
Abstract
BACKGROUND:
An increase in the compensatory action of the quadratus lumborum (QL) during side-lying hip abduction (SHA) can lead to lateral movement impairment of the pelvis.
OBJECTIVE:
To compare the effects of knee flexion (KF) and knee extension (KE) during SHA at abduction angles of 25
METHODS:
Thirty healthy men were recruited and randomly divided into two groups: those with SHA with KF and those with SHA with KE. The subjects performed SHA at three angles of abduction in a random order. Surface electromyography was used to record the muscle activities of the GM and QL.
RESULTS:
The QL activity decreased significantly more in the KE group than in the KF group at each of the three angles of abduction during SHA. The GM/QL activity ratio increased significantly in the KE compared to the KF group. In addition, in the KE group, the onset of the GM activity was significantly earlier than that of the QL activity. On the other hand, in the KF group, the onset of the GM activity occurred later than that of the QL activity.
CONCLUSIONS:
These findings indicate that KE is more effective than KF in selectively activating the GM during SHA by reducing the QL activity and firing the GM earlier than the QL.
Keywords
Introduction
Gluteus medius (GM) controls the abduction of the hip joint and provides lateral dynamic stability to the hip joint and pelvis [1, 2]. GM is the largest abductor muscle of the hip joint and occupies about 60% of the total cross-sectional area of the hip joint abductor muscles [3]. For these reasons, the weakening of GM can contribute to back pain [4] and can result in various musculoskeletal problems such as iliotibial band friction syndrome [5], patellofemoral pain syndrome [6], and instability of ankle [7]. Therefore, strengthening exercises for GM are important for the functional movement of the lower extremities [1, 2].
Side-lying hip abduction (SHA) is principally used to reinforce GM [8, 9]. SHA allows GM to contract effectively; therefore, easy evaluation of the GM strength is possible in this position [10, 11]. While performing SHA, it is difficult to strengthen GM effectively if the compensatory activity of the quadratus lumborum (QL) as a synergist increases instead of GM as an agonist [12]. The increase in compensatory activity of QL can lead to lateral pelvic rotation, resulting in lateral instability and impaired movement of the pelvis [13]. Therefore, it is preferable to increase the muscle activity of GM while decreasing the muscle activity of QL [14, 15, 16].
Changes to the angle of the hip joint in the sagittal and horizontal planes affect the contraction force of the GM. Lee et al. [17] reported that medial rotation of the hip joint during SHA results in the increase of GM activity by 33% compared with the neutrality of the hip joint in women with weak GM. In addition, Willcox and Burden [18] reported that the increase in hip flexion during “clam” exercises leads to an increase in GM activity.
Moreover, bending of the knee affects the movement of the hip joint due to biarticular muscles connecting the hip and knee joints [19, 20]. Tensor fasciae latae and sartorius are abductors of the hip joint and are biarticular muscles crossing the knee joint [21]. Changes in the length of these muscles caused by knee flexion (KF) and knee extension (KE) can affect the abduction moment of the hip joint [20]. However, there has been no study of the effect of KF during SHA on the selective activity of the GM and QL.
Page et al. [22] mentioned that the GM and tensor fasciae latae are the first active muscles during SHA. If the GM is weakened or inhibited, the tensor fasciae latae and QL contract first as compensatory action. Chaitow [23] described that the muscle recruitment sequence during SHA follows this order: GM first and then QL. Moreover, he explained that the QL is overactive if it contracts before or simultaneously with GM. However, studies on the onset time of GM and QL during SHA are still insufficient; furthermore, how KF affects the onset time of GM and QL during SHA has not been explored yet.
Therefore, the main purpose of this study was to compare the effects of KF and KE during SHA on the muscle activities of GM and QL as well as GM/QL activity ratio. Another aim of this research was to identify the effect of KF during SHA on the onset time of GM and QL. It was hypothesized that there would be significant differences in the muscle activities, activity ratio, and onset time of GM and QL depending on the presence of KF vs. KE during SHA.
Methods
Subjects
The sample size was calculated using G-power program (ver. 3.1.2; Franz Faul, University of Kiel, Kiel, Germany). A pilot study was conducted with 10 subjects (five with KF and five with KE), and the necessary sample size of at least seven subjects per group was determined (significance level of 0.05, power of 0.9, and effect size of 2.07). The effect size was calculated from the mean and standard deviation of the pilot study. Thirty healthy men in their 20s to 30s participated in the experiment (Table 1). Participants were randomly divided into two groups using the random-number function in Microsoft Excel: SHA with KF (90
General characteristics of subject
General characteristics of subject
Values are presented as mean
Candidates with back, pelvic or leg pain within the last three months, those with experience of orthopedic or neurosurgical surgery on low back, pelvis, hip joint and legs, and those who could not perform hip joint abduction normally due to shortened hip flexor muscles were excluded from the experiment. We provided all participants with a description of the purpose and methods of the study, and written consent was obtained from all subjects. This study was approved by the Daegu University’s Institutional Review Board (No: 1040621-201711-HR-025-002).
Electromyography (EMG) measurements of the activity of GM and QL during hip abduction were collected using wireless surface EMG. A disposable single surface electrode with Ag/Agcl material was used and patients’ hair was removed with a shaver to minimize skin resistance. The skin was rubbed 2–3 times using fine sandpaper to remove the corneum. Then, oils on the skin surface were removed with an alcohol swab. Two electrodes were placed approximately 20 mm apart in the direction of the muscle fibers. For the GM, electrodes were placed directly superior to the greater trochanter of the femur, one-third of the distance between the iliac crest and the greater trochanter of the femur [14, 16]. For the QL, electrodes were placed 4 cm lateral from the vertebral ridge of the belly of the erector spinae and at a slightly oblique angle at half the distance between the 12
Myo-Research Master Edition 1.06 XP software was used to analyze the EMG data. The sampling rate was 1000 Hz. A digital band-pass filter, which filtered the raw signals, was between 20 and 400 Hz and removed 60 Hz noise using a notch filter. Root-mean-square values were calculated with a moving window of 150 ms. Collected signals were normalized with the % maximal voluntary isometric contraction (% MVIC).
MVIC measurements of GM and QL were measured using Kendall’s method [10]. MVIC measurements were performed three times for five seconds. The average value was obtained by calculating the mean value for each of the middle three seconds, excluding the first and last seconds of the five-second measurements. To calculate the muscle activity ratio of GM/QL, the normalized value of GM activity was divided by the normalized value of QL activity [17]. A one-minute break was allowed between each contraction to avoid muscle fatigue.
The baseline EMG was calculated by averaging the EMG activity for five seconds in the initial resting position. The onset of activity of each muscle was defined when the EMG amplitude exceeded two standard deviations of the baseline level for a minimum of 50 ms [24, 25]. The relative onset difference between the GM and QL was calculated by the following equation:
Therefore, a negative value indicates that the GM fired before the QL. When the QL fired earlier than the GM, the relative onset difference was a positive value [24, 26].
Experimental procedures
To identify differences between groups at various abduction angles, the activity of each muscle was measured at abduction angles of 25
The subjects placed the non-dominant leg on the treatment table and were laid sideways in a straight line. Using a goniometer and a target bar, the angles of hip abduction of subjects were set. A guide bar was installed in order to ensure hip abduction under the same conditions by preventing flexion and extension of the hip joint. Measurements were invalidated when the leg touched the guide bar. In addition, an inclinometer was attached to the abducted leg to maintain neutrality of hip joint in the transverse plane; during SHA, the inspector supervised the angle of the inclinometer to remain at zero. At each angle, subjects performed hip joint abduction and kept their leg touching the target bar for five seconds (Fig. 1). The EMG signal collected for the middle three seconds, excluding the first and last seconds of the five-second measurements. The average value over the three repetitions was used for EMG activity analysis.
Side-lying hip abduction with knee 90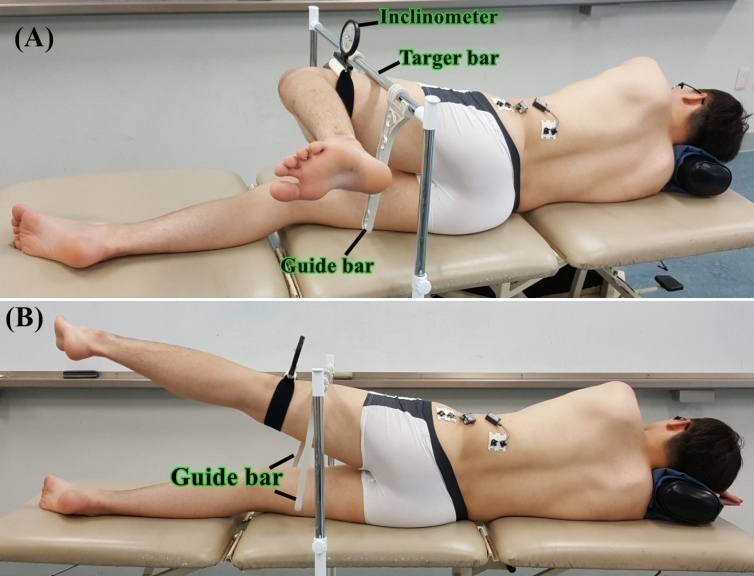
Comparison of muscle activity of knee flexion (KF) group and knee extension (KE) group at three abduction angles during side-lying hip abduction (SHA)
Values are presented as mean
Statistical analysis was performed using the PASW Statistics 18 software (SPSS Inc, Chicago, IL, USA). All data were subjected to a normality test using the Shapiro-Wilk test. In order to compare EMG activity between the two groups, the two-way repeated measures ANOVA test was used and the significance level was set to 0.05. As a post-hoc test, the independent
Results
Comparison of muscle activity between groups in three angles
Measured data concerning the EMG activity of each muscle in both groups are summarized in Table 2. There were no significant group-by-abduction angle interactions for the activity of GM (
Comparison for EMG onset between groups during SHA
The relative onset was significantly faster in the KE group (mean
The relative onset difference between the gluteus medius (GM) and quadratus lumborum (QL). Relative onset difference 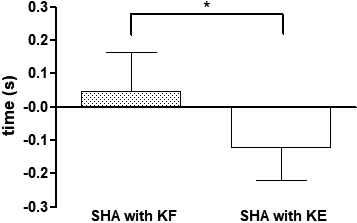
It is preferable to increase the activity of GM while decreasing the activity of QL during SHA because increasing the action of QL can cause elevation or lateral rotation of the pelvis [13, 14, 15, 17]. In this study, the QL activity of the KE group decreased significantly more than that of the KF group at angles of 25
The relative increase of QL activity in the KF group can be explained by the following mechanism. Flexion of the knee can increase the anterior tilt of the pelvis in the sagittal plane [24, 28]. Moreover, during SHA, flexion of the knee can transfer the center of gravity of the torso backwards by moving the weight of the lower leg in that direction. Therefore, these factors are considered to increase the lumbo-pelvic perturbation, thereby increasing the activity of QL. These results are similar to that of previous studies in which augmented torso stability during SHA decreased QL activity [14, 15].
The lateral part of QL originates on the posterior iliac crest and inserts into the 12th rib without attachment to any vertebrae. It primarily produces a lateral bending movement, whereas the medial part of QL provides segmental stability by attaching to the transverse processes of the lumbar spine [23, 29]. When one side of QL contracts, the pelvis on the ipsilateral side is rotated upwards [23]. The increase in QL activity during SHA laterally rotates or elevates the pelvis more than stabilizing the lumbar area [22]. Considering the anatomical structure and function of QL, it is expected that, in the KF group, increased QL action would increase the lateral tilt of the pelvis. Although we did not measure kinematic information in this study, the grounds for this prediction are based on the study results of Cynn et al. [14], in which augmented torso stability decreased QL activity and pelvic lateral tilt during SHA.
Another finding of the present study was that the relative onset difference between GM and QL in the KE group was negative, meaning that the GM was firing before QL. Conversely, the relative onset difference between GM and QL in the KF group was positive, meaning that the QL was firing before GM. Chiatow [23] and Page et al. [22] reported that GM and tensor fasciae latae were the first firing muscles during SHA, which is consistent with our results in the KE group. As described earlier, flexion of the knee during SHA can affect hip and pelvic neutrality. The QL seems to be activated before the GM in order to prevent the pelvis from rotating in the horizontal plane during SHA. Therefore, performing SHA with KF is a less effective method because it leads to earlier onset of QL activity.
This is the first study comparing the effects of KF and KE during SHA. Many studies on the effects of KF during prone hip extension have been conducted, and it is known that KF, more than KE, facilitates the activity and early onset of gluteus maximus [30, 31]. However, in this study KF during SHA was found to have no improvement on muscle activity and onset of GM. We believe that our study is of clinical value as it suggests the criteria and basis of the knee position necessary to achieve selective activation of the GM while performing SHA.
This study has several limitations. First, we could not confirm that KF increases the action of hip internal rotators during SHA, as we did not measure the EMG activity of tensor fasciae latae. Second, we could not confirm whether the lateral movement of the pelvis actually occurred as we did not measure kinematic data. In future studies, it is necessary to investigate how KF affects the activity of tensor fasciae latae and the motion of the pelvis during SHA. Third, because the subjects were healthy men, it is difficult to generalize to other population groups.
Conclusion
We suggest that KE is more effective than KF for selective activation of the GM during SHA by reducing the QL activity and firing the GM earlier than the QL. Based on our analysis, this study points out to a standard position during SHA.
Author contributions
CONCEPTION: Dong-Woo Kim.
PERFORMANCE OF WORK: Dong-Woo Kim.
INTERPRETATION OR ANALYSIS OF DATA: Dong-Woo Kim and Han-Kyu Park.
PREPARATION OF THE MANUSCRIPT: Dong-Woo Kim and Yang-Jin Lee.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Han-Kyu Park.
SUPERVISION: Yang-Jin Lee.
Ethical considerations
IRB number: 1040621-201711-HR-025-002.
Research date: December, 21, 2017 December, 20, 2018.
Funding
None.
Footnotes
Acknowledgments
None.
Conflict of interest
The authors declare no conflict of interest.