
Abstract
BACKGROUND:
Posterior shoulder tightness (PST) has been identified as an important factor that causes scapular dyskinesis. Therefore, rehabilitation programs should focus on an intervention involving a posterior shoulder stretch combined with a scapular stabilization exercise (PSSE). However, few studies have investigated the effects of PSSE on rotator cuff (RC) muscle strength in overhead athletes with scapular dyskinesis.
OBJECTIVE:
To determine the effects of PSSE on RC muscle strength, dynamic control ratio (DCR), range of motion (ROM), and pain.
METHODS:
Twenty-four adolescent baseball players with scapular dyskinesis were randomly allocated to one of two groups which trained for 6-weeks. Group I performed PSSE while group II performed same exercises but without stretching (SSE). The isokinetic peak moment/body weight (PM/BW) of concentric and eccentric external rotation (ERc and ERe) and concentric and eccentric internal rotation (IRc and IRe), the DCR (ERe/IRc and IRe/ERc), ROM, and pain were measured in pre- and post-intervention.
RESULTS:
A time-by-group interaction effect was observed for the concentric and eccentric ER, the DCR, and the ROM only the PSSE group.
CONCLUSIONS:
PSSE intervention is a more effective program than SSE for improving RC muscle strength and balance, particularly in terms of its ER component and the associated DCR.
Flow chart of the study.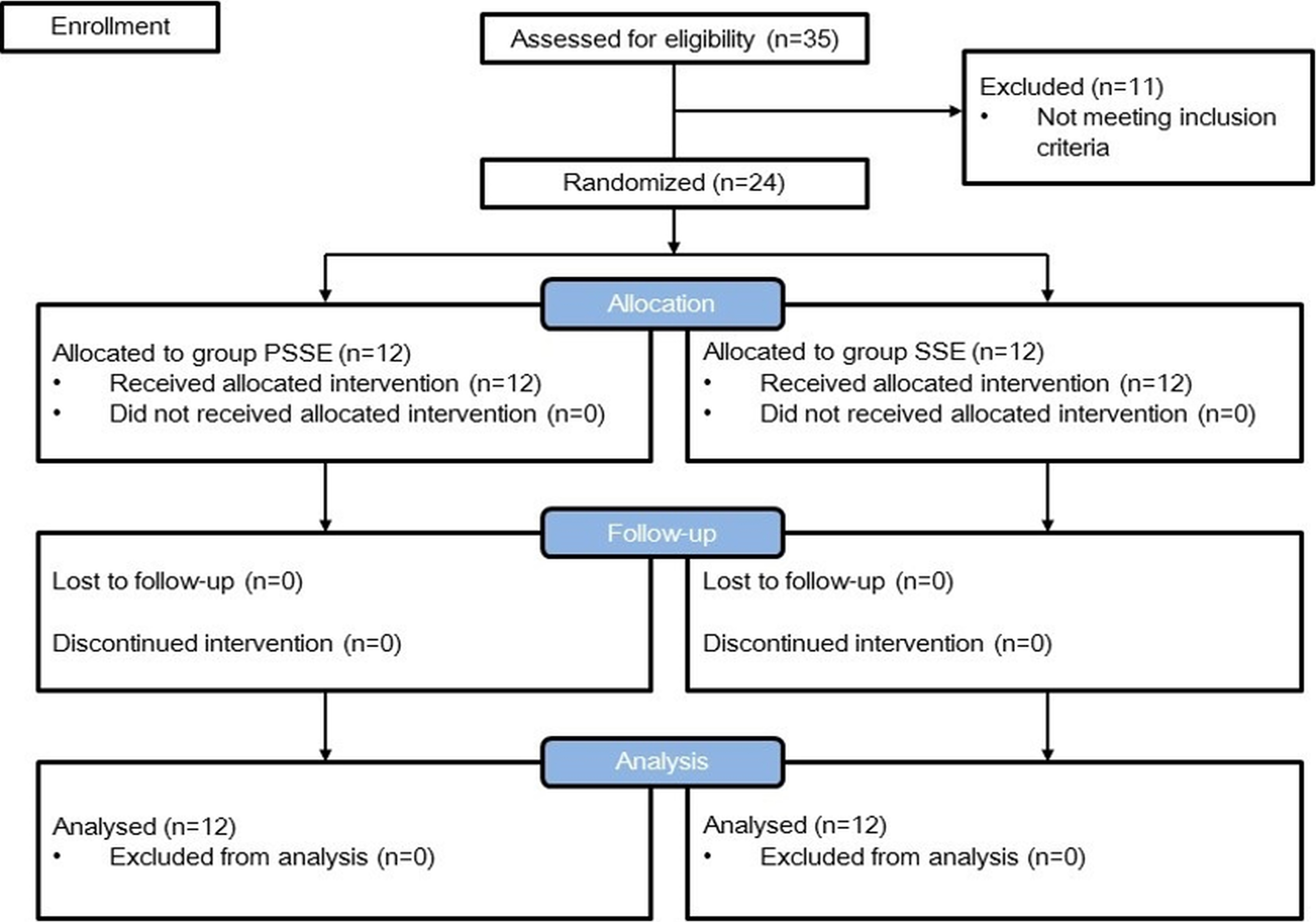
Glenohumeral (GH) joint injuries are common in adolescent baseball players, more than 50% of whom experience shoulder pain [33]. Such injuries are caused by cumulative microtrauma due to repetitive high-velocity dynamic overhead arm motion during throwing [24]. The repetitive throwing motion alters scapular kinematics, defined as scapular dyskinesis, and is common in overhead athletes [17, 18]. Scapular dyskinesis has been associated with rotator cuff (RC) muscle strength, as the scapula provides a stable base of support and an optimal length-tension relationship for the RC muscle. Many factors have been implicated as the cause of scapular dyskinesis, including posterior shoulder tightness (PST), which is thought to be an important factor [5, 19].
A moderate to strong relationship has been reported between PST and scapular dyskinesis in baseball players [19]. PST also leads to GH internal rotation deficit (GIRD) [4, 5, 38], resulting in an imbalance of the shoulder muscles [13, 16]. Recently, an isokinetic study reported reduced isokinetic strength of the shoulder flexor and extensor in high school baseball players with a PST [21]. Guney et al. [13] found a smaller range of motion (ROM) of shoulder internal rotation (IR), decreased strength in external rotation (ER), and a lower ER to IR strength ratio in amateur tennis players with pain. Therefore, rehabilitation programs should focus on posterior shoulder stretch combined with scapular stabilization exercise (PSSE) intervention.
Previous studies have investigated the effects of PSSE on RC muscle strength in patients with scapular dyskinesis. Merolla et al. [28] recently reported increased supraspinatus and infraspinatus isometric strength and reduced pain scores in overhead athletes with scapular dyskinesis. Başkurt et al. [2] reported that stretching with strengthening exercises was effective in improving RC muscle strength and quality of life in scapular dyskinesis patients. Based on this rationale, we believe that PSSE could be effective in improving RC muscle strength in adolescent baseball players with scapular dyskinesis.
However, only a few studies have investigated PSSE effects on RC muscle strength in overhead athletes with scapular dyskinesis, using isometric strength as the outcome measure following PSSE [2, 28, 29]. However, we argue that a measurement of the dynamic strength is strongly indicated to determine the dynamic function of the RC muscle during throwing. Isokinetic dynamometry has been used in objective assessment of shoulder muscle strength and risk of shoulder injury [10]. Fair to good reliability and reproducibility have been reported in previous studies [10].
The purpose of the present study was therefore to determine the effects of PSSE on RC muscle strength, the dynamic control ratio (DCR) of the acting muscles, the GH joint rotational ROM, and the pain in adolescent baseball players with scapular dyskinesis.
Methods
Participants
Thirty-five potential participants volunteered to take part in the study. Following the screening tests, eleven participants were excluded because they did not meet the inclusion criteria. Eventually 24 adolescent male baseball players participated in the study (Fig. 1). Sample size calculation was performed using the free statistical package G*Power 3. The calculation was based on our pilot test. Eleven participants (six participants in the PSSE group and five participants in the SSE group) took part in the pilot test, which was used to determine the number of participants needed for this study (mean difference, 9.90%; standard deviation, 4.52%; effect size, 1.28). The results of the pilot test indicated that at least nine participants per group would be required to detect a difference in concentric external rotation (ERc) peak moment/body weight (PM/BW) between groups using a one-tailed test with a power of 0.80% and an
Inclusion criteria included scapular dyskinesis, pain caused by or increasing during baseball games or training, and more than 15
Following the block randomization method, a study assistant who was not involved in the baseline evaluation results and interventions randomly assigned participants to a group. The block randomization method was used to ensure that two groups had an equal number of members. Participants picked a single card without looking from a swathed set of two cards marked with P or S (P card, PSSE group; S card, SSE group). Because the same examiners were involved in both outcome determination and intervention, they were not blind to the group allocations; however, participants were not informed of their group assignment or the aim of the study.
Procedures and instrumentation
Scapular dyskinesis
The disorder was identified through the following test: Beginning in a standing position, participants were asked to elevate their arms with 3-kg or 1.5-kg dumbbells in their hands, with their thumbs up to the end position over a period of 3 s, and then to lower their arms to the initial position in 3 s. The examiner classified the scapular positions and movement patterns during arm movement [14] (Table 2).
Isokinetic testing
RC muscle strength was measured only dominant shoulder with scapular dyskinesis using a Biodex System 4 dynamometer (Biodex Corp., Shirley, NY, USA). Participants completed 3–5 submaximal contraction trials to become familiar with the procedure and to warm up their muscles. The test was performed in a supine hook-lying position; straps were placed on the shoulder girdle and trunk to prevent compensation. Participants were asked to abduct the shoulder to 90
Rotational RoM
GH joint ROM was measured by two examiners by determining IR and ER ROM using the bubble goniometer [30, 42]. The goniometer axis was positioned over the olecranon process, with the stationary arm aligned perpendicular to the ground and the moveable arm aligned along the ulnar styloid process [42]. IR was permitted until the participant’s coracoid was felt rising into the examiner’s thumb, and then the motion was stopped. ER ROM was measured by passive external rotation until the end range was reached. GIRD was calculated based on the difference in IR ROM between the throwing shoulder and the non-throwing shoulder.
Shoulder pain
Shoulder pain was evaluated using a visual analog scale (VAS) [2].
Sleeper stretch. A, Start position. B, End position.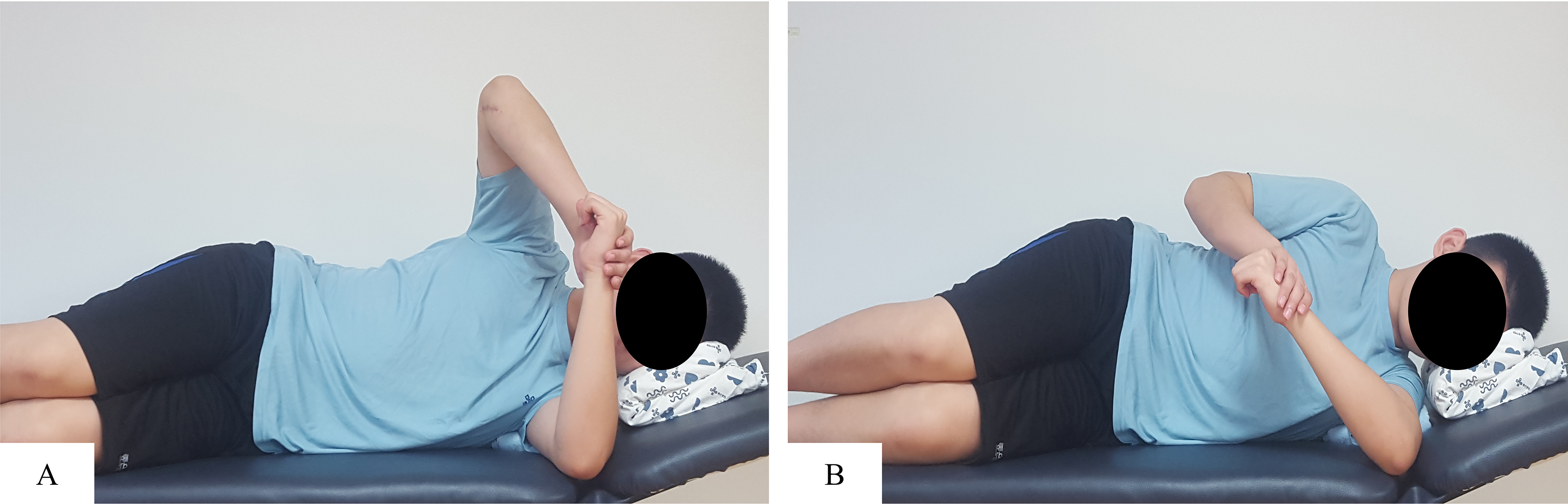
Scapular stabilization exercise. A, Punch exercise. B, Forward flexion (FF) in a side-lying position. C, Prone horizontal abduction (PHA). D, Prone extension (PE).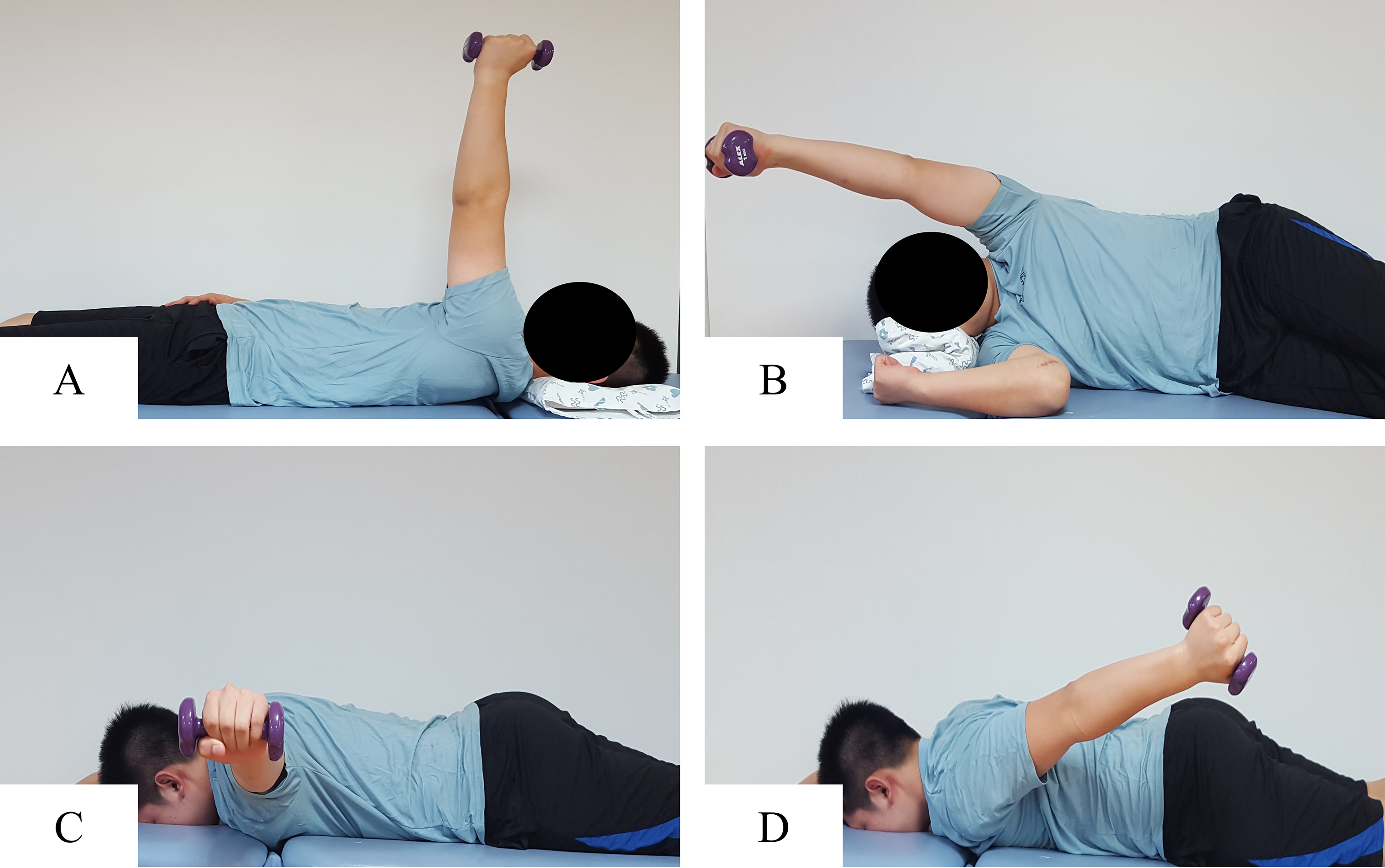
Isokinetic strength test of RC muscle. A, Start position. B, External rotation 50
The PSSE group performed the sleeper stretch with four SSE over 6 weeks: a punch exercise, forward flexion (FF) in the side-lying position, prone horizontal abduction (PHA), and prone extension (PE). The SSE group performed four SSE without stretching for 6 weeks. The sleeper stretch was performed to improve the flexibility of the posterior shoulder muscle and soft tissue [16, 20, 23, 26, 27]. Participants began in a side-lying position on the floor with the throwing shoulder below, flexed to 90
Outcome measures
The isokinetic outcome measures consisted of the PM/BW of the IR, in the concentric and eccentric mode – IRc and IRe respectively and the corresponding values for external rotation: ERc and ERe. The DCR comprised of two variants: DCRi-e
Statistical analysis
Statistical analyses were performed with SPSS software (ver. 18.0 for Windows; SPSS Inc., Chicago, IL USA). Two-way repeated-measures analysis of variance (ANOVA) was used to determine the time-by-group interaction effect or the main effect for time. The within-group factor was time (pre-intervention versus post-intervention) and the between-group factor was group (PSSE group vs. SSE group). When significant main effects or time-by-group interaction effects were found, post hoc
Demographic characteristics of the participants
Demographic characteristics of the participants
Values are mean
Classification of the main patterns of scapular dyskinesis
Isokinetic PM/BW and DCR pre- and post-intervention
Values are mean
G.H joint ROM and pain pre- and post-intervention
Values are mean
All twenty-four enrolled participants completed the follow-up. All participants denied any adverse (
A significant time-by-group interaction effect was observed for the ERc (
A significant time-by-group interaction effect was observed for IR ROM (
There was no significant time-by-group interaction effect for pain (
Discussion
We investigated the effects of PSSE over 6 weeks on RC muscle strength, DCR, ROM, and pain in adolescent baseball players with scapular dyskinesis. Our results showed significantly decreased pain in both the PSSE and SSE groups. However, RC muscle strength, DCR, and ROM improvements were observed only in the PSSE group.
The PSSE group showed improvements in the ERc and ERe PM/BW; there are several possible reasons for the increased muscle strength. First, the restoration of flexibility affects the length-tension relationship and produces muscle force [31]. Altered muscle length affects the joint kinematics-muscle activation relationship and can produce a certain degree of muscle force [12]. We observed increased IR ROM in the PSSE group, indicating restored flexibility in posterior shoulder muscles and soft tissue [20, 26, 27]. This increases the length-tension relationship and activation of the ER muscle, and may have increased the ERc and ERe PM/BW in this study. Second, increased muscle tension over time may have affected our results. Stretching increases relaxation and reduces muscle tone over time. This leads to increased muscle length and viscoelastic properties, ultimately increasing muscle force production [37]. A 6-week intervention period was applied in this study. There was a greater increase in the ER muscle length and viscoelastic properties post-intervention in the PSSE group, which would have resulted in increased ERc and ERe PM/BW. Previous researchers have reported the long-term effects of stretching on ROM and strength. Worrell et al. [44] reported 8.5% and 13.5% increases in eccentric PM of the hamstring muscle measured at 60
The increased ER PM/BW observed in our study may have affected the DCR results. Our DCR results showed a significantly increased ERe to IRc ratio and decreased IRe to ERc ratio post-intervention in the PSSE group. Previous authors have reported that a lower ERe to IRc ratio predisposes individuals to throwing shoulder injuries [7, 34, 39]. Therefore, PSSE intervention may inhibit the distractive force in the deceleration phase and prevent such injuries. The reduction in the IRe to ERc ratio can be explained by the increased strength of the ERc PM/BW.
IR ROM significantly increased and ER ROM and GIRD significantly decreased post-intervention in the PSSE group. GIRD has been closely related to the pathologic changes and shoulder dysfunction in younger throwing athletes [15, 16, 35]. Shanley et al. [35] found that high school baseball players with
The VAS score was significantly lower post- intervention in both the PSSE and SSE groups. Our results may be closely related to the dynamic stability of the humeral head provided by the ER muscles during throwing. Throwing-related pain inhibits the ER muscle, leading to ERe weakness, as observed in previous studies [7, 28, 34, 39]. The ER muscle plays an important role in providing the dynamic stability of the humeral head. Therefore, increased ERc and ERe PM/BW after 6 weeks of PSSE intervention would have increased the dynamic stability of the humeral head during throwing and decreased the VAS score in the PSSE group. The SSE program focused on LT, MT, and SA strengthening exercises to restore scapular kinematics. De Mey et al. [9] reported significantly reduced UT activity and increased LT and MT activity, as well as an earlier LT and SA onset than UT after a 6-week SSE program. Cools et al. [8] observed a significantly increased LT/UT and MT/UT ratio during SSE. Lynch et al. [25] also reported that LT, MT, and SA strengthening exercises for 12 weeks significantly increased the LT, MT, and SA strength. Although we did not evaluate scapular kinematics, it appears that scapular stabilizer muscle balance increased after 6 weeks in the SSE group. Thus restoring normal scapulohumeral rhythm may reduce throwing-related pain.
The present study had several limitations. First, we did not evaluate scapular kinematics. Thus, we could not its effect on RC muscle strength. Future studies are hence needed to investigate the effects of PSSE and SSE on scapular kinematics and the relationship between scapular kinematics and dynamic strength in the RC muscle. Second, we did not evaluate RC muscle activity. Therefore, we could not confirm differences in RC muscle strength due to muscle activity changes; therefore, we recommend future studies to fill this gap. Finally, since the intervention effect was compared only in the dominant shoulder with scapular dyskinesis in this study, it is unclear whether there is a difference in intervention effect compared to the non-dominant shoulder.
Conclusion
Both PSSE and SSE interventions led to more pain relief. However, only the PSSE group showed improvements in ROM, ERc, ERe PM/BW, and DCR. These results suggest that PSSE intervention is a more effective program for improving RC muscle strength and balance, particularly concentric and eccentric ER muscle strength and the ERe to IRc ratio, in adolescent baseball players with scapular dyskinesis.
Footnotes
Acknowledgments
This work was supported by the 2017 Inje University research grant.
Conflict of interest
All authors have completed the ICMJE uniform disclosure form and no conflicts of interests were reported for this study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.