
Abstract
BACKGROUND:
There have been conflicting findings regarding the relationship between ankle muscle fatigue and a fatiguing run due to different selections of running protocol. Bruce protocol is strongly established as a maximum graded exercise test for volitional fatigue.
OBJECTIVE:
To determine if volitional exhaustion utilizing the Bruce protocol would result in localized ankle plantarflexor (PF) and dorsiflexor (DF) fatigue.
METHODS:
Twenty-three healthy individuals participated. Participants ran on a treadmill until they reached volitional exhaustion during performance of the Bruce protocol. Before and after volitional exhaustion, participants performed 3 maximum voluntary isometric contractions for both PF and DF with electromyography (EMG) assessing activation of the tibialis anterior, peroneus longus, and medial gastrocnemius muscles.
RESULTS:
Volitional exhaustion resulted in ankle PF fatigue (moment:
CONCLUSIONS:
That the general fatigue induced by the Bruce protocol caused ankle PF and DF fatigue. Identifying and understanding the neuromuscular responses to volitional fatigue following running are helpful in not only improving the comfort and enjoyment of physical activities, but also in enhancing training and safety of injuries associated of these activities.
Introduction
Participation in sports and recreation is ever-increas-ing due to enhanced opportunity and desire for individuals to remain physically active. Consequently, the incidence of activity-related injuries has increased due to this overall elevated level of exposure to sports [1]. Approximately 40% of all athletic injuries occur at the ankle joint [2]. Fatigue is hypothesized to be one of many potential causative factors for these injuries in competitive and recreational athletes [2, 3]. In fact, the majority of ankle injuries occur near the end of a game when the participants are more likely to be fatigued [2, 3]. Mechanistically, it has been suggested that fatigue results in a decrease in a stabilizing capacity of an ankle musculature, resulting in an increased risk of ankle injuries [4].
Fatigue has been described in a number of different ways [5]. Local muscle fatigue protocols which commonly use an isokinetic dynamometer have been used to examine the effects of ankle muscle fatigue on postural control, neuromuscular function, proprioception, ankle joint mobility, and ground reaction forces during balance tasks [3, 6]. However, these local fatiguing protocols are artificial as they do not mimic lower extremity and ankle movements that are typical during physical activity or sport. While localized fatigue may be effective, muscles and joints are activated and move differently in closed-chain and through unconstrained tri-planar motion (i.e. running) [7]. Thus, it is necessary to investigate the effect of a functional fatiguing exercise on localized muscle activation and joint function.
General exercise such as walking, running, or cycling involves multiple joints and many muscle groups resulting in whole body displacement in space [5, 8]. Running is required during most of the competitive sports and requires significant cardiovascular and muscular effort. Further, running and gait are strongly associated with the ankle structure because the ankle plantarflexors (PF) and dorsiflexors (DF) have important roles in gait and fall prevention [9, 10]. Specifically, PF powers the gait cycle and helps to establish a rigid lever for pushoff [10]. The DF are responsible for controlling foot placement after initial contact, controlling pronation, and for maintaining toe clearance during swing [9]. While both muscle groups function primarily in a sagittal plane, they are partly responsible for maintaining stability in secondary planes [11].
Ankle muscle fatigue by repetitive contractions of PF and DF to absorb shock during running has been hypothesized to be causative factor for running injuries associated with the ankle. For example, it has been reported that exhaustive running results in decreased dorsiflexion angle at heel contact and increased rearfoot motion, both of which may be associated with running injuries [12]. While functional fatigue has been shown to change running mechanics and postural control, the underlying neuromuscular mechanism of these changes is not completely known [5, 12]. Investigating the local neuromuscular effect at the ankle of a fatiguing run may aid in a partial understanding of the etiology of running and athletic injuries.
A number of studies have used running as a method of fatigue in order to investigate its effect on ankle fatigability in athletes [5, 8]. For example, Fourchet et al., reported that male long distance trail runners demonstrated decreased PF but not DF from pre-to post-5-h hilly run [13]. However, another Fourchet et al.’s study showed that male adolescent distance runners have not demonstrated decreased isokinetic peak moments of PF and DF in post compared to pre-high intensity running to exhaustion [14]. In addition, Mizrahi et al., showed the average activation of the tibialis anterior decreased from the beginning to the end of 30 min treadmill running but not gastrocnemius [15]. One of factors to influence conflicting findings in ankle fatigability from the previous studies may be the running protocol. The previous studies have used their own running protocols that are not well established for general fatigue with reliability and validity.
The Bruce protocol is a widely-used, maximum-graded exercise test performed on a treadmill [16]. Fatigue following performance of the Bruce protocol has been estimated using several parameters including changes in venous blood oxygen saturation, maximum heart rate, lactate production, glycogen metabolism, and Borg scale (RPE) as well as volitional exhaustion [17, 18]. These measures of physiological fatigue are considered reliable for indicating both the anaerobic threshold and general fatigue [19]. In addition, biomarkers for VO
To the best of our knowledge, no relationship has been established between localized muscle fatigue on the ankle and volitional exhaustion utilizing the Bruce protocol. This relationship may contribute to a better understanding of the mechanism of injuries of the ankle joint in sports and recreation involving running. Therefore, the purpose of this study was to determine whether volitional exhaustion induced by the Bruce protocol results in localized ankle muscle fatigue. It was hypothesized that the Bruce protocol would result in ankle muscle fatigue of PF and DF.
Methods
Participants
Based on previously published data utilizing similar variables to those in the current study, an a priori power analysis (
Injury questions completed by participants showed that all participants reported no history of lower extremity injury including ankle sprains. In order to participate in the study, all participants were classified as low risk for cardiovascular disease according to current American College of Sports Medicine (ACSM) Guidelines for Exercise Testing and Prescription. In addition, all participants engaged in
Assessment of volitional fatigue
ACSM guidelines for the Bruce protocol were used to determine fatigue and thereby justify termination of activity prior to completion of the entire protocol [18]. Participants performed the Bruce protocol on a Trackmaster treadmill (Full Vision Inc., Newton, Kansas), and their heart rate was measured continuously using a ParvoOneMax system (Parvo Dedics, Salt Lake City, UT, USA) and Polar HR monitor (Polar electro Inc., New Success, NY, USA). Participants walked for 3 minutes at 0.8 m/s with 0% grade. After the first 3 minutes, incline was elevated by 2% every 3 minutes with simultaneous increases in speed to 1.1, 1.5, 1.9, 2.2, and 2.5 m/s until volitional exhaustion was reached. RPE measured perceived exhaustion and was collected every 3 minutes on a scale of 6–20 [20]. While performing the Bruce protocol, verbal encouragement was provided. If the subject’s heart rate exceeded age-associated maximum heart rate (220-age), activity was terminated. Other indications for test termination included angina, dizziness, nausea or volitional exhaustion [18]. Subject characteristics during the test are shown in Table 1.
The mean and standard deviations for participants’ max heart rate (HR
) and heart rate (HR), duration of running and ratings of perceived exertion scale (RPE) at volitional exhaustion
The mean and standard deviations for participants’ max heart rate (HR
Values are mean
A single visit was required for all participants. Before beginning, participants rode a stationary bike for 5 minutes as a warm-up exercise. Electromyography electrodes were placed on each participant’s tibialis anterior, peroneus longus and medial gastrocnemius, and the reference electrode was placed on the tibial tuberosity of their dominant leg (defined as: the side used to kick a ball). Maximum voluntary isometric contraction (MVIC) was performed on an isokinetic dynamometer (BIODEX, INC, Shirley, NY, USA).
For the MVIC, participant’s ankle axis of rotation (medial and lateral malleoli) was aligned with a dynamometer shaft and participants kept the knee fully extended with a limb-support pad and appropriate straps. Participant’s ankle was set at 90 degrees (neutral position). The seatback angle was set to 70 degrees. While performing the MVIC, participant’s arms were crossed over the chest. Participants performed a single set of warm-up contractions at 50% and 75% each of perceived MVIC. Participants then rested for 10 minutes prior to beginning testing. While performing the MVIC, verbal encouragement was provided. Participants performed one MVIC in the plantarflexion direction for 5 seconds followed by another MVIC in the dorsiflexion direction for 5 seconds. Participants rested for 5 seconds between trials. A total of 3 MVICs in both directions were performed while recording with the wireless EMG system (Telemyo 2400 G2, Noraxon, Scottsdale, AZ, USA). The raw EMG signal was digitally sampled at 1000 Hz, and bandpass filtered during data collection from 10 to 500 Hz.
After performing the pre-fatigue test, participants performed the Bruce protocol on a treadmill. Participants ran until they reached volitional exhaustion as previously described. After finishing the Bruce protocol, participants performed 3 MVICs in each PF and DF as described above. The time delay between the Bruce protocol and the post-fatigue test was about 1 minute.
Statistical analysis
The variables of interest for the current study were average peak moment for PF and DF as well as mean median frequency and mean amplitude for tibialis anterior, peroneus longus, and medial gastrocnemius. Four separate two-way (time x direction) repeated measures analyses of variance (ANOVA) were used to assess the effect of fatigue (pre and post-fatigue) for ankle moment and EMG activation. Separate paired t-tests were used for post-hoc testing to assess the effect of fatigue (pre and post-fatigue) for peak moment in PF and DF and median frequency and mean amplitude for all included muscles. For all statistical tests, the level of significance was set at 0.05.
Peak moments of plantarflexors (PF) and dorsiflexors (DF) in pre and post-Bruce protocol. Values are mean 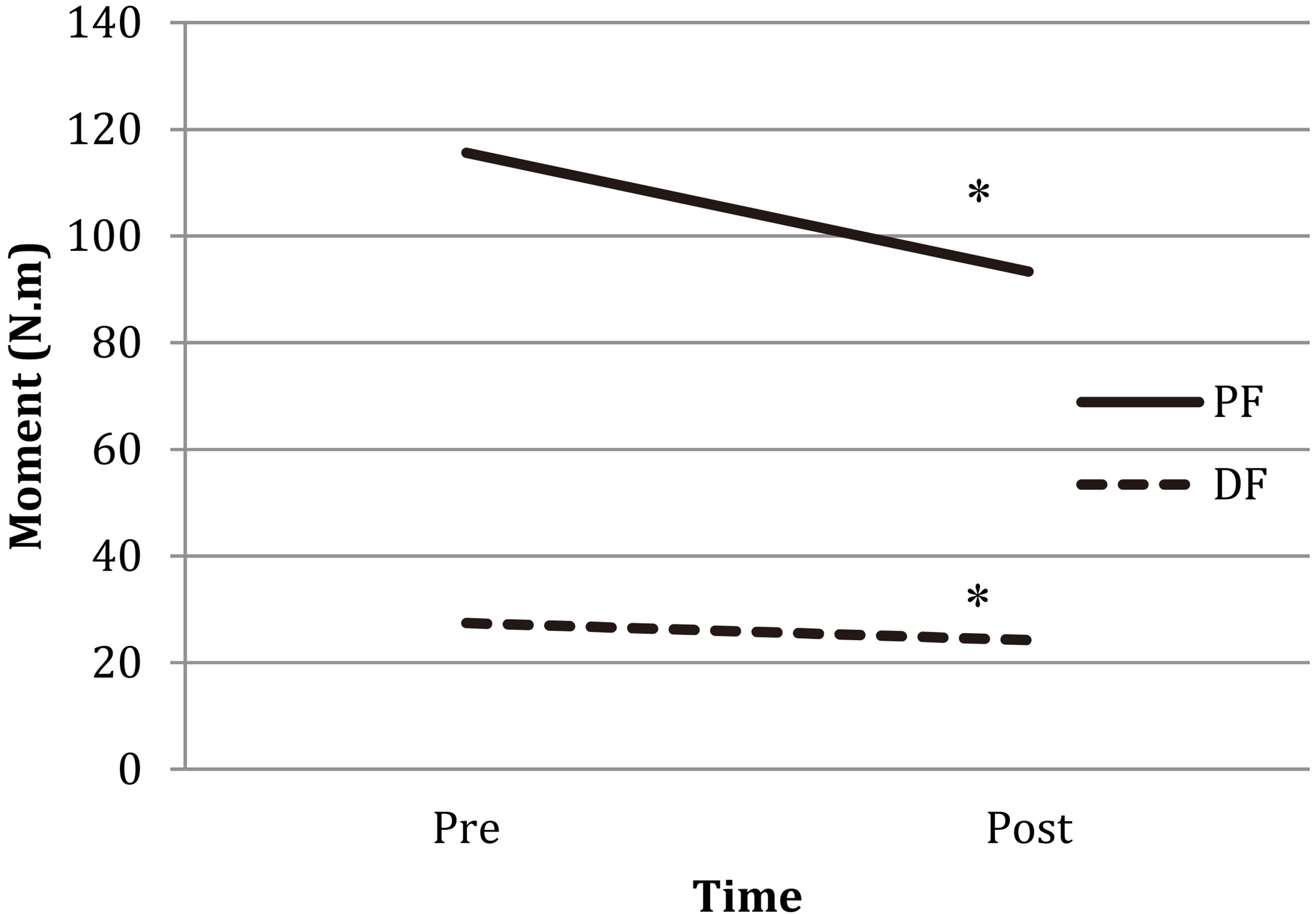
Median frequent and mean amplitude of tibialis anterior in pre and post-Bruce protocol Values are mean 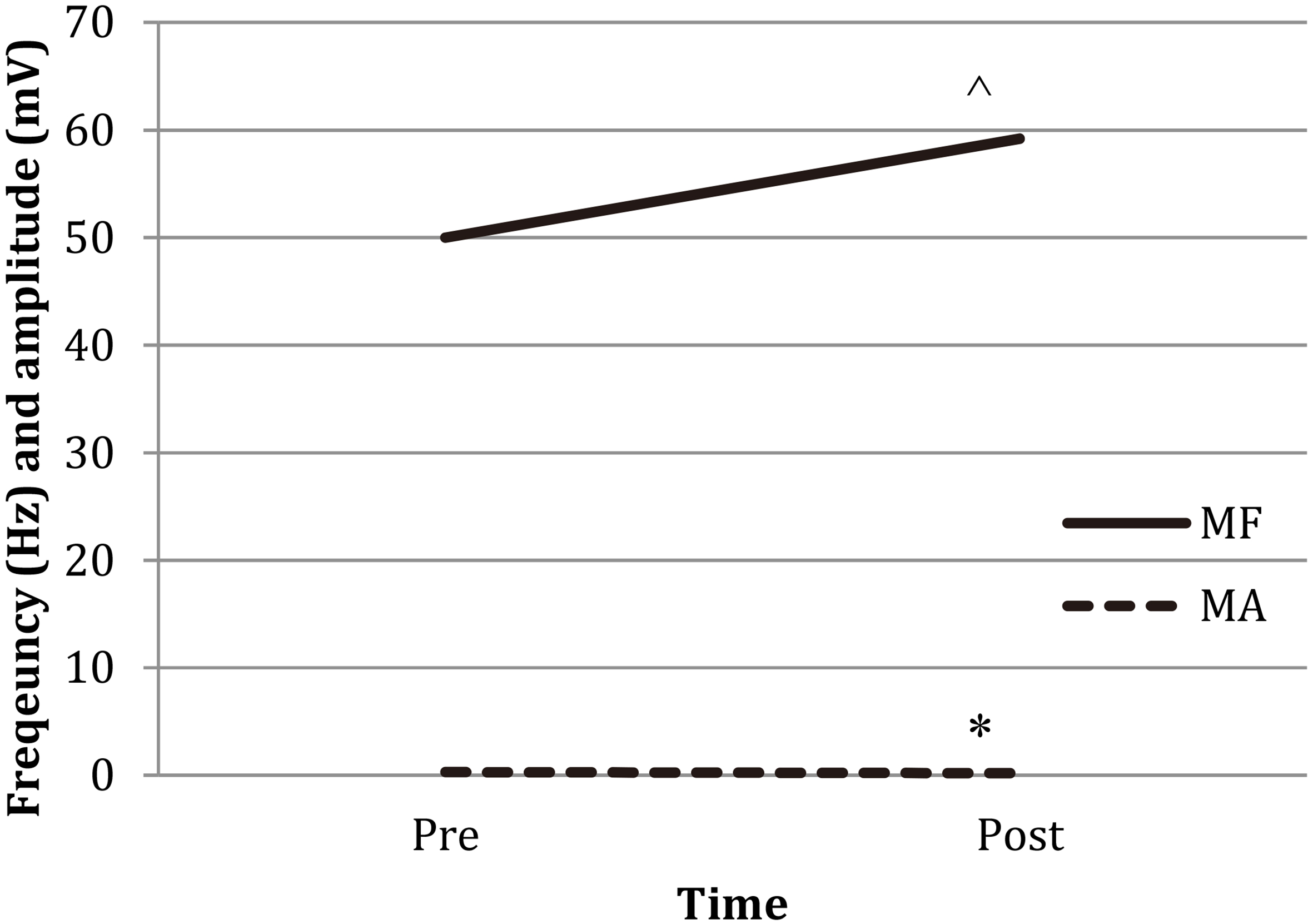
There was a significant interaction between time and direction for moment. (F 1,23
The mean, standard deviations, and percent difference (%) for peak moment of plantarflexors (PF) and dorsiflexors (DF) and median frequency (MF) and mean amplitude (MA) of anterior tibialis (TA), peroneus longus (PL), and medial gastrocnemius (MG) from 3 trials in pre and post-fatigue tests
The mean, standard deviations, and percent difference (%) for peak moment of plantarflexors (PF) and dorsiflexors (DF) and median frequency (MF) and mean amplitude (MA) of anterior tibialis (TA), peroneus longus (PL), and medial gastrocnemius (MG) from 3 trials in pre and post-fatigue tests
Values are mean
The purpose of this study was to determine whether volitional exhaustion induced by the Bruce protocol resulted in localized ankle muscle fatigue in a non-injured population. It was hypothesized that the Bruce protocol would decrease peak moments and change electromyography activation of PF and DF. The results of this study were mixed. It was determined that the Bruce protocol resulted in localized fatigue of ankle PF and DF as evidenced by a reduction in peak moment during an MVIC. While there were decreases in muscle activation and frequency of the tibialis anterior, there were no significant changes in mean amplitude and median frequency of the medial gastrocnemius and peroneus longus following the fatiguing protocol.
The main difficulty with a study of this nature is accurately obtaining and determining the extent of fatigue. Mean RPE at the time of volitional exhaustion was 20 which indicates that participants were working as hard as possible. Also, participants’ heart rates approached their individual maximum heart rates which serves as an indicator of VO
Although this study did not statistically analyzed the difference between PD and DF moments, means of moment showed a greater moment reduction in PF than DF after the fatiguing run. Because PF is a muscle group that is primarily responsible for powering the gait cycle, and the participants in the current study were required to run uphill, this result seems reasonable. Similarly, it has been reported that MVIC activation of PF decreased while there was no change in DF after 5 hours of hilly running [13]. Further, it has been demonstrated that DF was less fatigued than PF during a hilly run compared to a level or slight uphill run [13]. In contrast, it was reported that DF moment had greater declines than PF during a sustained maximum contraction [24]. Additionally, it has been reported that there is no difference in moment reduction for ankle PF and DF after an isometric fatiguing protocol [25]. Because these studies utilized an isometric contraction as method of fatigue, it is possible that DF were activated to a greater extent than during the fatiguing run, thus resulting in greater declines than in the current study.
In the current study, both median frequency and mean amplitude of EMG in the tibialis anterior were decreased after the fatiguing run. A decreased EMG signal from the tibialis anterior corresponds to a decreased peak moment of DF as the tibialis anterior is the prime mover for DF. Decreased mean amplitude suggests decreased muscle activation levels, and decreased median frequency is an indicator of muscle fatigue [26, 27]. Co-contraction of the ankle muscles and joint angles of the ankle has demonstrated a greater impact force during initial contact phase of running [28, 29]. Specifically, decreasing the initial angle of the ankle from the ground during heel contact resulted in an increased impact force [28, 29]. These studies suggest that if the tibialis anterior is lengthened by increasing the angle of the ankle at heel strike, the ankle could have greater potential PF range of motion and require more eccentric control [28, 29]. This would aid in dissipating the impact force by absorbing greater energy. However, fatigued DF may lead to decreased eccentric contraction, thereby resulting in an increase in ground reaction force. It has been suggested that greater ground reaction force is associated with running injuries [28, 29]. Therefore, results from the current study suggest that fatigued DF caused by a fatiguing run could increase the incidence of running injuries related to changes in ground reaction force parameters.
While peak moment of PF showed a reduction, there were no changes in electromyography activity of the PF muscles after fatigue. An initial activation of PF occurs prior to the peak burst of electromyography activity during DF [30]. Therefore, in order to accelerate the ankle quickly, DF needs to overcome the cocontraction of PF [31]. When walking or running speed is increased, ankle angular acceleration is also increased with increased activity of DF [31]. Based on these results, when speed was gradually increased during the Bruce protocol, dorsiflexion velocity was also increased. In addition, activity of the tibialis anterior was active for 50–85% of the running cycle which suggests that the muscles were active during stance as well [32]. This may be due to the need to work against the high demand and output of PF. High levels of DF muscle activity are necessary just after initial contact to avoid foot slap and during swing to avoid foot drop, to avoid dragging the toes and to prepare for initial contact [9].
The mean, standard deviations, and percent difference (%) for peak moment of plantarflexors (PF) and dorsiflexors (DF) for women and men
The mean, standard deviations, and percent difference (%) for peak moment of plantarflexors (PF) and dorsiflexors (DF) for women and men
Values are mean
In the current study, both median frequency and mean amplitude of EMG signals in the peroneus longus and medial gastrocnemius were not decreased indicating that they were not fatigued. The MVIC measurement of plantarflexion in this study includes all PF including medial gastrocnemius, peroneus longus, tibialis posterior and soleus. However, the current study measures only EMG activities of peroneus longus and medial gastrocnemius. Both soleus and gastrocnemius contribute significantly to the ankle in supporting forward progression and mediolateral balance in running [33]. Specifically, these muscles contribute most significantly to forward acceleration in the second half of stance, and the soleus works as the major stabilizer throughout stance [33]. Thus, it seems reasonable to explain that the medial gastrocnemius may not demonstrate reduced muscle activity as there are multiple large muscles acting as agonists during activity. While the peroneus longus is one of the primary evertors, it is also a secondary muscle for PF. In order to accurately examine fatigability of peroneus longus, a measurement of MVIC in eversion should be performed.
The Bruce protocol has been extensively utilized for measuring VO
The findings of this study are important in understanding the neuromuscular mechanism of injuries associated with fatigue during sport or physical activities. It has been suggested that running leads to a strengthening of structures of the ankle complex and thereby strength of the ankle muscular structures may have protective character with respect to injuries associated with running [38]. Moreover, muscle fatigue has been hypothesized to be the one of causative factors in running injuries. For example, intense running may cause muscle fatigue which results in alteration of the muscle’s shock absorbing capability or running mechanics [12, 39]. Abnormal ankle joint motion or excessive impact forces could play a major role in injuries associated with running. There have been claims that muscle contraction in association with joint motion and impact loading during running are strongly associated with localized ankle muscle fatigue [29, 40]. During running, PF and DF generate and control the primary movements of the ankle. Running during the Bruce protocol resulted both ankle PF and DF fatigue. Thus, localized ankle fatigue induced by a functional activity that causes fatigue may be considered as a mechanism of ankle injuries such an ankle sprain, gastrocnemius muscle injury, tibialis posterior tendinopathy, or peroneal tendinopathy.
There are several limitations to the current study. Since there are some data to suggest that strength changes and fatigability differ between women and men, the inclusion of both males and females may complicate the interpretation of the results [41, 42]. However, there also exist some data that have resulted from studies inclusive of men and women [43, 44]. The main purpose of this study was to determine whether the Bruce protocol affects localized ankle muscle fatigue regardless of gender. Because we analyzed % change in difference by comparing pre-fatigue-moment to post-fatigue moment, there should be a limited effect of gender. Additionally, we closely matched the number of subjects by gender in an attempt to reduce gender bias. Table 3 demonstrates no % change differences that exist between genders despite differences in overall force output. Because isokinetic contractions of ankle muscles are required during running, future study should include isokinetic strength in order to comprehensively understand the effects of localized ankle fatigue induced by the Bruce protocol. Finally, a frequency analysis of EMG signals is limited in its ability to determine whether localized ankle fatigue is more impacted by peripheral or central fatigue.
Conclusion
This is the first study to examine the effects of volitional exhaustion utilizing the Bruce protocol on localized ankle PF and DF muscle fatigue. The results suggest that activity-related injuries at the ankle joint may be caused, in part, by ankle PF and DF fatigue resulting from general fatigue induced by running. Identifying and understanding the neuromuscular responses to volitional fatigue following running are helpful in not only improving the comfort and enjoyment of physical activities, but also in enhancing training and safety of injuries associated of these activities.
Footnotes
Acknowledgments
The authors would like to thank research assistants for their help with managing participants in this study. The authors declare to have no support and funding for this study.
Conflict of interest
There is no conflict of interest regarding this study.