
Abstract
BACKGROUND:
Shoulder function is directly related to scapular kinematics and the scapula has always been a part of shoulder rehabilitation. Kinesio Taping (KT) is a specific taping technique where flexible tapes indirectly stabilize underlying soft tissues to modify their behavior. KT has been utilized for scapular stabilization in shoulder rehabilitation but its effect on shoulder strength was not examined before.
OBJECTIVES:
The aim of this self-controlled therapeutic study was to assess the effect of KT on shoulder scapation (arm elevation in scapular plane) strength in healthy individuals.
METHODS:
This study was conducted on 160 shoulders of 80 healthy volunteers (34 males, 46 females; mean age: 23.8 [18–30]). The shoulder scaption strength was recorded, using an electronic dynamometer, as the maximal value of 3 consecutive measurements in two different forearm positions: ‘palm down’ and ‘empty can’. Two sets of measurements, 3 days apart, were taken. The results of untaped and taped measurements were compared. Scapular taping, dominant side, forearm position, sex, and body mass index (BMI) were analyzed.
RESULTS:
The test-retest findings of both forearm positions were highly correlated with ICCs ranging 0.978–0.990. There was no significant difference in strength between ‘without KT’ and ‘with KT’, 69.46
CONCLUSIONS:
Based on our comparisons, scapular KT does not appear to influence scaption strength in healthy individuals.
Introduction
There is a strong association between scapular dysfunction and shoulder disorders. Thus, improving scapular stability has become an effective strategy in most rehabilitation protocols [1, 2, 3]. While supervised periscapular muscle training programs are the mainstay in most scapular stabilization protocols, lack of standardization, and sustainability are their major drawbacks.
Kinesio Taping (KT) is a specific taping technique where flexible tapes indirectly stabilize underlying soft tissues to modify their behavior [4]. This standardized and sustainable functional stabilization method has been proposed to improve scapular alignment [5].
We hypothesized that if KT improves scapular stabilization in healthy volunteers, this would positively affect shoulder scaption (abduction in scapular plane) strength which is a well-known outcome measure for the assessment of scapular stabilization [6]. The aim of this study was therefore to compare shoulder scaption strength of healthy volunteers before and after the application of KT.
Methods
Subjects
Eighty healthy volunteers (34 males, 46 females; mean age: 23.8 (range: 18–30) took part in this study. They were recruited following an institutional website announcement and informed about the test, while remaining blind to the study question. Before inclusion candidates were questioned and examined for a musculoskeletal or a systemic problem, which would interfere with the strength measurement. Those with previous shoulder surgery, trauma history in the last 3 months and shoulder or scapular asymmetry were excluded. Thus, the study was conducted on 160 shoulders of 80 healthy volunteers (34 males, 46 females; mean age: 23.8 [18–30]) who fulfilled the inclusion criteria. An institutional review board approval was obtained before the study (Koc University, Istanbul, Turkey; 2014.023.IRB2.010).
Procedure
Taping was performed by the same researcher, who was trained in the method prior to the study. Three tapes were used in each case: The first two from each acromioclavicular joint to the contralateral inferior angle of scapula, and a transverse tape through scapular spines. Subjects retained both scapulae in a retracted position during the taping procedure (Fig. 1).
Measurement position: Standing with the arm in 90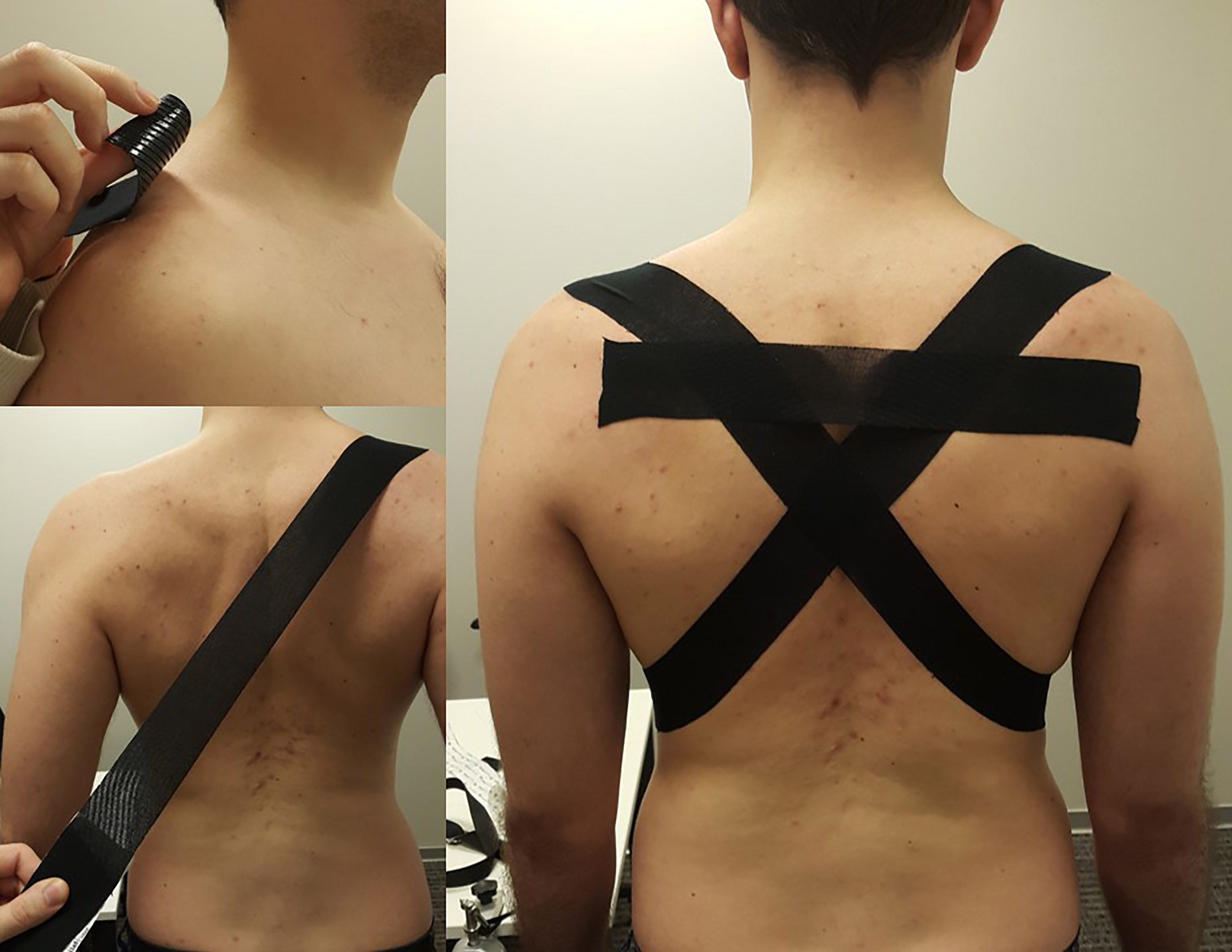
Isometric scapation strength was recorded, using an electronic dynamometer (Mecmesin Myometer, West Sussex, UK) with a real time display. Measurement took place in standing with the arm in 90
Measurement position: Standing with the arm in 90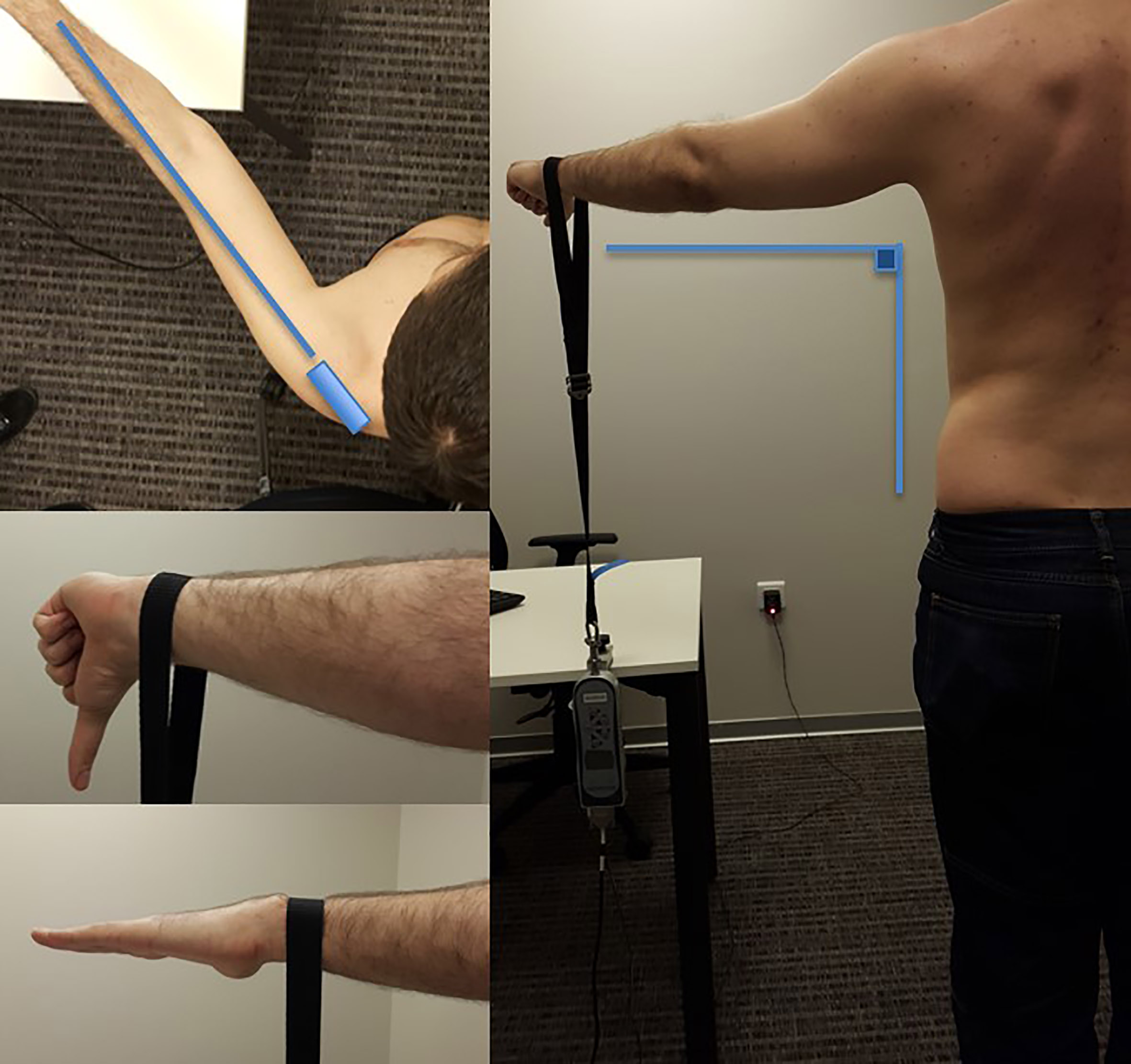
Statistical analyses were performed using IBM SPSS Statistics, Version 23.0 (IBM Corp, Armonk, NY, USA). In addition to descriptive statistical methods (average, standard deviation), paired and unpaired student’s
Results
All 80 volunteers attended the second step of the measurement in the given period and completed the study. Average height, weight and body mass index (BMI) were 1.72
Intraclass correlation coefficients (ICC) and %95 confidence intervals of different measurements. Note that ICC is above 0.7 which is accepted as the minimum level for the reliability of a test
Intraclass correlation coefficients (ICC) and %95 confidence intervals of different measurements. Note that ICC is above 0.7 which is accepted as the minimum level for the reliability of a test
EC: empty can; PD: palm down.
The mean scaption strength of the dominant side (71.73
Dominant and non-dominant measurement values of volunteers in both positions, with and without taping. Dominant side strength was superior to non-dominant side significant in all measurements (
EC: empty can; PD: palm down.
Effects of taping on shoulder strength in two different positions and for both dominant and nondominant sides. There was no statistically significant difference (
EC: empty can; PD: palm down.
The mean scaption strengths before and after KT were 67.41
Both the male sex and the BMI showed positive correlation on maximum shoulder strength (
Our hypothesis was based on the idea that Kinesio Taping would provide a sustainable and standard home-based modality for the rehabilitation of scapular disorders. For this purpose, we wondered whether the KT indirectly affects shoulder scaption strength, based on the widely accepted concept of a stabilized scapula enhancing shoulder function. Considering the beneficial results reported in different studies for various anatomic locations, it was expected that the Kinesio Taping would improve shoulder scaption strength immediately after application, in healthy subjects. However, the results of this research reject the proposed hypothesis. There was no statistical difference between measurements without and with taping, in both genders.
The measurement method used in this study was attributed to Constant et al.’s publications on his shoulder outcome score [7, 8]. There are still some controversies on the ideal measurement technique for shoulder strength. Although the standing position and 90
Three consecutive measurements were performed to achieve the highest strength record. This technique was reliable as shown in our results with a high ICCs for both test positions. There are different recommendations in the literature regarding the forearm position [6, 9, 10, 11], and there is no consensus favoring one over the other, therefore we compared both techniques in order to substantiate a recommendation. However, the current results indicate that both forearm positions are reliable while the results are consistent with each other.
Although there is considerable number of studies regarding KT, its validity has not been sufficiently probed for any body part. In our method the obliquely positioned tape acted as the scapular reposition test (modified scapular retraction test) exerting a posterior tilt and external rotation effect, assisting in forward elevation and possibly improving shoulder strength [12, 13]. The transverse tape also assisted in supporting the retracted position of the scapula. We combined these two taping methods to achieve a stabilized scapula in a retracted position, and also to support and positively affect the upper body posture.
A significant positive effect of KT on muscle strength was suggested in several comparative studies. Hsu et al. on lower trapezius muscle [14], Vithoulka et al. [15] and Fu et al. on quadriceps [16], Lee et al. on flexor muscles of the hand [17] and Hagen et al. on back extensor muscles [18]. Hsu et al. and Slupik et al. also reported significant effects on muscle activity measurement with electromyography [14, 19]. Compared to the mentioned anatomical locations, the scapula and shoulder present a more complex musculature with a thicker subcutaneous tissue. However, Shaheen et al. managed to show scapular motion alterations with KT using a motion tracking system, suggesting that previously studied beneficial effects may also be valid for scapula and shoulder. Scapular taping increased the scapular external and upward rotations and posterior tilt in elevations in the sagittal plane [5]. Our results, do not support such an immediate stabilization effect and enhancement on shoulder strength.
This study is limited by the absence of scapular motion tracking, or another method to assess scapular stabilization. Furthermore, it is not possible to make a negative conclusion on KT’s overall role on shoulder rehabilitation, as the study assessed only the immediate effects.
Our study suggests therefore that scapular KT has no immediate effect on shoulder muscle strength. The long term utilization of KT has yet to be explored with different taping methods to prove its role in shoulder rehabilitation.
Footnotes
Acknowledgments
The study protocol was approved by the Medical Ethics Committee of the Koç University, Istanbul, Turkey (2014.023.IRB2.010).
Conflict of interest
The authors certify that they have no affiliations with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in the article.