
Abstract
BACKGROUND:
Adequate participant’s fixation affects measurement accuracy and performance of isokinetic exercise.
OBJECTIVE:
To examine the effects of different fixation methods and contraction modes on the kinetics and 3D kinematics of prone isokinetic knee flexor tests.
METHODS:
Fourteen healthy male participants performed maximal unilateral concentric and eccentric knee flexion movements with minimal (hand grips), moderate (grips, hip strap) and maximal (grips, thigh and hip strap, hip wedges, shoulder pads) fixation at 30
RESULTS:
Concentric and eccentric peak moments were highest at minimal and maximal fixation, whereas contractional work peaked at minimal fixation. Axis alignment was best at moderate fixation. Initial axis alignment caused an average antero-cranial shift (2.0 and 0.1 cm) as well as mean roll and yaw angle tilts of
CONCLUSIONS:
Depending on their purpose, prone isokinetic knee flexor tests or training sessions should be conducted with minimal (maximal force production) or moderate (axis alignment) fixation. When interpreting and comparing isokinetic results, the examined kinematic and kinetic effects of different fixation methods should be taken into account.
Introduction
Isokinetic testing has gained widespread interest in clinical and laboratory context. Although a variety of test settings are recommended, relatively little research about their measurement accuracy [1, 2, 3] is available. Arampatzis et al. [1] investigated isokinetic plantar-dorsiflexion movements. Although the foot and shank were maximally fixed, considerable axis misalignment led to a 5–9% difference between measured and resultant moments. Alt et al. [2] evaluated the effects of fixation, contraction mode and angular velocity on the kinetics and 3D kinematics of supine knee extensions. Maximal fixation improved axis alignment, while the moment output was reduced. The same research group found considerable deviations between the pre-selected range of motion and angular velocity and the actual kinematic values of concentric knee extensor and eccentric knee flexor exercise [3] when hand grips were used as stabilisation.
Due to the anatomy of human joints a perfect axis alignment between the axis of the testing device and the knee joint is impossible. However, the aim of isokinetic tests should be a best possible reduction of this intrinsic axis misalignment. A simultaneous kinematic analysis of isokinetic tests can quantify the respective differences of axes orientation. Prone isokinetic knee flexor tests are especially used to measure the strength capabilities of the hamstrings in order to assess the injury risk for a hamstring strain injury or an anterior cruciate ligament tear [4]. It is well-known that hamstring peak moments increase when hip flexion is augmented because of the greater moment arm at the hip joint and the more lengthened muscle-tendon unit [5, 6, 7, 8]. Alt et al. proved that an eccentric knee flexor test at 150
Consequently, the aim of the present study was to examine the effects of different fixation methods and contraction modes on the kinetics and 3D kinematics of prone isokinetic knee flexor tests. The hypotheses were:
Peak moments and contractional work would increase with higher hip flexion. Maximal fixation would improve the alignment between transepicondylar and dynamometer axis. Eccentric knee flexion movements would result in a smaller range of motion and a reduced mean angular velocity compared to concentric exercise.
Awareness of these kinetic and kinematic effects is important for scientists and physiotherapists conducting maximal strength tests and/or rehabilitation training. It assists in ensuring a functional loading of the involved biological tissues and a reasonable interpretation of collected data.
Participants
Fourteen healthy male participants (mean
Procedures
All participants performed two sessions (familiarisation and testing) which followed the identical procedures. The sessions were separated by 72–96 h. After determining their mass, the participants individually warmed up (jogging, dynamic stretching) for ten minutes. This general warm-up was followed by the participant’s positioning on the dynamometer (IsoMed 2000, D&R Ferstl GmbH, Hemau, Germany). The participants were asked to lie prone, with shoes off to reduce acceleration errors, with a 0
The individual settings of each participant were stored by the manufacturer’s computer software IsoMed analyze V.2.0 to guarantee an accurate repositioning. Afterwards, a rigid three-dimensional calibration frame (LxWxH: 40
Minimal (top), moderate (middle) and maximal (bottom) fixation during prone isokinetic knee flexor tests. Eight retro-reflective markers were used to compute knee and hip kinematics.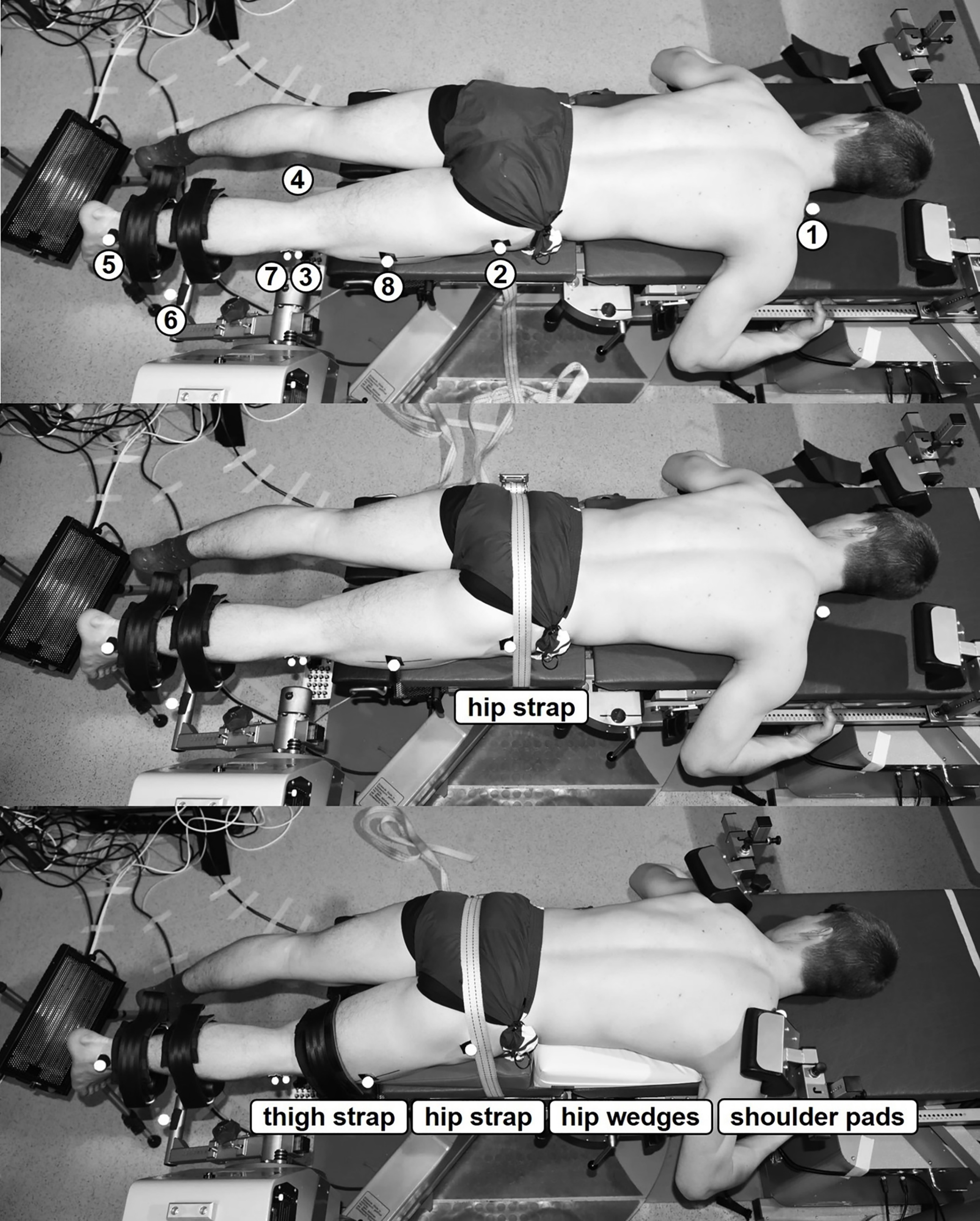
Functional movement planes of the calibrated volume (LxWxH: 180 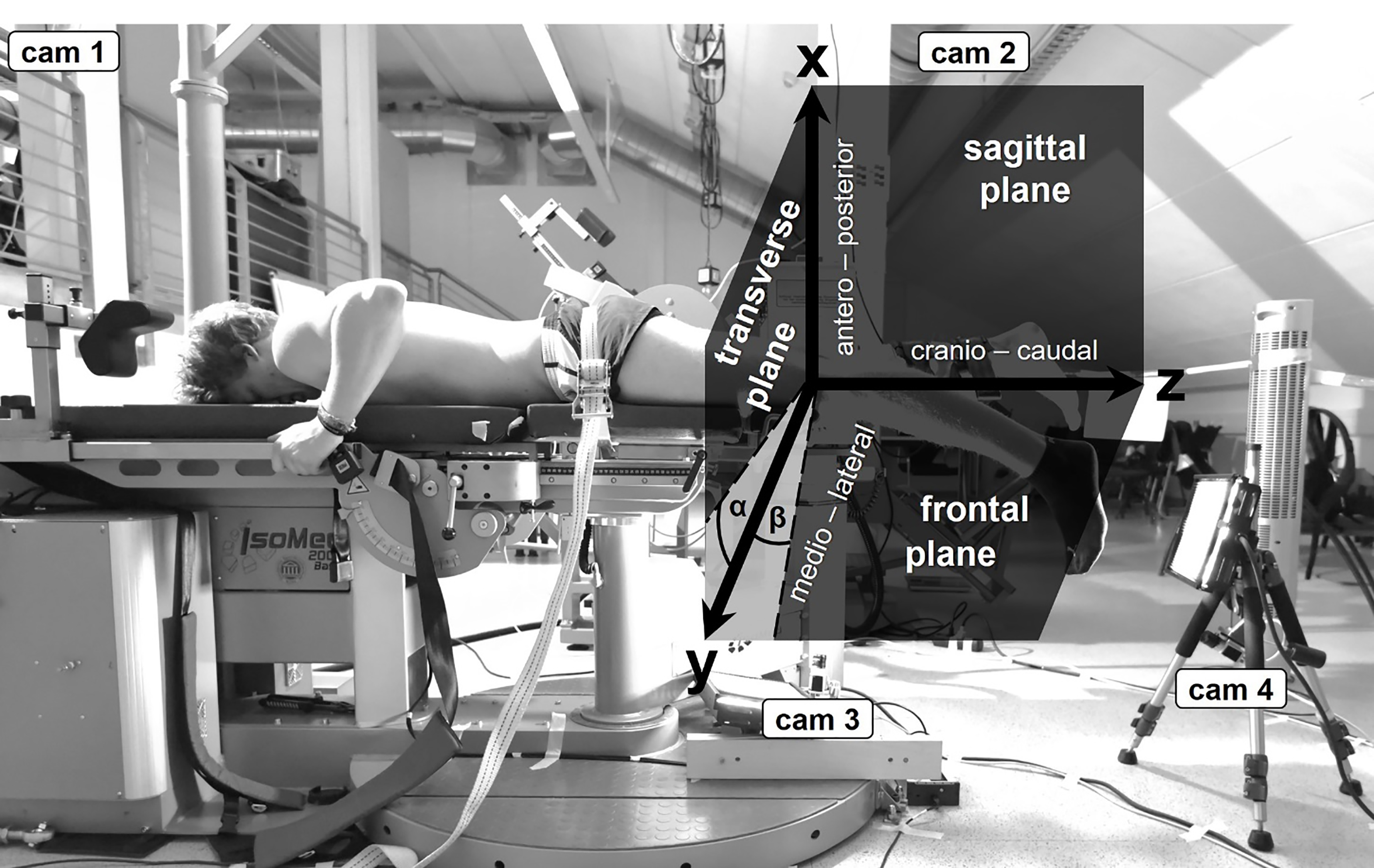
After removing both calibration frames, a double shin pad for unilateral knee extension was attached to the motor-driven axis, whereas its distal part was fastened by straps approximately 2–3 cm proximal to the lateral malleolus. A static gravity correction in horizontal lever arm position and at a relaxed muscular state was executed by the integrated software. Each participant had to perform concentric and eccentric knee flexion movements at three fixation methods: minimal (hand grips), moderate (grips, hip strap) and maximal (grips, thigh and hip strap, hip wedges, shoulder pads) (Fig. 1). To ensure the highest reproducibility the fixation was applied by the same examiner. The order of the fixation condition was randomly assigned. After each fixation was applied the participants performed 15 submaximal (
Mean postero-cranial displacement of the lateral femoral epicondyle in relation to the dynamometer axis (dashed cross) obtained from concentric (left) and eccentric (right) knee flexion movements at 30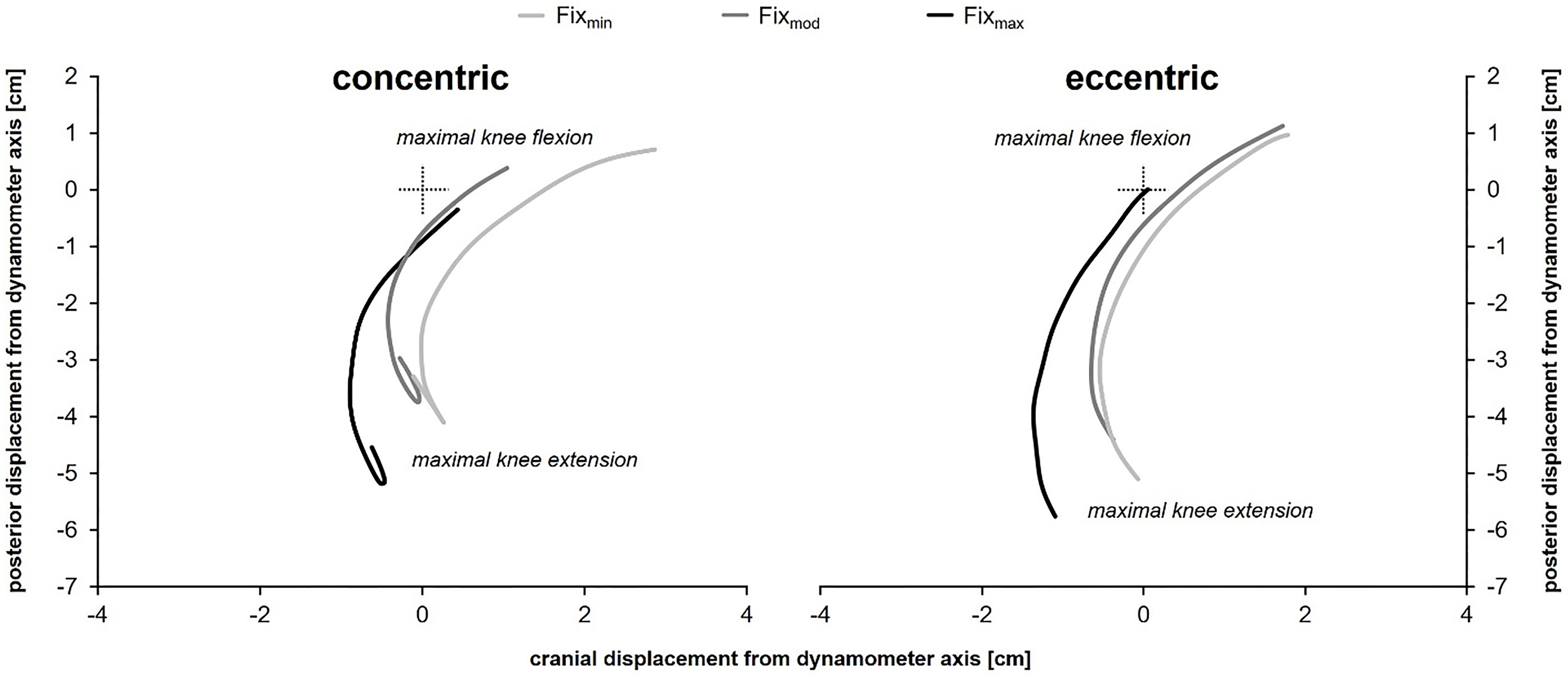
Kinetic raw data were recorded at a sampling rate of 200 Hz (IsoMed analyze V.2.0, D&R Ferstl GmbH, Hemau, Germany). Kinematic data were captured with 100 Hz (Basler A602fc-2, Basler AG, Ahrensburg, Germany) and processed in Vicon Motus (V9.2, VICON TM, Oxford, UK). Kinetic and kinematic data were synchronized (TEMPLO 8.2.358, Contemplas, Kempten, Germany). Roll (
Kinetic raw data were stored as ASCII files. By the aid of a custom software written in C++, a recursive 5
Kolmogorov-Smirnov (
The effect size of the ANOVA was assessed by the partial eta-squared (
Results
Table 1 contains all kinetic and kinematic results gathered from concentric and eccentric prone knee flexion movements with minimal, moderate and maximal fixation. Significant effects are highlighted by grey accentuation.
Kinetic results
Moderate fixation led to significant reductions of peak moments (PM) (
Kinematic results
Compared to minimal and moderate fixation, isokinetically determined angles of concentric and eccentric peak moments (APM
Effects of participant’s fixation (fix) and contraction mode (contrac) on kinetic and kinematic parameters obtained from concentric (con) and eccentric (ecc) prone isokinetic knee flexor tests
Effects of participant’s fixation (fix) and contraction mode (contrac) on kinetic and kinematic parameters obtained from concentric (con) and eccentric (ecc) prone isokinetic knee flexor tests
Concerning the kinematic range of motion (ROM
Figure 3 shows the postero-cranial displacement of the lateral femoral epicondyle in relation to the dynamometer axis (coordinate origin). Initial axis misalignment resulted in an average antero-cranial shift (2.0 and 0.1 cm) during maximal contractions. Maximal fixation led to a significantly increased anterior trajectory centre shift (tcsx) (1.04
Mean roll (top) and yaw angle (bottom) characteristics of the transepicondylar axis in relation to the dynamometer axis (zero line) obtained from concentric (left) and eccentric (right) knee flexor tests at 30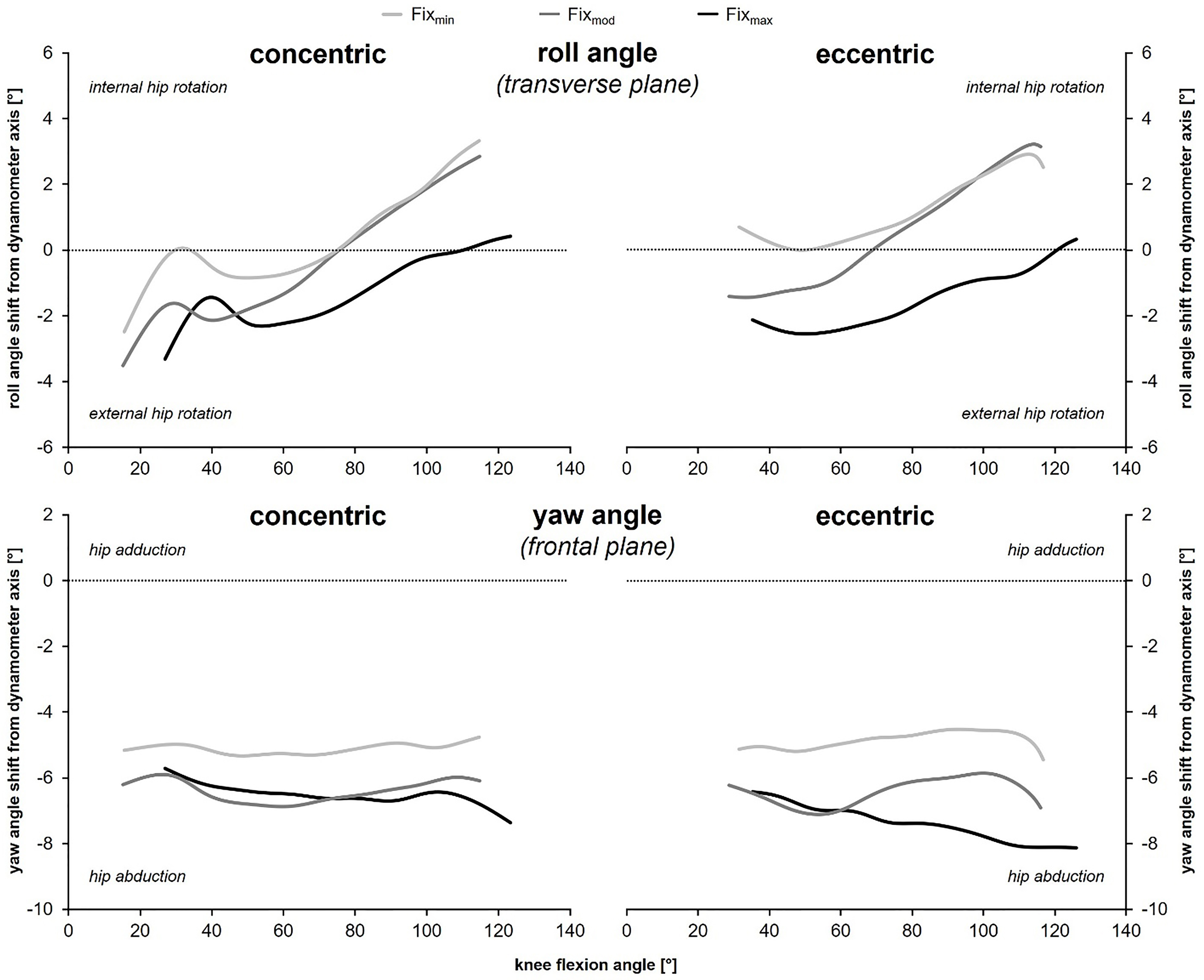
Figure 4 illustrates the roll (top) and yaw angle (bottom) histories of the transepicondylar axis in relation to the dynamometer axis (zero line). During concentric and eccentric knee flexion movements, there was an average misalignment of 0.1
The aim of the present study was to examine the effects of different fixation methods and contraction modes on the kinetics and 3D kinematics obtained from prone isokinetic knee flexor tests. The subsequent discussion is arranged according to the three hypotheses.
Peak moments and contractional work would increase with higher hip flexion
Peak moments and contractional work were highest at minimal fixation when maximal hip flexion angles demonstrated mean values of 15
Due to the above reasons, the first hypothesis can be partially confirmed for peak moments, but not for contractional work.
Advantages of minimal, moderate and maximal participant’s fixation as well as unaffected parameters concerning kinetic and kinematic parameters obtained from prone isokinetic knee flexor tests
Advantages of minimal, moderate and maximal participant’s fixation as well as unaffected parameters concerning kinetic and kinematic parameters obtained from prone isokinetic knee flexor tests
ROM
Maximal and moderate fixation induced the shortest sagittal trajectory length (Table 1). However, maximal fixation caused a mean antero-cranial shift of the trajectory centre (2.8 cm and
Roll and yaw angles of concentric movements were unaffected by fixation method (Table 1). Eccentric exercise showed lowest values at minimal fixation (Fig. 4). These findings support the assumption that maximal fixation altered the movement patterns of the knee joint axis and its surrounding muscles [6, 13]. The present results of prone knee flexion movements can be well compared with previous research about supine concentric and eccentric knee extensions [2]. The average misalignment of 2.0 and 0.1 cm in antero-caudal direction (0.8 and 2.4 cm), mean roll and yaw angle tilts of
Thus, the second hypothesis has to be rejected for all three movement planes. Best axis alignment was achieved by moderate fixation which prevented hip motion by a strap.
Eccentric knee flexion movements would result in a smaller range of motion and a reduced mean angular velocity compared to concentric exercise
It is well-established that under the same angular velocity, the peak moments produced during eccentric efforts are higher than their concentric counterparts [5, 6, 7, 8]. The present results demonstrated an expected difference of 26%–31% (Table 1). This enhanced muscular strength might have led to greater material deformation of the lounger’s edge (directly adjacent to the knee joint axis, see Figs 1 and 2) especially near full knee extension inducing an anterior shift of the knee joint axis (Fig. 2). Therefore, minimal knee flexion angles (
Thus, the third hypothesis can be confirmed underlining the importance of controlling joint kinematics during isokinetic tests.
Synopsis
Table 2 enumerates the advantages of minimal, moderate and maximal participant’s fixation as well as the unaffected parameters. As previously mentioned, some of the detected differences – especially concerning sagittal axis alignment at maximal fixation – might be induced by inappropriate initial alignment which likely befalls each examiner to a certain extent. The average deviations – an antero-cranial shift of 2.0 and 0.1 cm as well as mean roll and yaw angle tilts of 0.1
Depending on their purpose, prone isokinetic knee flexor tests or training sessions should be conducted with minimal (maximal force production) or moderate (axis alignment) fixation. Maximal fixation showed no essential advantages over the other fixation methods which does not justify the additional time requirement for appropriate positioning and fixation of the shoulder pads, the hip wedges as well as the hip and thigh strap (Fig. 1). Apart from the fixation method used, the examiner must always check if the patient/athlete executes unwanted evasive movements which might compromise measurement accuracy. Therefore, good instructions as well as a separate and properly conducted familiarisation session is crucial for appropriate standardisation of testing procedures and reliable data acquisition [10]. If muscular strength of the hands, arm and trunk muscles is not sufficient to ensure an adequate internal fixation by hand grips (e.g. among females), additional external fixation will be mandatory [13].
Limitations
The present study incorporated three major constraints. First, the material deformation-induced anterior displacement of the lateral femoral epicondyle could have been reduced if the plinth’s padding would have been more rigid and/or a tough covering of
Perspectives
It is well-established that hamstring peak moments are considerably increased (
Conclusions
The presented study provides first empirical insights into the effects of different fixation methods and contraction modes on the kinetics and 3D kinematics of prone isokinetic knee flexor tests. After weighing the advantages and disadvantages of minimal, moderate and maximal fixation, we recommend that prone isokinetic knee flexor tests or training sessions should be performed with minimal (maximal force production) or moderate (axis alignment) fixation, depending on their purpose. Maximal fixation showed no exclusive advantages.
Peak moments were greater when fixation permitted higher hip flexion (Fix
Due to the complex anatomical structure of the knee joint, a perfect three-dimensional alignment to a fixed dynamometer hinge axis is not possible. However, every effort should be made to increase measuring accuracy by reducing spatial expansion and systematic axis shifts during isokinetic movements.
The knowledge of the presented kinetic and kinematic relations may be important for scientists as well as physiotherapists to warrant a functional loading on the involved biological tissues and to put test and training results into perspective.
Footnotes
Acknowledgments
The authors would like to thank all subjects who volunteered to participate in this study and demonstrated great motivation and commitment.
Conflict of interest
The present study was not funded and there was no conflict of interest.