
Abstract
BACKGROUND:
The diagnostic accuracy of manual muscle testing (MMT) has been examined- but not for grip strength.
OBJECTIVE:
Determine the diagnostic accuracy of MMT relative to grip dynamometry for identifying patients with weak grip strength.
METHODS:
This study involved the secondary analysis of grip strength data obtained from 61 patients managed in a home care setting. The concordance between weakness identified using MMT and grip dynamometry was examined.
RESULTS:
The agreement between MMT and dynamometry was about 70%. Kappa suggested fair agreement beyond chance. Sensitivity and specificity ranged from 66.7 to 73.4 percent.
CONCLUSIONS:
Grip strength measured using MMT lacks sufficient diagnostic accuracy to advocate its use – at least with patients seen in a home setting.
Introduction
Grip strength is widely used as an indicator of overall strength and as a biomarker of health status [1]. Although dynamometry is often employed for measuring grip strength, manual muscle testing (MMT) is also used [2]. Measurements of grip strength obtained by MMT have been shown to have good test-retest (
The purpose of this study, therefore, was to explore the diagnostic accuracy of grip strength measured by MMT. My expectation was that MMT measures of grip strength, like those of knee extension strength, would lack sufficient diagnostic accuracy to justify their use in lieu of dynamometric measures grip strength.
Methods
This study involved the secondary analysis of data recorded in the initial therapy notes of patients managed personally in a home-care setting by the author. Use of the data without consent was approved by the Institutional Review Board of the University of Connecticut (H10-316).
Measurement of hand-grip strength by manual muscle testing (top) and dynamometry (bottom).
Description of manual muscle test (MMT) grades and associated scores (kg) obtained by dynamometry
Of 71 consecutively evaluated patients, 61 had MMT and dynamometer measurements of grip strength recorded for both hands in their initial notes and were included in the study. All were adults with a mean (range) age of 68.4 (32–94) years. Most of the patients (
Patients with MMT grip scores below 5/5 were considered to be weak. Based on literature focused on the knee [7, 10], patients with dynamometer measured grip forces more than 20% below side, gender, and age matched reference values were considered to be weak [11, 12]. The reference values used were the mean and the lower limit of the 95% confidence interval of the mean (e.g., 17.1 and 14.5 kg for the left hand of an 82 year old woman).
MMT and dynamometer scores (
Dot plot showing distribution of dynamometer scores between manual muscle test grades.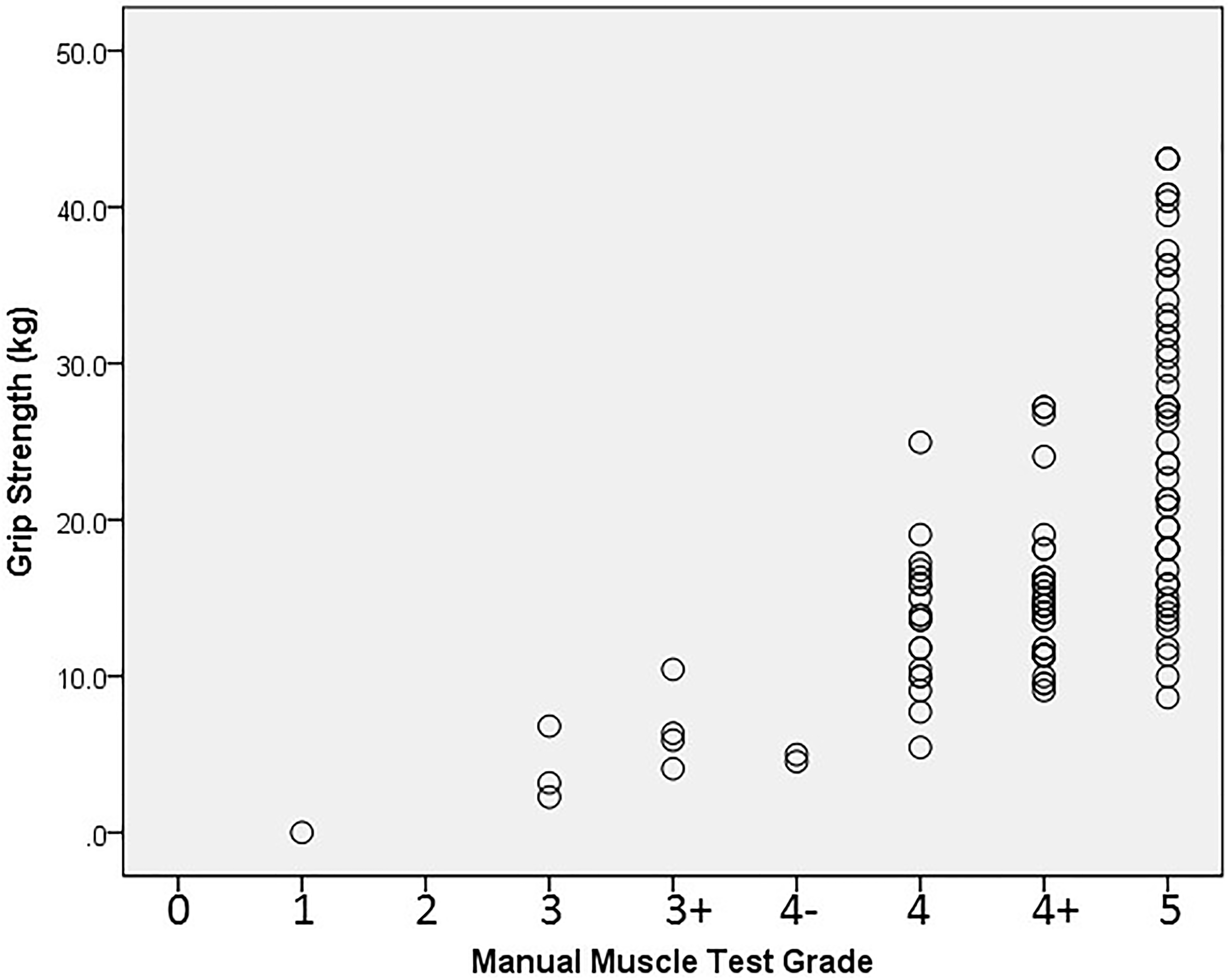
Statistics related to the diagnostic accuracy of manual muscle testing of grip strength
PPV
Table 1 shows the distribution of MMT and dynamometer scores. With one exception, all patients obtained a MMT score of 3/5 or greater. Dynamometer scores ranged from 0 to 43 kg. The dynamometer scores associated with the higher MMT grades were widely dispersed (Fig. 2). Two observations highlight this fact. First, for patients with a MMT grade of 5/5, the highest dynamometer score (43 kg) was more than 4 times greater than the lowest score (9 kg). For patients with a MMT grade of 4
Discussion
The accurate diagnosis of muscle weakness is crucial to determining patient status and the need for therapeutic interventions. As other studies have demonstrated for knee extension strength measured by MMT, this study showed that grip strength measured by MMT lacks diagnostic accuracy. Neither the sensitivity nor the specificity of MMT met the 90% standard recommended by Lincoln et al for screening tests [14]. Consequently, patients with vastly different grip strengths (according to dynamometry) are likely to be given the same MMT grade and patients with different MMT grades are likely to have similar grip strengths (as determined by dynamometry).
This study has several limitations that may affect the generalizability of the findings. First, all patients were seen in a home-care environment. The range of MMT and dynamometer measurements obtained, therefore, may differ from those obtained from other populations (eg, patients in intensive care) [15]. Second, a single male examiner performed all MMT. Male examiners typically apply more force than female examiners [16]. Finally, a 20 percent deficit in dynamometer measured force was used as a criterion for establishing weakness. Although there is precedence for the criterion, others have used different criteria. For example, Alley et al used 26 kg as a standard for men and 16 kg as a standard for women [17].
Footnotes
Conflict of interest
None to report.