
Abstract
BACKGROUND:
Strengthening exercises help improve physical function and muscle strength in knee osteoarthritis (OA). However, optimal exercise programmes for treating knee OA remain unclear.
OBJECTIVE
: To compare efficacy of isometric exercises performed at different angles and isokinetic exercises in patients with knee OA.
METHODS:
Patients were randomly divided into two groups. For four weeks, Group I (
RESULTS:
VAS on movement, WOMAC, Leuqesne and SF-36 physical scores improved from T0 to T2 within each group, but Grade 3 and Grade 4 patients in the Group I showed better results compared with Group II at T2. Isokinetic exercise yielded higher extensor PM values than its isometric counterpart at T2 (
CONCLUSIONS:
Both isokinetic and isometric exercises were effective in the treatment of knee OA of all grades in terms of pain reduction and functional improvements. However, isokinetic exercise produced longer lasting effects than isometric exercise.
Introduction
Knee OA is a chronic degenerative disease characterised by articular cartilage damage, thickening of subchondral bone and osteophytes on the joint surfaces, resulting reduced muscle strength [1, 2]. The global prevalence of symptomatic knee OA is estimated to be 3.8% and it is one of the major health problems causing disability throughout the world. According to a previous study, the global burden of hip and knee OA has a significant impact on disability-adjusted life years [3]. The aetiology of the disease includes patient-related factors (age, gender, obesity, genetic) and local (trauma, occupational use) factors [4].
The most common symptoms in patients diagnosed with OA are pain and functional limitations [5], both of which reduce the quality of life [6]. Another important finding related to the disease is impaired muscle function, which causes weakness of the quadriceps muscles. This situation may occur before the onset of pain or muscle atrophy [3, 7]. There are studies in the literature that emphasise how reduced quadriceps muscle strength may cause OA [8]. However, there is no consensus on whether muscle weakness is a cause or consequence of the disease.
The radiographically generated Kellgren-Lawrance (KL) scale is commonly used to determine the state of knee OA. It has been shown that for the development of the radiological characteristics of KL Grade 1, approximately 5 years have likely already passed since the onset of the disease [9]. It has also been found that decreased performance of the lower extremity predicted the development of radiographically observable knee osteoarthritis 5 years later [10]. These results show us that the disease should be seriously addressed in its very earliest stages [8].
Over time, the need for functional assistance is increasing in patients with advanced stage of knee OA. Treatment designed for osteoarthritis should intend reducing pain, improve joint mobility and movement restriction. Therefore, selecting the most appropriate treatment for each patient has a critical importance. Despite advances in research and new treatment methods, there is actually no cure for the knee OA [4, 11]. Many guidelines recommend exercises in the early stages of the disease to avoid the possibly adverse effects of pharmacological treatment [6, 12, 13], and indeed there are many effective exercise programmes for controlling pain and maintaining function, although their effects can vary widely [4]. Of particular interest regarding knee OA is the importance of improving strength, especially in the quadriceps muscle group, and exercises to achieve this result include isometric, isotonic and isokinetic approaches. Isometric exercises are types of strength training in which the joint angle and muscle length do not change during contraction, and therefore this approach can be advantageous in the early stages of knee rehabilitation in cases where the range of motion is restricted due to pain [14]. No physical work is performed during isometric exercise. Intensity and duration combination reflects the energy consumption of an isometric contraction [15]. In addition, muscle strength increases in isometric exercise are specific to the angle applied. This situation can be regarded as a disadvantage of isometric exercise. To deal with this problem, strength training protocols were suggested to be done at varying joint angles. Even though many studies on varying types of muscle contractions were relatively major, a small number of these studies have compared isometric to dynamic exercises such as isotonic and isokinetic trainings. The authors reported that isometric and dynamic exercises showed equivalent isokinetic strength gain [16, 17, 18]. It was also concluded that isometric exercise performed at different angles should be especially considered as an alternative strength training since it induces the most noticeable and fastest increase in muscle moment [17].
Isokinetic exercises are device-assisted movements that can increase the strength of a muscle throughout its full range of motion. The velocity of the joint movement is constant at all angles except for the acceleration and deceleration phases and can be determined by a computer-controlled system as low, medium or high. The force that is applied by the patient varies depending on how much effort is exerted by pushing or pulling on the lever arm of the isokinetic dynamometer. Isokinetic measurement devices can provide a large quantity of objective data that can be used to evaluate and analyse both muscle strength and the effectiveness of various treatments. However, the need for trained personnel and expensive equipment are the main disadvantages that restrict the clinical use of isokinetic exercises for the specific treatment of knee OA [19].
Although the positive effect of exercise is well known [20, 21, 22], it is not clear which type of strengthening protocol is more productive regarding grades of knee OA. The number of quality investigations in which isokinetic exercise are compared with other exercise modalities is minimal [4, 23, 24, 25, 26, 27, 28, 29]. It is also not known whether isometric exercises performed at different angles would increase muscle strength in a way similar to the isokinetic method. Therefore, the aim of this study was to compare the efficiency of isokinetic and isometric exercise programmes performed at various angles in patients with different grades of knee OA.
Methods
Only patients with bilateral primary knee OA at KL Grade 2–4 and those with knee pain for at least 3 months were included in the study. We excluded patients with a history of cardiovascular or pulmonary disease that prevented exercise, as well as those with inflammatory or infectious pathology of the knee joint, uncontrolled endocrinological disease, and anyone who had experienced knee surgery or prosthesis placement, or who had a neurological disease affecting the knee joint innervation and restricted ambulation.
The local ethics committee approved this study (Trakya University Medical Faculty Ethics Committee, 25.01.2012, TUTF-GOKAEK 2011/11) and participants provided written informed consent. A total of 48 women patients with knee OA were evaluated, and 32 of them were included in this study. Sixteen patients was excluded from the study because of they had cardiopulmonary disease (2 patients congestive heart failure, 1 patient chronic obstructive pulmonary disease), inflammatuar arthritis (3 patients rheumatoid arthritis, 1 patient ankylosing spondylitis), history of knee surgery and prosthesis (3 patients knee arthroscopy, 2 patients knee prosthesis placement) and knee flexion contracture (2 patients). Two patients declined to participate to study. Our patients ranged in age from 40 to 70 and had earlier been admitted to the Physical Medicine and Rehabilitation Outpatient Clinic of the Trakya University Faculty of Medicine. In each case, the diagnosis of knee OA was based on the criteria specified by the American College of Rheumatology.
This study was designed as a prospective single-blind, randomised investigation, therefore the clinician who assigned and evaluated the patients was blinded to the treatment the patient received. Eligible patients were allocated into two groups via block randomisation. A computer random number generator was used to select random permuted blocks with a block size of four and a similar allocation ratio. Two different exercise methods were used in the current study, and the isokinetic exercise patients were put into Group I, while those undertaking isometric exercises were in Group II. There were 15 patients (30 knees) in Group I, 17 patients in Group II (34 knees). Patients in each group was divided into subgroups as Grade 2, 3 and 4 knee OA. A total of 64 knees in 32 patients were subjected to the exercise sessions. The estimation of sample size was determined on the basis of a greater improvement of muscular strength in the quadriceps of the treated knee in isokinetic group compared to the isometric group derived from previous literature [23]. It was provided a power of 80% at a significance level of 0.05 (a two-tailed
We recorded the height, weight, medical history, lower extremity dominance, level of education, occupation and duration of complaints of each patient. All were evaluated at the beginning of the treatment (week 0, T0), at the endpoint of the treatment (week 4, T1) and at the control point (week 10, T2) for the following parameters:
Radiological score – initially determined by the KL scale (Grade 2–4).
Pain intensity – evaluated using a 10 cm long Visual Analogue Scale (VAS) during both rest and activity (0
Thigh circumferences – were evaluated by measuring at 10 cm proximal to the top of the patella. These measurements were recorded in cm.
Knee range of motion (ROM) – The active ROM was measured with goniometer with movable double arms, marked in 5
Functional status – was assessed with the Western Ontario and McMaster Universities Arthritis Index (WOMAC), which consists of 24 questions, specifically 5 for pain, 2 for joint stiffness and 17 related to functional status, each being scored from 1 to 5. On this metric, a high score suggests bad health, while relatively healthy subjects will have a low score. The assessments were grouped into four classifications, specifically WOMAC A for pain, WOMAC B for joint stiffness, WOMAC C for function status, and WOMAC-Total for the total score.
We determined the severity of the knee OA by using the Lequesne Index, which is an 11-item questionnaire addressing pain/discomfort, maximum walking distance and daily living activities. Like with the WOMAC, a high score suggests poor health while lower scores suggest better overall functioning. The assessments were as follows: Lequesne A for pain-discomfort, Lequesne B for maximum walking distance, Lequesne C for daily living activities and Lequesne-Total for the total score.
We measured quality of life using the Short Form-36 (SF-36), which consists of 36 questions and includes 2 summary scales (physical and mental), both of which were utilised in our current study. In this case, a high score indicates good health and a low score indicates poor health.
Muscle strength was evaluated with an isokinetic test and exercise system (CSMI Cybex HUMAC/ NORM, model number: 502140, China). Patients were familiarised with both the equipment and the test protocol, and the equipment was calibrated prior to each test. Each patient was allowed to warm up for 10 minutes on the bicycle ergometer and was then seated on an isokinetic test chair with the hip joint flexed at 90
Isokinetic exercise group
Patients were allowed to warm up for 10 minutes on the bicycle ergometer before each isokinetic exercise session and the equipment was calibrated prior to every session. The patients were then positioned into the isokinetic test and exercise system as described previously. The isokinetic exercise programme was performed for each knee during 3 sessions a week for 4 weeks (12 sessions). Each knee of the patients was subject to an isokinetic exercise programme consisting of 10 repetitions at 180
Isometric exercise group
For this part of the study, each patient was allowed to warm up for 10 minutes on the bicycle ergometer before each isometric exercise session, for which the equipment had previously been calibrated. The patients were then positioned into the isokinetic test and exercise system as described previously. The angle of the knee joint is 0
Sociodemographic and clinical data
Sociodemographic and clinical data
Intra and intergroup comparisons of VAS scores
VAS: Visual Analog Scale; T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a, b, c): different letters in the same column indicate a significant intragroup difference in scores between time points for the different subscales. *
After 4 weeks of treatment, each group was given a home exercise programme specifying the use of isometric methods addressing the quadriceps, including straight leg lift, hip abduction-adduction and mini-squatting exercises. All subjects were instructed not to use NSAID during the study. Only paracetamol was allowed, if necessary. Also, it was not allowed to take paracetamol two days before evaluations.
Statistical analyses were performed using the SPSS software (SPSS Statistics for Windows 20.0; Licence code 10240462, SPSS Inc). The Kolmogorov–Smirnov test was used to define whether two random samples had normally statistical distributions. Parametrically distributed variables were tested using the independent samples test. The Mann-Whitney U test was used to compare the non-normally distributed continuous variables between the two groups. The Friedman variance analysis was used to compare repeated measures in the two groups, while the Wilcoxon signed-rank test was used to compare paired data. The Bonferroni correction was applied for multiple comparisons. The Pearson test was used to determine the correlation of the qualitative data. The data we obtained from the study were expressed as median (med), minimum-maximum (min–max) and mean
The flow chart summarizing the distribution of participants during each stage of the study.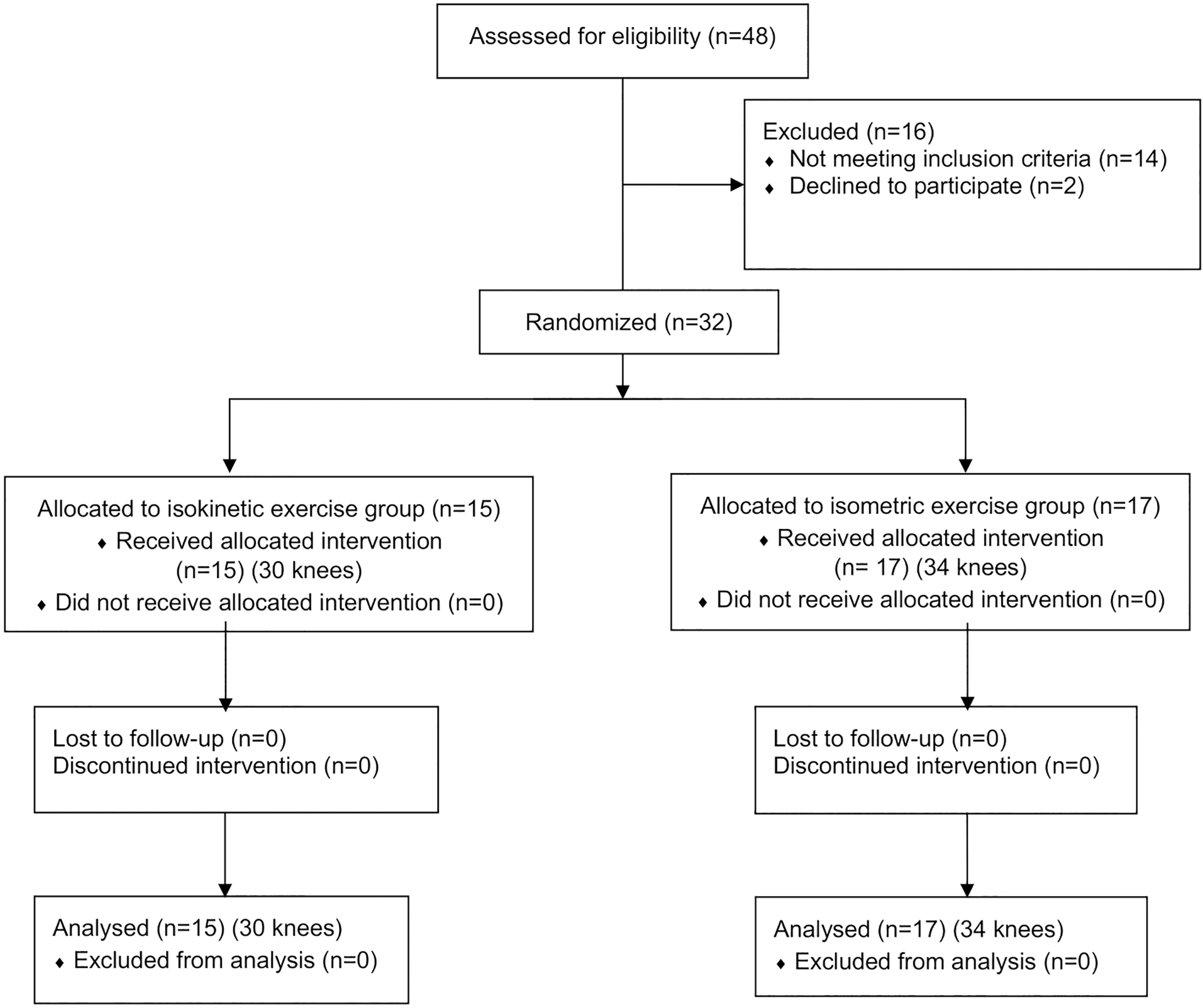
A flow chart summarising the distribution of participants during each stage of the study is shown in Fig. 1. A total of 48 women patients with knee OA were evaluated and 32 were included in the study. All of them (15 in the Group I and 17 in the Group II) completed the 4 weeks of treatment and attended the 10-week post-treatment follow-up programme. A total of 64 knees in 32 patients were subjected to the exercise sessions.
Intra and intergroup comparisons of WOMAC scores
Intra and intergroup comparisons of WOMAC scores
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a, b and c): different letters in the same column indicate a significant intragroup difference in scores between time points for the different subscales. *
Intra and intergroup comparisons of Leuqesne scores
T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a, b, and c): different letters in the same column indicate a significant intragroup difference in scores between time points for the different subscales. *
Intra and intergroup comparisons of measurements of thigh circumference (cm)
T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a and b): different letters in the same column indicate a significant intragroup difference in scores between time points.
Intra and intergroup comparisons of extensor PM values (Newtonmetre)
T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a, b): different letters in the same column indicate a significant intragroup difference in scores between time points. *
Intra and intergroup comparisons of flexor PM values (Newtonmetre)
T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a, b): different letters in the same column indicate a significant intragroup difference in scores between time points.
Intra and intergroup comparisons of SF-36 scores
T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a, b, c): different letters in the same column indicate a significant intragroup difference in scores between time points. *
Intragroup and intergroup comparisons of ROM values of the knee joint
T0: baseline; T1: treatment endpoint; T2: 10 week follow-up; superscript letters (a and b): different letters in the same column indicate a significant intragroup difference in scores between time points.
There was no significant difference across the sociodemographic and clinical data of the participants (Table 1).
VAS scores (at rest and on movement) in patients of all grades in each group at different times are shown in Table 2. Evaluating intragroup comparisons, Grade 2 and Grade 3 patients had a significant decrease in pain severity at rest and on movement from T0 to T1 (
A significant decrease in WOMAC (A, B, C, total) and Leuqesne (A, B, C, total) scores were observed from baseline to T2 in patients of all grades within treatment groups (
A significant increase was obtained in thigh circumference measurements from baseline to T1 and T2 within both Group I and II, except for Grade 4 patients in isometric group at T2 (Table 5). In addition, there was no difference among thigh circumference measurements of both groups at all-time points for all grades (
Considering extensor peak moment (PM) values, patients of all grades in Group I experienced a significant increase from baseline to T1 and T2 at 60 and 180
Evaluating flexor muscle PM values at 60 and 180
In the SF36 evaluation, statistically significant improvements were noted in the physical scores within both groups from baseline to T1 and T2 (
Considering ROM values, there were no significant differences in Grade 2 and Grade 3 patients for both groups at any of time periods. Grade 4 patients in both groups showed significant improvements from T0 to T2 in terms of ROM values. However, there were also no differences among ROM measurements of both groups at all-time points (Table 9).
This is the first randomised trial to directly compare the effects of isokinetic vs isometric exercises performed at different angles in patients with knee OA, who were evaluated to be at Grade 2–4 according to the KL scale. Based on the findings of the current study, satisfactory improvements were observed in both groups. The primary aims of knee OA treatments such as reducing pain and improving function, were reached at the endpoint of treatment and also during 10 weeks of follow-up by using these exercises. Especially, VAS scores on movement decreased significantly in all treated groups after treatment and at T2. However, Grade 3 and Grade 4 patients in isokinetic group showed lower VAS scores compared with other group in the follow-up period. This result supported the idea that strengthening exercises had a positive effect on the treatment of knee OA, as has been reported in a number of previous studies [5, 11, 12, 13]. It was also mentioned in another investigation that these exercises had comparable beneficial effects regarding the use of NSAİDs, in terms of pain reduction and functional improvements [22]. Therefore, it was evident that carefully applied exercise programmes can be an important alternative to the pharmacological treatment of knee OA, especially in light of the possibility of undesirable side effects when using drugs.
The knee joint stability and mobility are related to the optimal function of quadriceps and hamstring muscles as well as the strength of these muscles [4]. Effects of isokinetic, isometric, and aerobic exercise protocols on pain and physical function in knee OA were studied by Kucuk et al. [32]. All exercise programmes improved pain and functional capacity. Isokinetic exercise also increased the muscle strength with improved maintenance of the hamstring/quadriceps ratio. The shortcoming of that study was the lacking of performing hamstring isometric contractions [32]. In our study, we performed both quadriceps and hamstring isometric contraction at 0
Another dimension of this study was the question of whether isometric exercises performed at different angles would have similar effects to those produced by isokinetic exercise performed throughout the full ROM. We were able to rigorously address this issue because of how our dataset was objectively acquired through the use of an isokinetic device to assess muscle strength. In the current study, significant progress with regard to extansor muscle strength was observed after isokinetic exercise in patients of all grades at all angular velocities. By contrast, only Grade 3 patients in isometric group showed significant improvements after treatment at 60
A number of earlier randomised controlled trials reported that the increase of muscle strength was higher after exercising compared to control groups [24, 25, 27]. According to the data we obtained, isokinetic exercises resulted in significantly higher extensor PM values than isometric exercises in Grade 2 and Grade 3 patients at 180
As is well known, an increased load at the knee is an important risk in the pathogenesis of OA [33]. An important factor to reduce this load is to increase the strength of the quadriceps muscle [8]. In our study, we obtained significant flexor and extensor muscle strength improvements in patients of all grades in isokinetic group after treatment. Extensor and flexor muscle strength gain persisted in Grade 4 patients with isokinetic exercise at all angular velocities when compared with the isometric exercise at T2. Then, it can be said that isokinetic exercise was more useful for advanced knee OA in terms of muscle strength gain. However, it was not possible to have enough data regarding the long-term effect of exercises on the treatment within a 10-week follow-up period. This situation can be considered a limitation of our study.
Huang et al. compared different muscle strengthening exercises with a control group regarding the treatment of moderate knee OA [23]. The most pain reduction was revealed in isotonic group, while the greatest increase of walking speed and decrease of disability was observed in isokinetic group. The authors reported that more patients in the isokinetic group discontinued treatment than in the other treatment protocols due to knee pain [23]. In our study, none of the patients left the treatment for any reason. Similar to some previous studies, muscle strength gain was found to be slightly superior in patients who received the isokinetic exercise [23, 24, 25, 27, 28]. This situation was considered to be due to how isokinetic exercises allowed the muscle to produce strength throughout the entire range of motion at every point of the movement and at a constant angular velocity. This may be interpreted as an advantage in favour of isokinetic exercise in terms of muscle strength gain. Extensor PM values after isometric exercise didn’t show significant improvement from T0 to T2 in the current study. It was an advantage that isometric exercises were performed at different degrees of joint range of motion, but it could be seen as a disadvantage that isometric exercise protocol only produced muscle strength at the adjusted angles and did not cover the full ROM.
Functional status was evaluated with the WOMAC and the Lequesne index in our study. Using these metrics, significant improvements were observed in both groups at T2. Although, joint stiffness and walking distance scores showed significant improvements in both groups for all grades from T0 to T2, no differences were found between groups. Additionally, Lequesne C and WOMAC C scores in Grade 3 subgroup of isokinetic group were significantly greater than isometric group at T2, which may be caused by the improvement of knee stability through more strengthening of type II muscle fibers during isokinetic exercise.
In a previous study that compare isokinetic exercise programmes, significant increases were observed in thigh circumference after 8 weeks of treatment [25]. In the present study, although 4 weeks of treatment were applied, thigh circumference values increased significantly at the end of treatment in both groups. There was no significant difference between the groups. Also, increased thigh circumference could not be maintained in Grade 4 patients in Group II from T1 to T2.
In another study [24], SF-36 scores were found better in the isotonic group compared to the isokinetic exercise group. In the current study, significant improvements were observed in the SF-36 physical scores in each group from baseline to T2. SF-36 physical scores in Grade 3 and 4 patients in isokinetic group at T2 were significantly greater than isometric group.
Strong correlations were found between reduced ROM of the knee joints and disability [34]. It was reported that limited joint mobility appears to be an important factor of disability in patients with OA [35]. Grade 4 patients in both groups were showed significant improvements from T0 to T2 in terms of ROM values in our study. It was suggested that both exercise types may be beneficial to prevent disability in advanced knee OA.
In our study, patients of all grades showed sinificant improvements in terms of pain and functional status after isometric or isokinetic exercises. On the other hand, Grade 4 patients are also considered candidates for knee arthroplasty in management of knee OA. It was reported before that leg strength and performance of the functional tasks can be improved upon before total knee arthroplasty (TKA), which has the potential to accelerate the rehabilitation process after TKA [36]. Therefore, the use of isokinetic and isometric exercises can be useful in order to reduce symptoms before surgery.
The small sample size, which affects the generalisability of the findings can be a limitation of this study. However, the computation of effect size showed that the isokinetic intervention had large effect on some clinical variables. The second limitation can be the lack of a control group, receiving no intervention. There remains a need for large-scale studies that evaluate the effects of different exercise programmes. We believe that our results will contribute to the development of new treatment programmes for knee OA. Appling isometric exercises with different angles, densities (number of repetitions and sets) and durations may cause changes in the effectiveness of the OA treatments. This study should be followed by further studies with larger sample sizes and different exercise programmes.
Conclusions
Within the limitations of this study, both isokinetic and isometric exercises were effective in the treatment of knee OA of all grades in terms of pain reduction and functional improvements. However, it is also important to note that the isokinetic exercises resulted in longer lasting effects in terms of an increase in the extensor muscle strength at high angular velocities. Grade 4 patients in isometric exercise group showed no significantly muscle strength gain at follow-up.
Footnotes
Conflict of interest
The authors certify that there is no conflict of interest with any financial organisation regarding the material discussed in the manuscript.