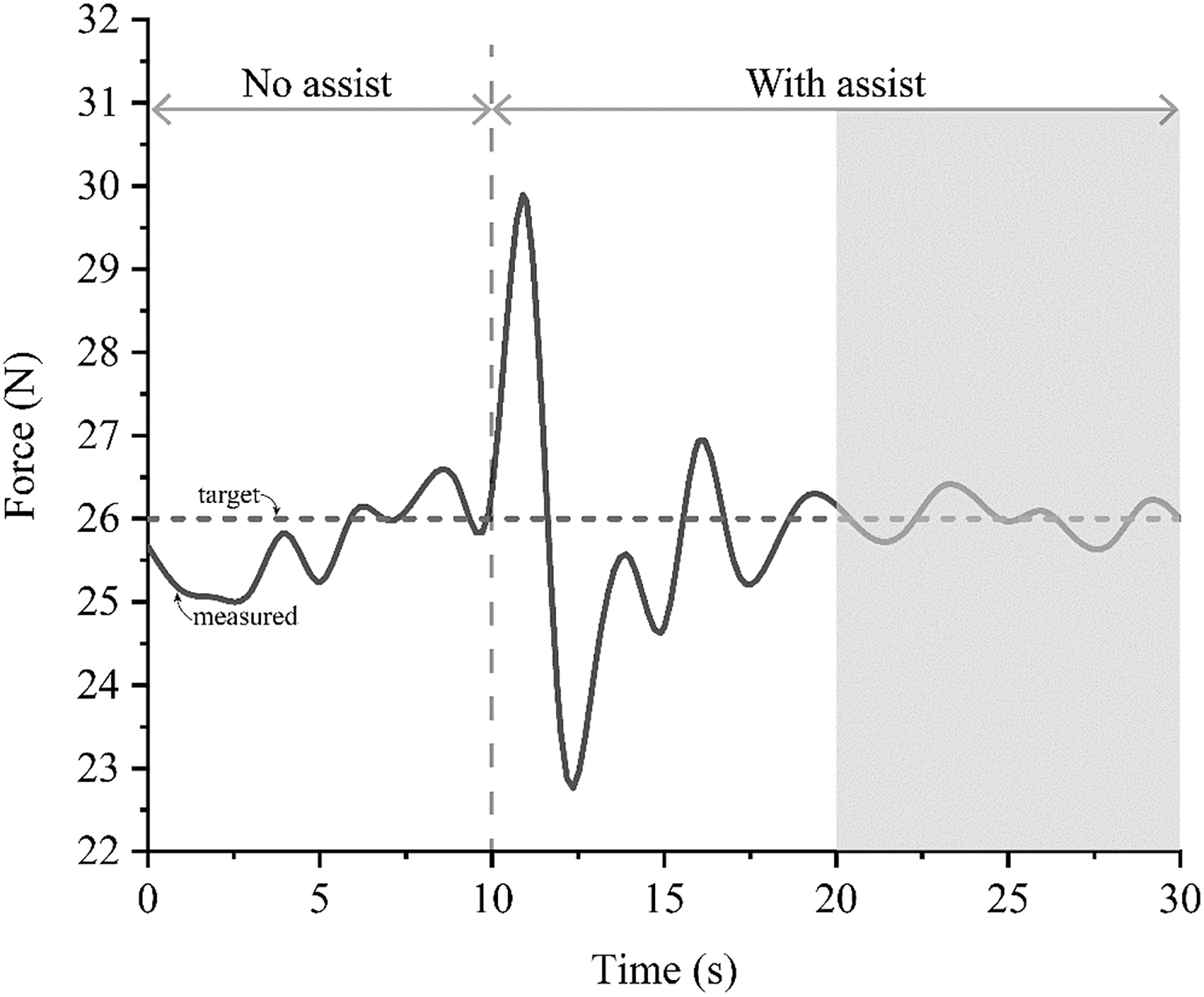
sEMG recordings
Before attaching the surface electrodes, the skin was gently scrubbed with an abrasive gel and cleaned with alcohol; an electrolytic gel was placed between the skin and the metallic part of the electrode to ensure signal quality. sEMG was recorded from BB and TB muscles. Disposable electrodes were placed above the belly of each muscle and the distance between the two electrodes was 2–3 cm. sEMG signals were amplified using a bio-amplifier (Bio Amp ML 132, AD Instruments Co., Australia).
Tension recordings
Tension during MVC and force matching tasks were recorded using a tension sensor (Attachment for tensile force, 30 kg, T.K.K. 1269f, Takei Scientific Co., Japan). The tension signal was amplified by a strain amp (strain amp TSA-210, T.K.K. 1268b, Takei Scientific Co., Japan).
Amplified analog signals of sEMG and tension were synchronized and converted into digital signals using PowerLab 16/30 (ML880, ADInstruments Co., Australia) and sampled at a frequency of 1 kHz with a band-pass filter of 10–500 Hz. These digital signals were imported to a personal computer and analyzed using LabChart v7.1.1 (AD Instruments Co., Australia) for further analysis. The sEMG signals were full-wave rectified and the amplitudes were normalized with respect to the MVC.
Perceived exertion
The rate of perceived exertion (RPE) during the force matching task was evaluated using Borg’s CR-10 Scale, which has a range from 0 to 10, with 0 being no muscle effort and 10 being maximum muscle effort. Participants rated the exertion directly after each experiment trial [18].
Data analysis
Muscle activity of BB and TB (%MVC)
The sEMG amplitude of BB and TB measured during the force matching trial was divided by the maximal sEMG of MVC for normalization. Muscle activity was evaluated by the normalized sEMG (%MVC).
Force steadiness (CV)
Fluctuation (force steadiness) in isometric force exertion was quantified by the coefficient of variation (CV).
Assist efficiency
Assist efficiency reflects the reduction rate of %MVC
The changes of muscle activity of BB (biceps brachii) at 20%MVF workload: (a) for the dominant arm; (b) for the non-dominant arm.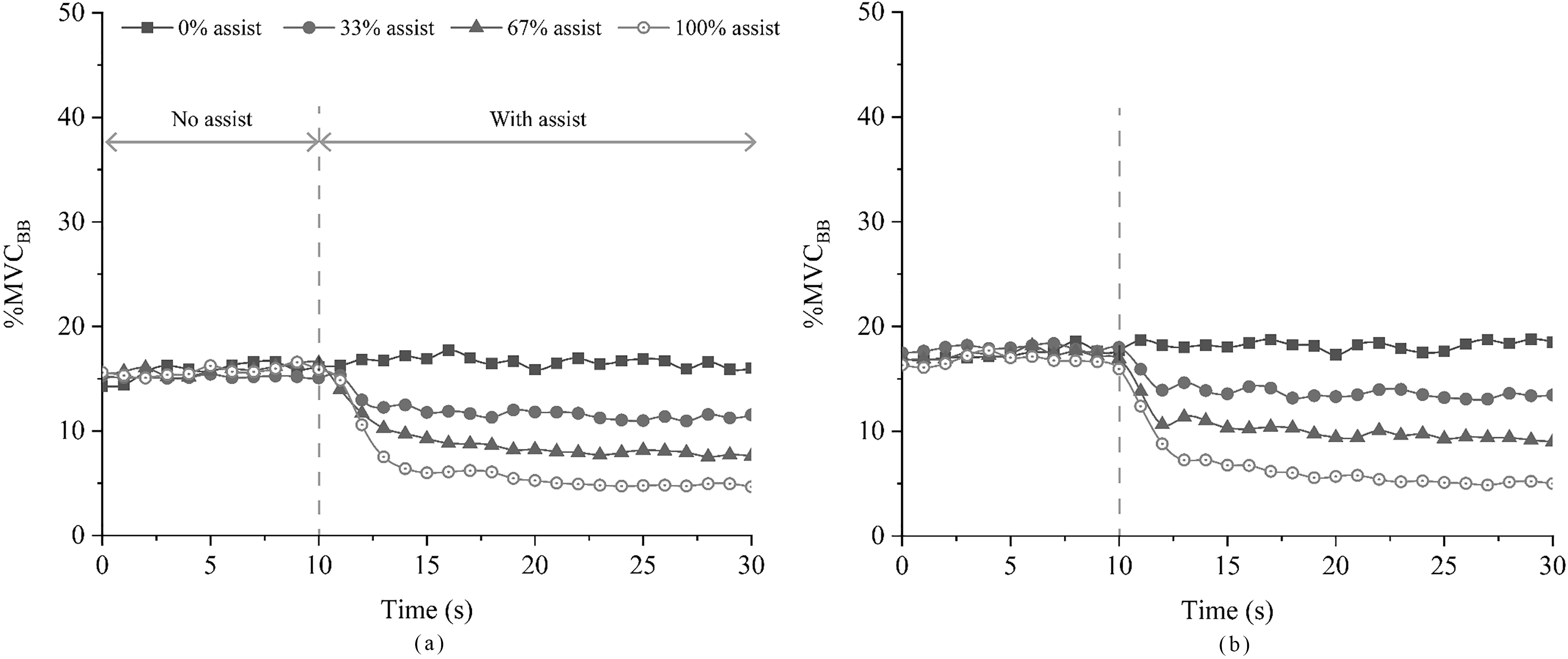
For the theoretical value of %MVC
Where, “0” refers to the theoretical %MVC
The analytic period of this experiment was defined as a 10-second interval from the 20th second when the force exertion began to stabilize to the end of the force matching task (emphasized by the shaded region in Fig. 2). This interval was also referred to as the steady period.
The changes of muscle activity of BB (biceps brachii) at 40%MVF workload: (a) for the dominant arm; (b) for the non-dominant arm.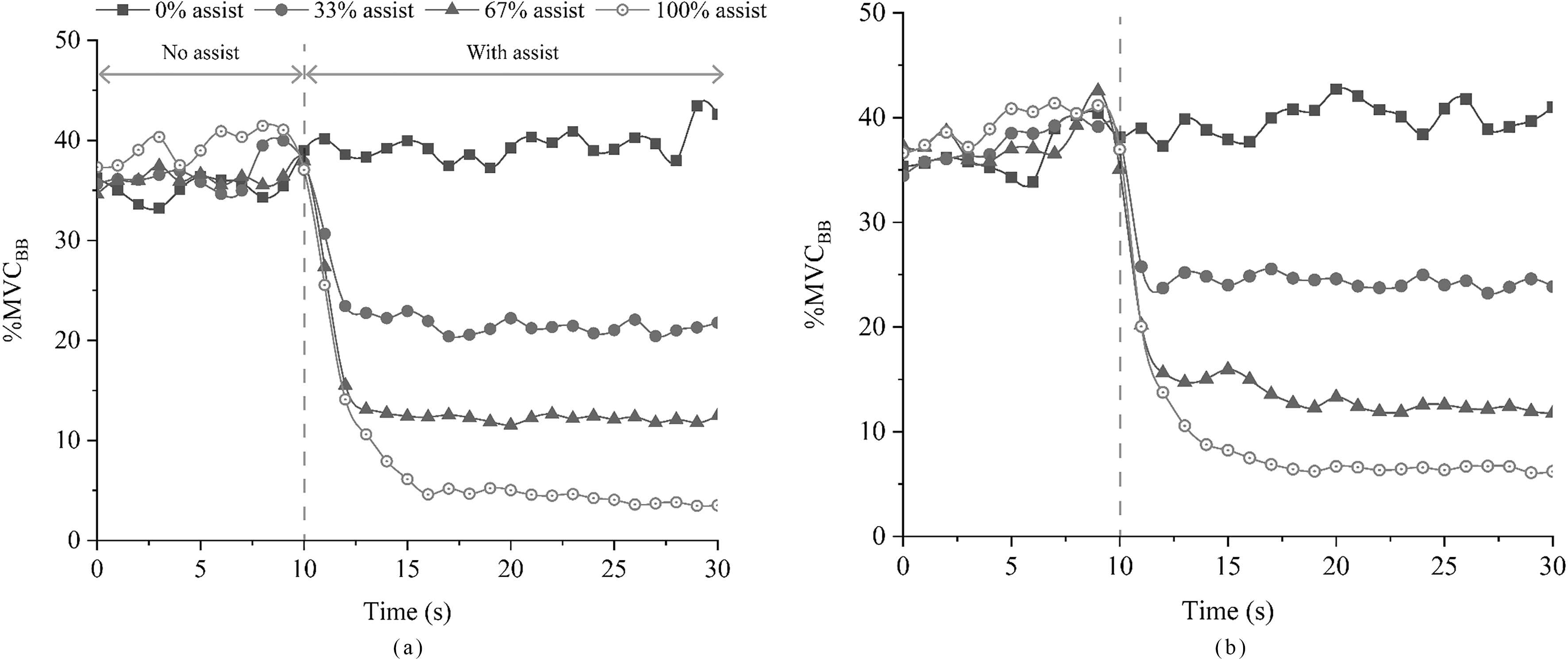
Mean muscle activity of BB (biceps brachii) of the dominant and non-dominant arms during the steady period: (a) for 20%MVF workload; (b) for 40%MVF workload.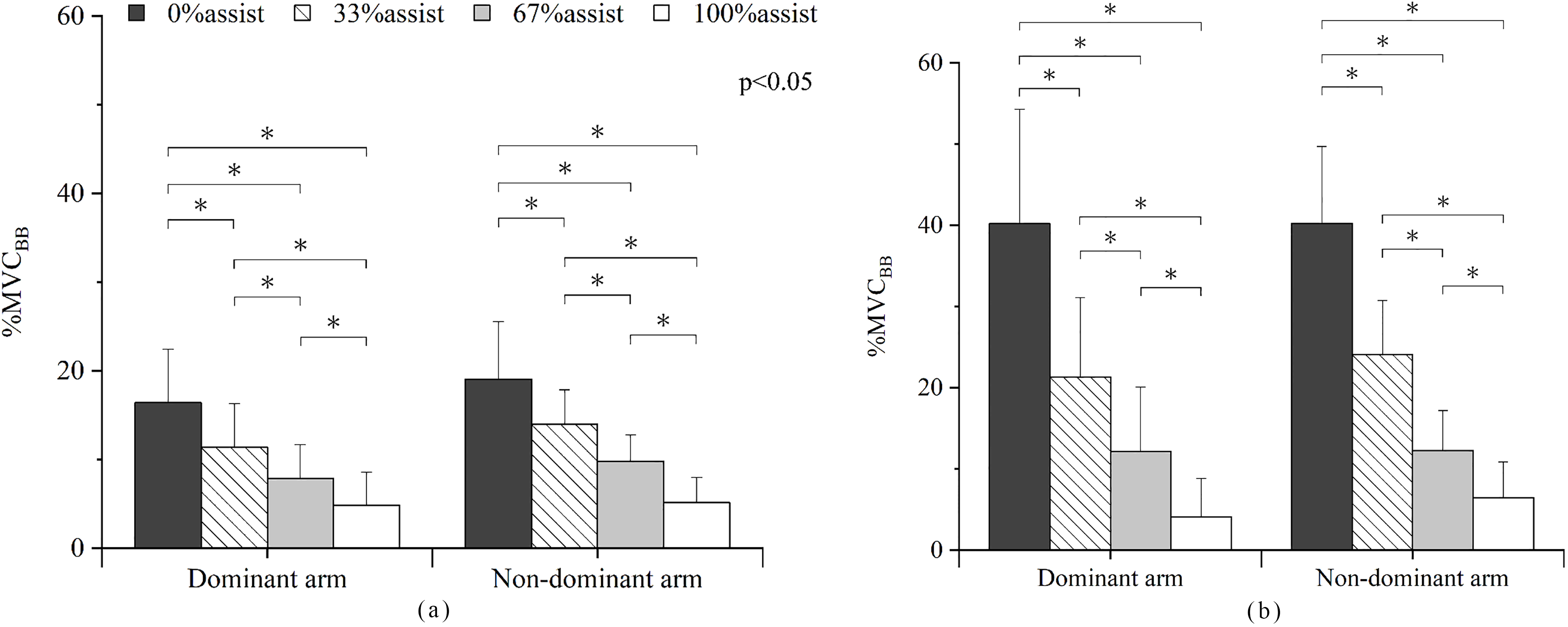
Assist efficiency of the dominant and non-dominant arms at different assistive levels: (a) for 20%MVF workload; (b) for 40%MVF workload.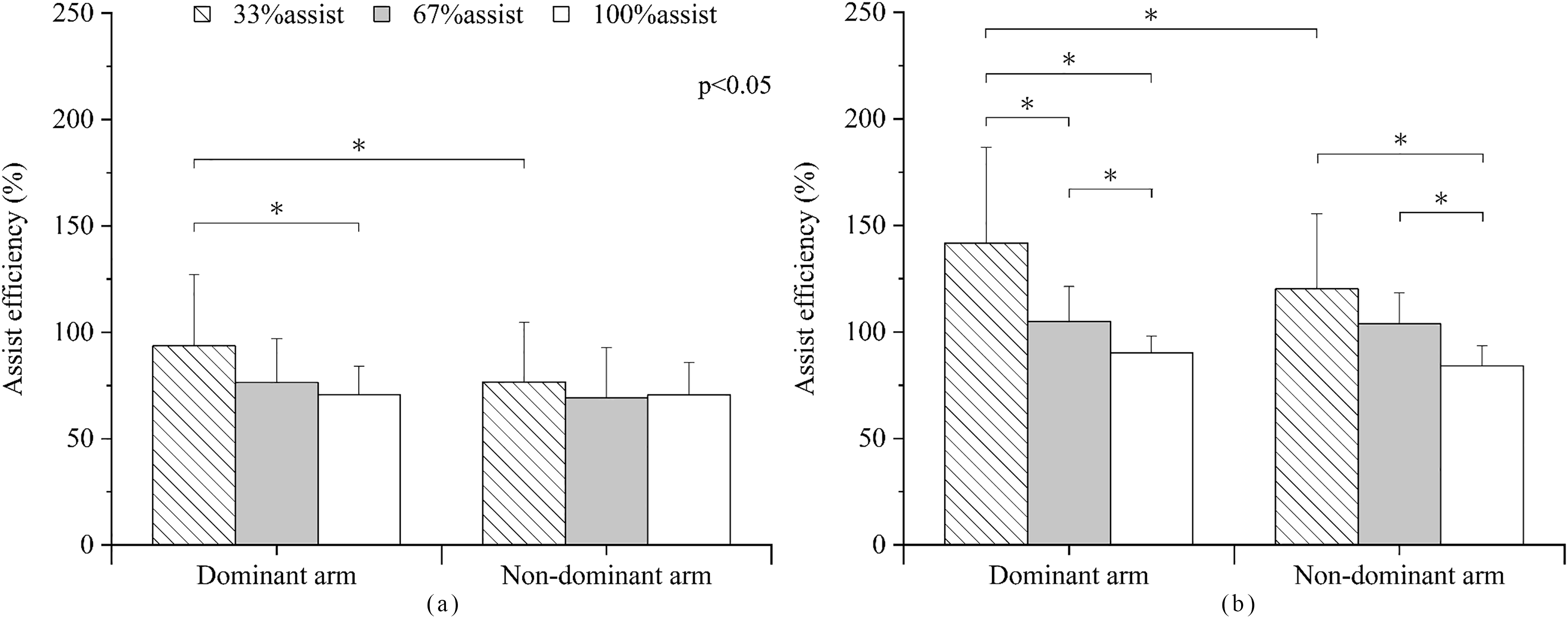
Mean muscle activity of TB (triceps brachii) of the dominant and non-dominant arms during the steady period: (a) for 20%MVF workload; (b) for 40%MVF workload.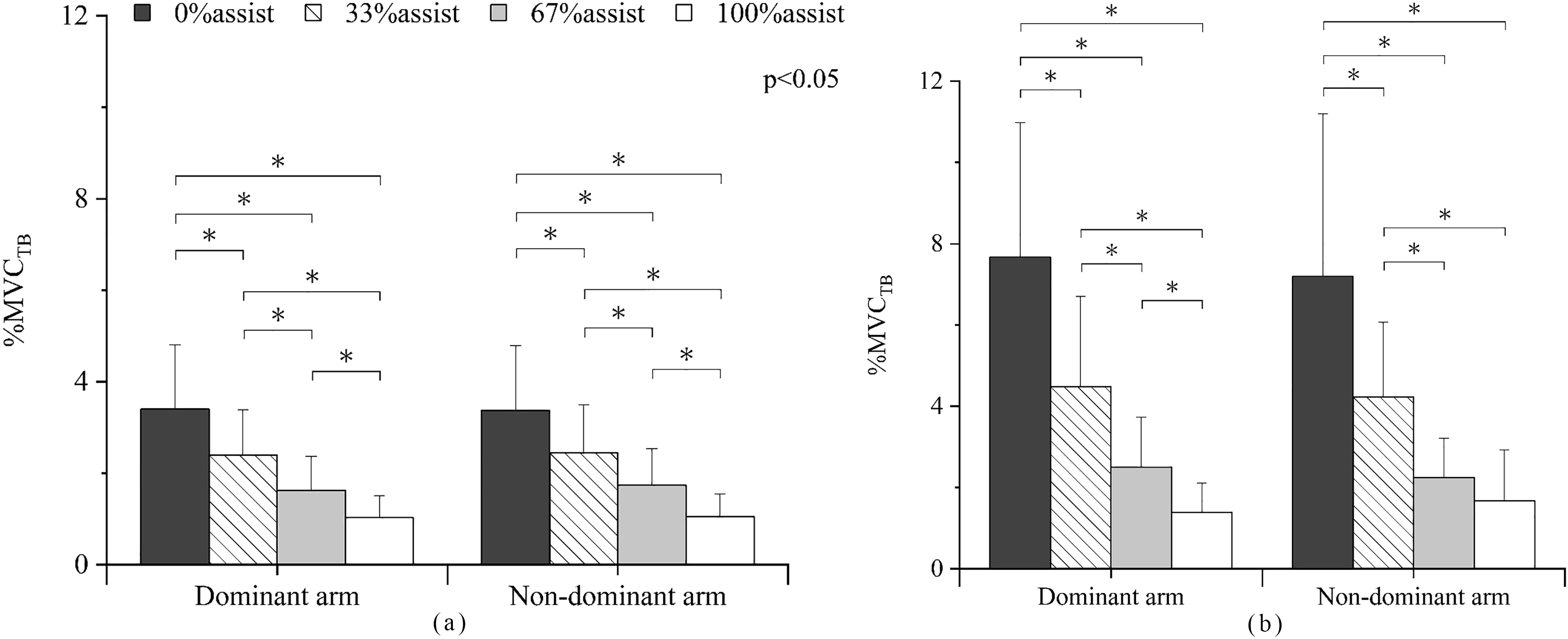
Perceived exertion of unilateral task performed by the dominant and non-dominant arms at different assistive levels: (a) for 20%MVF workload; (b) for 40%MVF workload.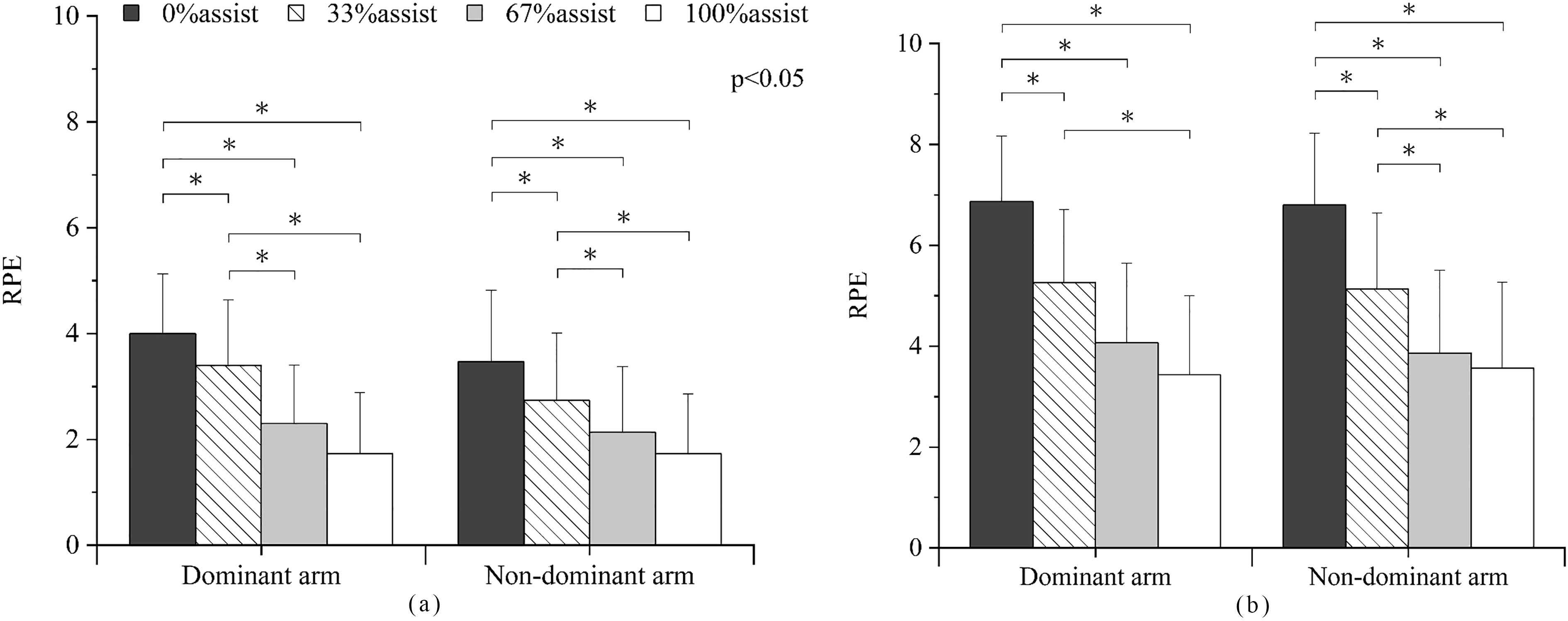
Steadiness (CV) of the dominant and non-dominant arms at different assistive levels: (a) for 20%MVF workload; (b) for 40%MVF workload.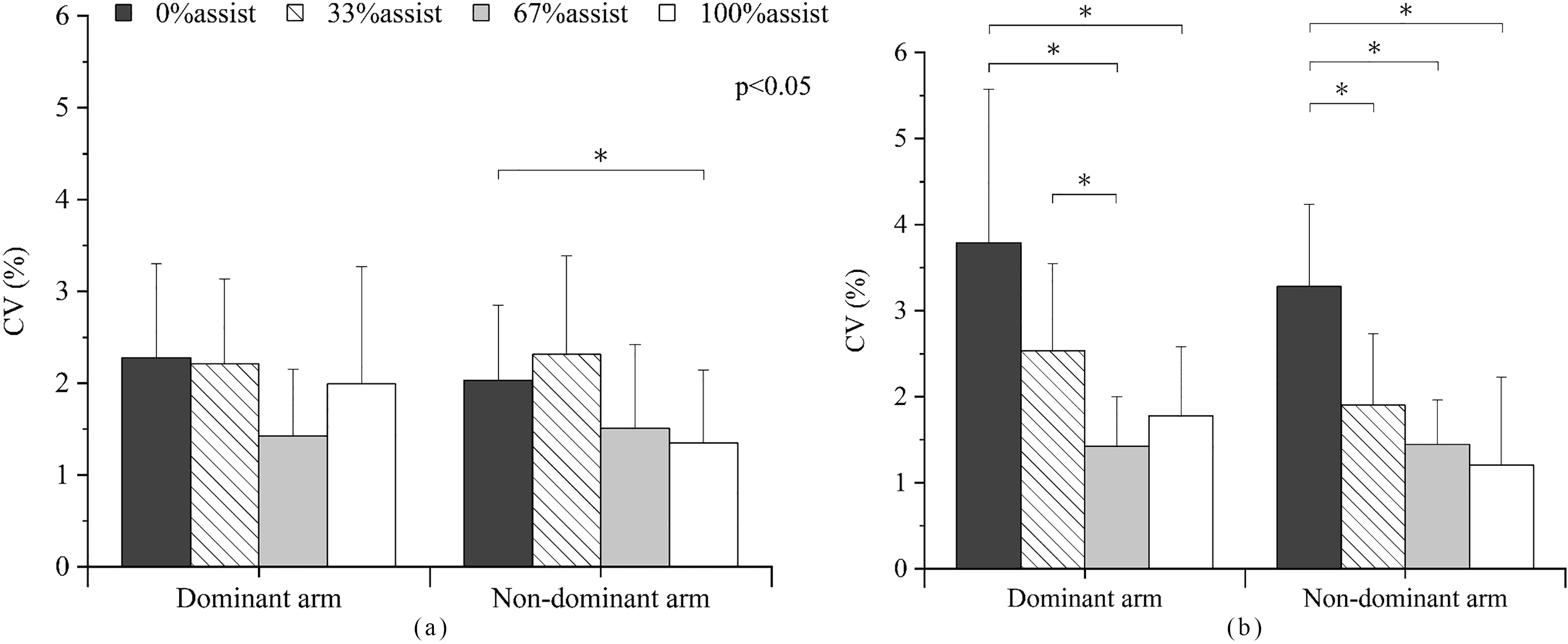
All statistical analyses were performed using IBM SPSS (version 24.0 software, Cary, NC, USA). Three-way ANOVA (arm conditions
Results
%MVC
of dominant and non-dominant arms
The changes of %MVC
The mean %MVC
Post hoc comparisons indicated significant difference among all assistive levels at both workloads. In general, at 20% and 40%MVF workloads, the %MVC
The assist efficiency of dominant and non-dominant arms during the steady period
The results of assist efficiency of the two arms at two workload conditions are showed in Fig. 6. Significant main effects of workload (
%MVC
of dominant and non-dominant arms
The mean %MVC
Perceived exertion
RPE of both dominant and non-dominant arms did not differ significantly (
Force steadiness of dominant and non-dominant arms
Force steadiness was significantly affected by workload level (
Discussion
The purpose of this research was to contrast the task performance of dominant and non-dominant arms at different workload levels (20% and 40%MVF) with different assistive levels (0%, 33%, 67% and 100%) by analyzing the muscle activity of the biceps, triceps, and force variation of the two arms. According to dominant arm advantages in task performance [7, 8], we hypothesized that the dominant arm would have a better performance to accommodate the assistive force compared with the non-dominant arm.
A comparison of muscle activity of dominant and non-dominant arms
Muscle activity of biceps brachii
The agonist muscle of both arms showed similar responses when adapting to the assistive force: decreasing gradually after the assistive force was applied and stabilizing after several seconds. By visual inspection, there was no drastic changes in the %MVC
The assist efficiency
Assist efficiency, which reflects the reduction rate of %MVC
Most importantly, the results in this experiment showed that the assist efficiency of the dominant arm is significantly higher than that of the non-dominant arm at 33% assistance (Fig. 6). This lower efficiency of the non-dominant arm, especially at the low assistive level, could be due to motor control differences between the two arms. The explanation can be discussed as follows:
(1) Why was the laterality of assist efficiency only found at a low assistive level?
As reported in previous study, forceful voluntary isometric muscle contraction that last at least 5 seconds can bring about rapid changes in excitability in the motor cortex and spinal reflexes that last long after the cessation of the contraction, thus resulting in a prolonged involuntary contraction [20]. In the experiment trials, the application of intensive assistance could be regarded as cessation of the muscle contraction. Before the assistance can be applied, participants maintained 20% or 40%MVF isometric elbow flexion for 10 seconds, which might be intensive enough to induce an involuntary contraction of BB. Additionally, voluntary contraction of BB occurred during assistance to prevent injury caused by sudden assistive force. Consequently, after an intensive assistive force is applied, especially at 100% assistance, voluntary and involuntary muscle contractions might exist simultaneously. In contrast, for low assistance (33%), the assistive force might not be powerful enough to induce cessation of muscle contraction, therefore, there would primarily be voluntary muscle contraction throughout the trial. Moreover, the control of voluntary contraction would be affected by motor control differences between the arms (explained in detail subsequently). Thus, the laterality of assist efficiency was demonstrated at a low assistive level.
(2) Why was assist efficiency of the non-dominant arm lower than that of the dominant arm?
It has been suggested that voluntary movement of the dominant hand is controlled mainly by the brain hemisphere contralateral to that hand, whereas the non-dominant hand is controlled by both hemispheres [9, 10]. Due to interhemispheric transmission delays, the non-dominant arm has disadvantages in performance, such as motor control and coordination [6, 11]. Correspondingly, a previous study also reported greater muscle activity in the non-dominant arm compared with the dominant arm during dynamic movement [21]. Similarly, during isometric elbow flexion, the motor control of the non-dominant arm might not be as efficient as the dominant arm, thus resulting in extra contractions of BB when accommodating external assistive force.
Overall, both dominant and non-dominant arms showed the ability to utilize the external assistive force to reduce the muscle activity of BB. However, due to the performance disadvantages of motor control, the non-dominant arm reduced the muscle activity of BB less efficiently compared with the dominant arm, especially at a low assistive level.
Muscle activity of triceps brachii
During isometric contraction, both the agonist and antagonist muscles contract at the same time to maintain joint stability [22, 23]. Similarly, in this experiment, the antagonist (TB) was co-activated with the agonist (BB) at an unassisted stage, and the %MVC
Rated perceived exertion
RPE also showed a similar tendency in response to increased assistive force as that observed in %MVC
A comparison of force steadiness (CV) of the dominant and non-dominant arm
It is known that muscle force steadiness could be influenced by the muscle group performing the task, the type and the intensity of the muscle contraction, and the physical activity status of the individual [24]. In the present study, CV of both dominant and non-dominant arms were greater at 40%MVF workload compared with that at 20%MVF workload. This result is in line with a previous study that indicated that CV of force increases as the level of the target force increases [25].
Bilateral difference was also found in the CV result. The non-dominant arm appears to be more capable of controlling force exertion with higher accuracy compared with the dominant arm (Fig. 9). This laterality of force control ability between arms might be due to two reasons: different intensity of the target force and a bilateral difference in motor control strategies.
In the present experiment, participants performed the isometric elbow contraction with each arm. Although the workload conditions (20% and 40%MVF) were the same for both arms, the target force intensity was different. The mean MVFs of the dominant and non-dominant arms were 161.8
Additionally, from the perspective of lateralization of control strategies of the two arms, Bagesteiro and Sainburg (2003) proposed a dynamic dominance model in which the dominant arm system more effectively anticipated task dynamics due to feedforward control mechanisms, whereas the non-dominant arm specialized in the control of the steady-state position due to sensory feedback mediated error correction mechanisms [13, 26, 27]. Similarly, in this experiment, from the result of assist efficiency, one can observe the specialization of the dominant arm for controlling muscle contractions in response to the external assistive force. From the CV results, one can observe the specialization of the non-dominant arm with greater force exertion accuracy at the steady state. Accordingly, control strategies in the dynamic dominance model might also be adaptable to this experiment: performances of the dominant arm might be characterized by a feedforward control strategy that enables it to take advantage of external assistive force. In contrast, performances of the non-dominant arm are probably related to impedance control that selectively modifies arm impedance independently of force [28].
Implication on rehabilitation
In the PAS-assisted rehabilitation scenario, pre-training session is required. The PAS is often directly mounted on the patients’ body, which makes it necessary for the patients to practice interacting with the dynamic operation as well as to coordinate with the external force provided by the PAS. Our findings regarding muscle activity indicated a comparatively lower ability of the non-dominant arm to utilize the external assistive force, which indicates that the non-dominant arm may require longer pre-training in order to adapt to the assistive force and make more effective use of it.
Moreover, our findings also suggested different control strategies for the two arms of healthy people when performing PAS-assisted movement. Further, a previous clinical study has demonstrated distinct control mechanisms involved in the production and coordination of forces for post-stroke [29]. These findings give insight into the control methods of rehabilitative PAS. For instance, PAS might need to control each arm in accordance with its control characteristics to achieve a better training effect, such as, feedforward control for the dominant arm and impedance/feedback control for the non-dominant arm, or distinct control mechanisms for the less-impaired limb and the impaired limb.
Limitations and future study
The present study found different specialties of the two arms in response to external assistive force. However, there are several limitations of our study, including movement form (static, isometric contraction, unilateral elbow flexion), workload intensity (20% and 40%MVF) and duration (30 seconds). If these factors are changed, physiological responses of the dominant and non-dominant arms might be different, and different specialties of the two arms might be observed. Further research is necessary to examine the specific responses of the two arms against various intensities of external assistive force during bilateral elbow flexion and dynamic movement.
Conclusion
Comparison of the task performance of dominant and non-dominant arms at various workloads and assistive levels showed that during unilateral elbow isometric contraction, the muscle activity of BB and TB, perceived exertion, and CV of both arms decreased with the intensity of assistive force, which indicates that both arms are capable of utilizing external assistive force. However, the two arms showed different abilities in response to external assistive force. The dominant arm utilized the assistive force more efficiently, especially at a lower assistive level, which suggests the necessity for the non-dominant arm to take more practices to accommodate to the PAS at pre-training session. On the other hand, the non-dominant arm could maintain a force with higher accuracy. The different advantages of the two arms in performance indicate distinct motor control strategies of each arm and implicate the necessity of the corresponding control method of rehabilitative PAS of each arm to achieve a better training effect.
Footnotes
Acknowledgments
This work was supported by KAKENHI JP15K 14619 and JP17H01454.
Conflict of interest
None to report.