
Abstract
BACKGROUND:
There is no information about the reliability of a comprehensive way to assess muscle tone that contains the different dimensions that define or could influence it in the ankle plantar flexors.
OBJECTIVE:
To evaluate the relative and absolute test-retest intra-day and inter-day reliability of a comprehensive protocol for the assessment of muscle tone responsiveness of the ankle plantar flexors.
METHODS:
Twenty healthy volunteers completed the study. It was performed a methodological study protocol (SPIRITT). Assessments included passive resistive torque-to-ankle dorsiflexion at slow (10
RESULTS:
Passive resistive-torque using isokinetic showed better reliability (CV
CONCLUSION:
The comprehensive protocol of muscle tone assessment showed very good reliability. The protocol established provides a reliable tool to assess and characterise muscle status and the effect of therapeutic interventions.
Introduction
Muscle tone has been defined as “the state of activity or tension of a muscle beyond that related to its physical properties” [1]. Furthermore, clinically, muscle tone is accepted as the resistance felt to externally imposed movements during a state of voluntary relaxation [2], resulting from the interaction of the intrinsic viscoelastic muscle properties (also called “passive tone”, “mechanical”, “non-reflex” or “EMG-silent” component) and neurogenic factors that are activated by stimuli, represented mainly as the tonic stretch reflex, also called “active tone”, “reflex tone” or “neurogenic tone” [3, 4].
Muscle tone is usually quantified in subjects with spasticity and other muscle tone disorders using isokinetic dynamometry and surface Electromyography (sEMG) [5]. Furthermore, these techniques are also considered a valid method to measure muscle tone in non-injured subjects [6]. However, only specific mechanical muscle properties, such as stiffness, are usually assessed in non-injured subjects. Considering this, both the whole muscle tone concept and specific stiffness are important aspects to measure in healthy subjects when studying neuromuscular physiology, muscle performance, or action mechanisms of several therapeutic interventions. However, there are no validated protocols and few reliability studies that specifically measure muscle tone or any of its components in non-injured subjects [7].
The potential usefulness of sEMG has been suggested as a complementary method to detect and quantify the reflex muscular response to passive mobilisation [3, 5, 8]. Although there have been some techniques described to measure this neuromuscular activity, which is different between passive mobilisation and reflex stiffness [3, 8], there are no reliability studies to validate these protocols. Furthermore, the sEMG technique reveals limitations in reliability and sensitivity to electrode location and type of muscle contraction [9, 10]. Muscle extensibility has been highlighted as an important characteristic within mechanical muscle properties [11, 12]. However, the implication of muscle extensibility on muscle tone or performance needs to be clarified [12, 13, 14]. Muscle extensibility is usually measured as the passive range of motion during stretching [11, 15]. However, the endpoint of the stretching depends on the protocol used, possibly influencing the reliability of the measure. Objective protocols to quantify muscle extensibility are necessary to validate the responsiveness to the therapeutic approach and to determine the relations between passive muscle properties and muscle function. Muscular performance has also been related to muscle tone and mechanical muscle properties [12]. The reliability of dynamometer devices in the assessment of the strength has been evaluated in several studies [16, 17, 18] and the focus has largely been on the knee joint [19, 20]. At the ankle joint, Webber et al. analysed the relative and absolute intra-rater reliability of different types of contractions (isometric, isotonic and isokinetic) for ankle dorsiflexion and plantarflexion, finding minimal detectable change scores [18].
There is no information about the reliability of a comprehensive way to assess muscle tone that contains the different dimensions that define or could influence it (resistance to passive movement at different velocities, electromyographic activity, strength and extensibility) in the ankle plantarflexors. The idea of having a valid and a reliable protocol to quantify non-injured muscle tone could be useful in the field of sports and performance, and also for clinical purposes, to better understand muscle tone disorders and to study experimental treatments in healthy subjects. Therefore, the purpose of this study was to evaluate the relative and absolute test-retest intra-day and inter-day reliability of a proposed protocol that included passive resistive torque at 10 and 180
Method
Subjects
Twenty healthy volunteers (12 males and 8 females) with a mean age of 26.6
Procedures
A repeated measures design was carried out to determine the intra-day and inter-day reliability. A week before the testing sessions commenced, the participants were familiarised with the testing procedures by simulating the testing conditions that were carried out during the experimental sessions. In addition, in order to ascertain the participants’ dominant limb, during this familiarisation session, all of the participants were required to undertake three tests: 1) jumping on one leg, 2) kicking a ball, and 3) climbing onto a stool with one leg according to [22] protocol. The limb used to do at least 2/3 tests was considered the dominant and the tests were carried out with this lower limb.
After the familiarisation protocol, each participant undertook the testing procedure on three different occasions, with a one-hour (intra-day reliability) and a one-week (inter-day reliability) rest interval between testing sessions. The experimental conditions (room temperature at 25
A: Schematic representation of the experimental procedures for passive resistive torque and muscle extensibility measurement. Subjects are seated with the hip placed at a 90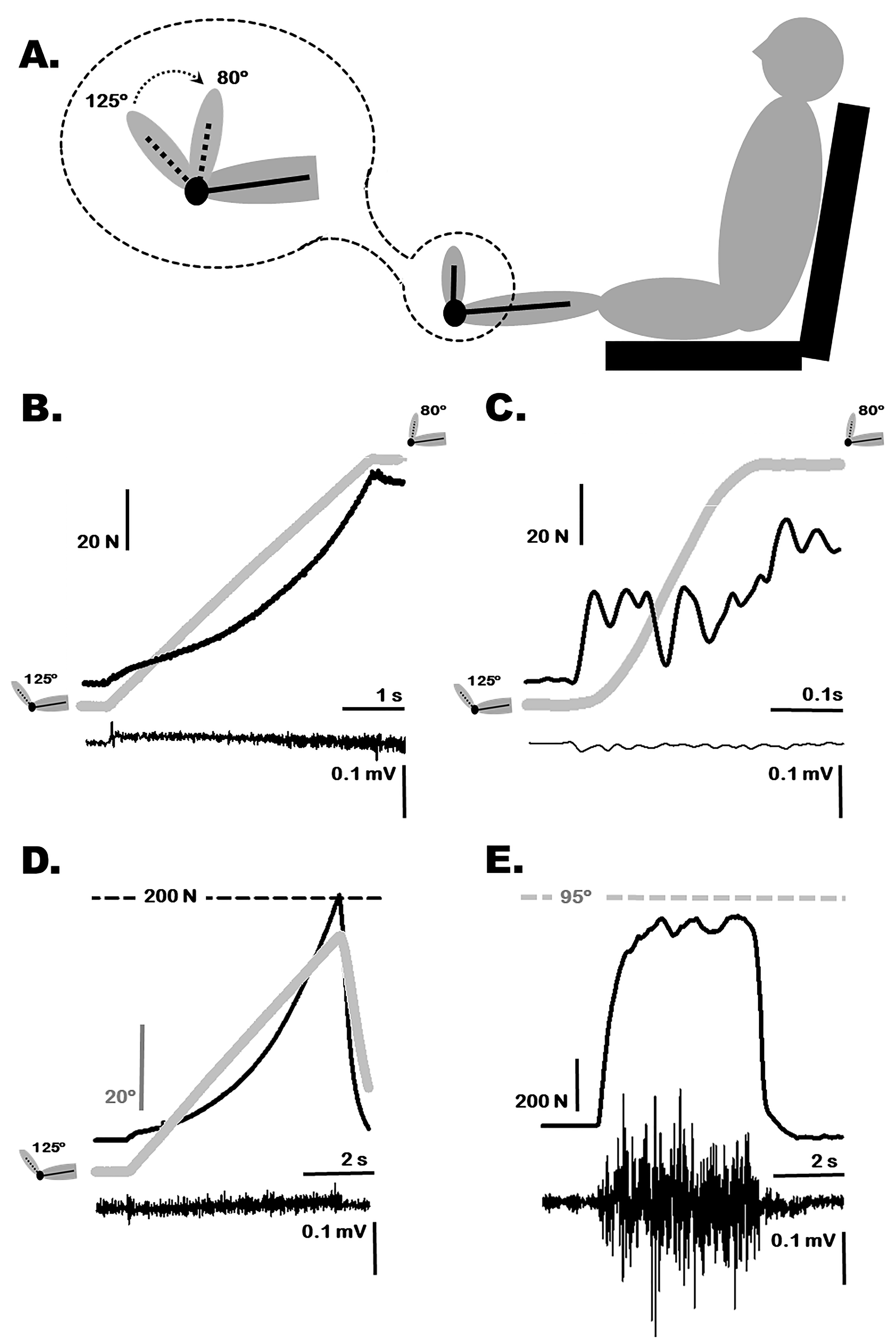
Initially, all volunteers were seated with the hip placed at a 90
Measurement of passive resistive torque
Triceps Surae passive resistive torque was quantified by measuring the resistance to passive ankle dorsiflexion at slow (10
Measurement of gastrocnemius muscle extensibility
Muscle extensibility has been considered as the ability of a muscle to extend to a predetermined endpoint [11]. To ensure objective and independent quantification of the passive range of motion (PROM) for ankle dorsiflexion, the Kin-Com dynamometer was employed to perform mobilisation at a constant velocity at 10
Maximal voluntary isometric force (MVIF)
The subject’s foot was fixed at 5
Data recording and analysis
Isokinetic device outputs were connected to an analogical-digital converter (Micro 1401-3; Cambridge Electronic Devices, CED, Cambridge, UK) and digitally monitored and further analyzed using the Spike 2 software package (version 5.03, Cambridge Electronic Devices, CED, Cambridge, UK). Quantification of ankle dorsiflexion peak force (N), measured as a passive resistive force at both slow and fast velocities, was registered to measure maximal resistance of the Triceps Surae muscles. The resistance integral (N.s), measured during mobilisation, was analysed to represent the energy accumulated in the stretched muscle. A mean of five repetitions for each measure was made for the 10
Surface EMG was recorded at a gain of 1 KHz with an in-built filter bandwidth between 20–450 Hz. Electromyographic data were collected via the analogical-digital converter to be synchronized with the mechanical parameters obtained from the isokinetic device. Further EMG offline analysis was made with the Spike 2 software. GM EMG data were obtained during the maximal isometric plantarflexion activation. The GM EMG response was registered during the slow and fast passive dorsiflexion mobilisations. EMG data were rectified, averaged and integrated for each contraction. EMG activity recorded during maximal isometric plantarflexion is presented in units of mV.ms. GM EMG activity recorded during slow and fast passive ankle dorsiflexion was normalised as a percentage of the maximal isometric plantarflexion activation level.
Statistical analysis
SPSS v. 17.0 software (SPSS Inc., USA) was used to perform the statistical calculations. The distributions of datasets were checked using the Kolmogorov-Smirnov test, which demonstrated that all data had a normal distribution (
The test-retest reliability for each variable was calculated with pairs of trials (set 2–set 1 and set 3–set 1) [26]. In addition, the following establishments of reproducibility in human performance were explored [26, 27]: i) A paired sample
Results
Paired
Table 2 shows descriptive statistics (mean values
Descriptive statistics for each variable in the extensibility test and in the MVIF test are shown in Table 2. The intra-day and inter-day ICC for PROM in the gastrocnemius muscle extensibility test were high (0.97 and 0.90, respectively). PROM showed the best CV
| Variable | Descriptive statistic (mean |
Intra and inter-day reliability (mean and 95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|
| Set 1 | Set 2 | Set 3 | Mean difference |
|
ICC | CV |
||
| Gastrocnemius muscle extensibility | ||||||||
| Passive range of motion ( |
158.4 |
159.1 |
158.7 |
Intra-day (2-1) | 0.7 |
0.162 | 0.97 (0.91 to 0.99) | 0.9 (0.7 to 1.3) |
| Inter-day (3-1) | 0.3 |
0.729 | 0.90 (0.74 to 0.96) | 1.5 (1.2 to 2.3) | ||||
| Maximal voluntary isometric force | ||||||||
| Peak plantarflexion force (N) | 607.7 |
596.9 |
642.2 |
Intra-day (2-1) |
|
0.500 | 0.94 (0.86 to 0.98) | 11.5 (8.6 to 17.2) |
| Inter-day (3-1) | 34.5 |
0.115 | 0.92 (0.80 to 0.97) | 10.9 (8.2 to 16.4) | ||||
| Integrated GM EMG (mv*ms) | 0.21 |
0.19 |
0.20 |
Intra-day (2-1) |
|
0.128 | 0.90 (0.77 to 0.96) | 20.8 (15.5 to 31.8) |
| Inter-day (3-1) |
|
0.680 | 0.82 (0.59 to 0.93) | 33.2 (24.4 to 52) | ||||
Descriptive values, inference statistic and absolute and relative reliability statistics among intra-day and inter-day sessions in passive range of motion and maximal voluntary isometric force tests (data are mean
This study was conducted to establish intra-day and inter-day reliability scores for a comprehensive method to assess muscle tone of the ankle plantar flexors. We have addressed, in an objective way, the main dimensions of muscle tone (strength, passive resistive force to slow-and-fast velocities, muscle extensibility and EMG activity). Although the reliability of these isolated measures has been previously investigated to assess passive muscle properties [7, 30], there are no standardised protocols that include the whole assessment of muscle tone, which is used often in the clinical context. The results of this study demonstrated that the parameters registered with the isokinetic device in all of the variables were associated with good relative intra-day reliability (all ICCs
Several methods for the measurement of musculotendinous stiffness have been used, such as hopping and oscillation tests [30], myotonometers [31], custom built devices [32] or manual dynamometers [33]. The application of a constant velocity stretching performed by a commercialised isokinetic dynamometer has been also used in other studies in healthy subjects [34, 35, 36] and in subjects with muscle tone disorders [23, 24]. However, there is a lack of consensus for the use of a standardised protocol, not only to assess muscle stiffness, but also to evaluate muscle efferent innervation and other mechanical passive properties that may characterise muscle tone [4, 6]. Dorsiflexion stiffness reliability results for the present study have been similar [32, 33] or better [37, 38] than the findings in other similar studies. In addition, the inclusion of a high velocity stretching (180
EMG activity was recorded to quantify neurogenic components of muscle tone, mainly due to the tonic stretch reflex that theoretically is present in high velocity stretching but not during low velocity stretching [6, 24]. However, our results showed similar percentages of EMG activation at slow (10
Muscle extensibility is a critical dimension of muscle length and it is usually measured as maximal PROM [11, 15, 25]. However, there are several methods to quantify maximal dorsiflexion PROM [41] that mainly distinguish three types of endpoints where the mobilisation finishes: i) when the endpoint is determined by the examiner’s perception, usually as “firm resistance” [42]. This method does not usually measure the amount of applied torque required to perform the stretch, and the validity and reliability of this endpoint are highly questionable [11]; ii) when the endpoint is determined by the subject’s sensory perception. Although subject sensation is the most frequently used endpoint in human stretching research, there is little consensus regarding which sensation is most clinically relevant [11, 12]. The use of this method based on a sensory perception of stiffness has been criticised when evaluating passive muscle properties [11]; and iii) when the endpoint is defined by a specific amount of force or moment applied. The high reliability found in the present study and others [41, 43] suggests that applying the same amount of force to all subjects reduces the variability of subsequent readings between the same subjects and is a good method to quantify Triceps Suralis muscle extensibility. Although the relation between muscle extensibility and muscle stiffness has been suggested [13], no direct association has been evidenced [44].
Although several studies have calculated the reliability of isometric strength measurement using isokinetic dynamometers [18, 20], only some of them measured plantarflexion muscles, finding slightly lower ICCs [18, 45]. However, these studies evaluated older people and subjects with intermittent claudication. The measurement of the peak isometric plantarflexion force using an isokinetic dynamometer has a very good intra- (0.94, 0.86–0.98) and inter-day (0.92, 0.80–0.97) reliability.
There is a general controversy between the abstract concept of muscle tone, which is most used from a clinical perspective [46], and passive muscle properties, such as muscle stiffness, that are used in a biomechanics context. This could be confusing when both concepts are assessed with similar protocols based on passive resistive torque [6, 35]. However, muscle tone is also influenced by efferent innervation of the muscle (neurogenic component). This misunderstanding has also been observed using other measurement methodologies, such as myotonometers [31]. To avoid this, the proposed protocol in the present study suggests that muscle tone should be assessed in a comprehensive way, including other mechanical properties of the muscle, such as strength and extensibility, as well as the neurophysiological component using electromyography activity records.
Having a reliable and comprehensive protocol to quantify muscle tone and its associated components could be useful in several areas, such as to investigate the implications of muscle tone in sports performance, or to have healthy-experimental models to test new muscle tone disorders managements [34, 47]. Although more reliability studies are needed in specific populations, this comprehensive protocol is suitable to quantify muscle tone disorders such as contractures, hypertonia or spasticity. Furthermore, direct relations among muscle stiffness, extensibility and strength [13, 14, 44] and their role in muscle performance and task execution should be deeply studied. Moreover, other aspects such as the measures of responsiveness to change should also be addressed in future studies. The possibility of detecting the amount of change over time that is clinically relevant as a response to an intervention is an important key for validating these types of protocols [36].
One of the limitations of this study is that the measurement of the passive resistive torque was performed only at two velocities (slow and fast). It would be desirable to perform a wider range of velocities to have deeper information about both the neural mechanisms and the viscoelastic properties of muscle tone. However, the idea of the proposed protocol is to develop a practical and replicable procedure to measure muscle tone and adding more velocities would increase considerably the time required during each session. Another point to highlight is the pooled analysis of data in terms of gender or age. Expected differences in muscle tone could be found between genders or between young and old population and could bias the study. However, the idea of this study was to compare the measurements of each subjects with those performed by him/herself in a short period of time, and not to analyze the differences of gender or the influence of an intervention.
Conclusions
The comprehensive protocol of muscle tone measurement here tested, which includes passive resistive torque, muscle extensibility, strength and EMG activity, may represent a valid tool and has exhibited high reliability in quantifying muscle tone in non-injured subjects. Evaluation techniques that include multiple dimensions of muscle tone provide tools to better assess muscle status and the effect of therapeutic interventions. More studies are needed to understand muscle tone and its alterations, as well as more precise assessments, allowing for selection of the intervention that will best address the specific disorder or to assess the effects of training protocols in order to optimise the muscle status to performance.
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest derived from the outcomes of this study. This study did not receive any funding.