
Abstract
BACKGROUND:
Little is known regarding the influence of force application during fatigue when the total amount of work is equal. That is, do changes in force applications result in different fatigue mechanisms despite the overall work being the same.
OBJECTIVE:
The aim of the current study was to examine the effects of alternating forces versus repeated constant force muscle actions on the time course of changes in neuromuscular responses.
METHODS:
Sixteen adults performed 50-intermittent isometric leg extensions at alternating 40 then 80% maximal voluntary isometric contraction (40/80% MVIC) or repeated constant forces at 60% MVIC. Each protocol resulted in equal, averaged force across all 50 repetitions. Electromyographic amplitude (EMG RMS), mechanomyographic (MMG) RMS, EMG mean power frequency (MPF), and MMG MPF were recorded from the vastus lateralis.
RESULTS:
Alternating force protocol resulted in less fatigue-induced changes in neuromuscular responses compared to repeated constant force protocol. The repeated constant force protocol resulted in earlier increases in EMG RMS and MMG RMS as well as earlier decreases in EMG MPF and MMG MPF compared to the alternating force protocol.
CONCLUSIONS:
Fatigue in occupational, sporting activities, or various fatiguing tasks may be dependent on the order that force is applied.
Introduction
Fatigue has been defined as a “…gradual decrease in the force capacity of muscle or the endpoint of a sustained activity, and it can be measured as a reduction in muscle force, a change in electromyographic (EMG) activity or an exhaustion of contractile function” [1, p. 12]. The amplitude of the EMG signal represents muscle activation, and the frequency content is related to motor unit action potential conduction velocity during isometric muscle actions [2, 3, 4, 5]. The mechanomyographic (MMG) signal, however, reflects the mechanical counterpart of the motor unit electrical activity as measured by EMG and quantifies the low-frequency lateral oscillations of activated skeletal muscle fibers [5, 6, 7]. Under some conditions, the amplitude of the MMG signal represents motor unit recruitment, and the frequency content is qualitatively related to the global firing rates of unfused, activated motor units [6, 7]. Therefore, simultaneous assessments of EMG and MMG signals have been used to examine fatigue-related neuromuscular responses and make inferences regarding motor unit activation strategies including muscle activation [2], motor unit action potential conduction velocity [2], motor unit recruitment [6, 7], and global motor unit firing rate [6, 7, 8] from the time-dependent changes in EMG amplitude, MMG frequency, MMG amplitude, and MMG frequency, respectively.
Most occupational and sporting activities involve complex motor programs that often include randomly ordered levels of force production, rest intervals, number of repeated contractions, durations of recovery, modes of muscle actions, and multiple muscle groups [9, 10]. The interactions among these factors can affect force-related outcomes during fatiguing tasks as well as the patterns of responses for EMG and MMG time and frequency domain parameters [11, 12, 13]. To understand the time course of neuromuscular responses that describe the process of fatigue, most studies have assessed these neuromuscular responses while manipulating one or more of the influencing factors (i.e. force production and/or rest intervals), and controlling others (i.e. mode of muscle action and/or the muscles involved) [11, 14, 15]. For example, Kouzaki et al. [14] reported decreases in EMG amplitude, EMG frequency, MMG amplitude, and MMG frequency from the vastus lateralis (VL), vastus medialis (VM), and rectus femoris (RF) muscles following 50 maximal, intermittent isometric muscle actions of the leg extensors. Bigland-Ritchie et al. [15], however, reported decreases in maximal voluntary isometric contraction (MVIC) torque, but increases in EMG amplitude from the VL following 10-min of submaximal, intermittent isometric muscle actions of the leg extensors at 50% MVIC. In addition, previous studies [12, 13] have shown that the time course of changes in neuromuscular responses are intensity-specific and may provide insight regarding the motor unit activation strategies used to maintain force production throughout the process of fatigue. For example, Smith [13] reported different time course of changes in EMG amplitude, MMG amplitude, EMG frequency, and MMG frequency from the VL, VM, and RF during dynamic constant external resistance leg extension muscle actions to failure at low (30% 1 repetition maximum [1-RM]) versus high force levels (70% 1-RM). Yung et al. [16] performed various muscle actions consisting of sustained, intermittent, and sinusoidal muscle actions from the lateral and medial heads of the triceps that all averaged to 15% MVIC force and found unique neuromuscular fatigue characteristics even though they all had the same averaged work. No previous studies, however, have simultaneously measured EMG amplitude, MMG amplitude, EMG frequency, and MMG frequency to examine the time course of changes in these neuromuscular parameters during repeated muscle actions at the same force versus alternating low and high force intermittent isometric muscle actions. Therefore, the purpose of the present study was to examine the effects of repeated muscle actions at 60% MVIC versus alternating muscle actions at 40 and 80% of MVIC on the time course of changes in neuromuscular responses during fatiguing, intermittent isometric muscle actions of the leg extensors. Based on previous studies [12, 13, 16, 17], we hypothesized that alternating force at 40 then 80% MVIC would result in less fatigue-related changes in these neuromuscular parameters compared to repeated muscle actions at 60% MVIC during intermittent isometric muscle actions.
Materials and methods
Subjects
Sixteen healthy adults (11 men and 5 women, mean
Orientation session
The orientation session was used to familiarize the subjects with the testing procedures including maximal and submaximal isometric muscle actions of the leg extensors. All isometric muscle actions were performed using the dominant leg (based on kicking preference) at a knee joint flexion angle of 60
Intermittent isometric protocols
A warm-up consisting of 5-min on a cycle ergometer at a self-selected resistance was performed prior to each testing session. In addition, the subjects performed 5 submaximal isometric muscle actions of the leg extensors at approximately 50% of their maximum effort, followed by 2-min of rest. After the warm-up, 2, 6-s MVICs were performed with a 2-min rest after each MVIC before performing one of the randomly ordered intermittent isometric protocols. At least 48-hrs were allowed between each of the intermittent isometric protocols. The highest MVIC torque value on the second visit (immediately prior to the first intermittent isometric protocol) was used to determine the torque values at 40, 60, and 80% MVIC for both intermittent isometric protocols.
Depiction of the 60% and 40/80% maximal voluntary isometric contraction (MVIC) protocols. Each protocol consists of 50 intermittent isometric muscle actions of the leg extensors with equal average load.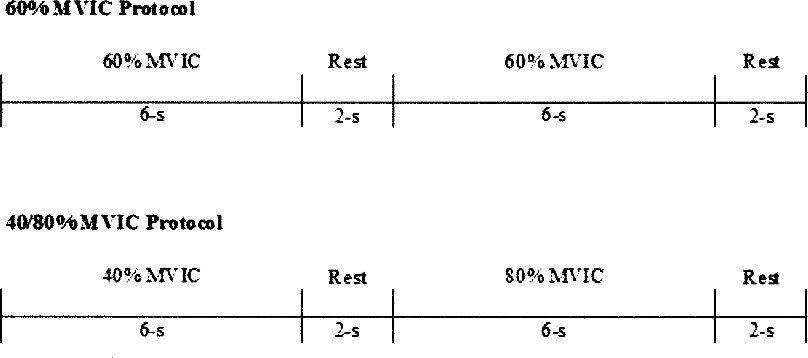
The 60% MVIC protocol consisted of 50, 6-s intermittent isometric muscle actions of the leg extensors followed by 2-s of rest (6:2 work to rest ratio) at 60% MVIC (totaling 50 repetitions at 60% MVIC each separated by 2-s of rest). The 40/80% MVIC protocol consisted of 50, 6-s intermittent isometric muscle actions of the leg extensors beginning with a 6-s repetition at 40% MVIC with 2-s of rest followed by a 6-s repetition at 80% MVIC with 2-s of rest. This alternating pattern continued until 50 repetitions were performed (totaling 25 repetitions at 40% MVIC and 25 repetitions at 80% MVIC each separated by 2-s of rest) (Fig. 1). The 60% MVIC and 40/80% MVIC protocols performed equal, averaged load across the 50 repetitions: (60% MVIC
A bipolar (20 mm inter-electrode distance) surface electrode (circular 4 mm diameter silver/silver chloride, BIOPAC Systems, Inc., Santa Barbra, CA) arrangement was placed over the VL of the dominant thigh according to the recommendations from SENIAM [19] and Barbero et al. [20]. The skin was dry shaven, abraded, and cleaned with rubbing alcohol prior to the placement of electrodes. The bipolar electrode arrangement over the VL was placed 33% the distance between the lateral side of the patella and the anterior superior iliac spine, orientated 20
The MMG signals were detected from the VL using a miniature accelerometer (Measurement Specialties EGAS-FT 10, bandwidth 0–200 Hz, dimensions: 1.0
A) Mean and standard error (SE) for the time course of changes in electromyographic (EMG) and mechanomyographic (MMG) amplitude (root mean square; RMS) and frequency (mean power frequency; MPF) during averaged 25 intermittent isometric muscle actions at 60% maximal voluntary isometric contraction (MVIC). B) Shows the results of the polynomial regression analyses as well as significant values from the ANOVA with post-hoc student Newman-Keuls tests. Solid lines and their associated * (X to X) * Indicate the repetition range and neuromuscular parameter that was significantly different from repetition initial repetition of each neuromuscular parameter (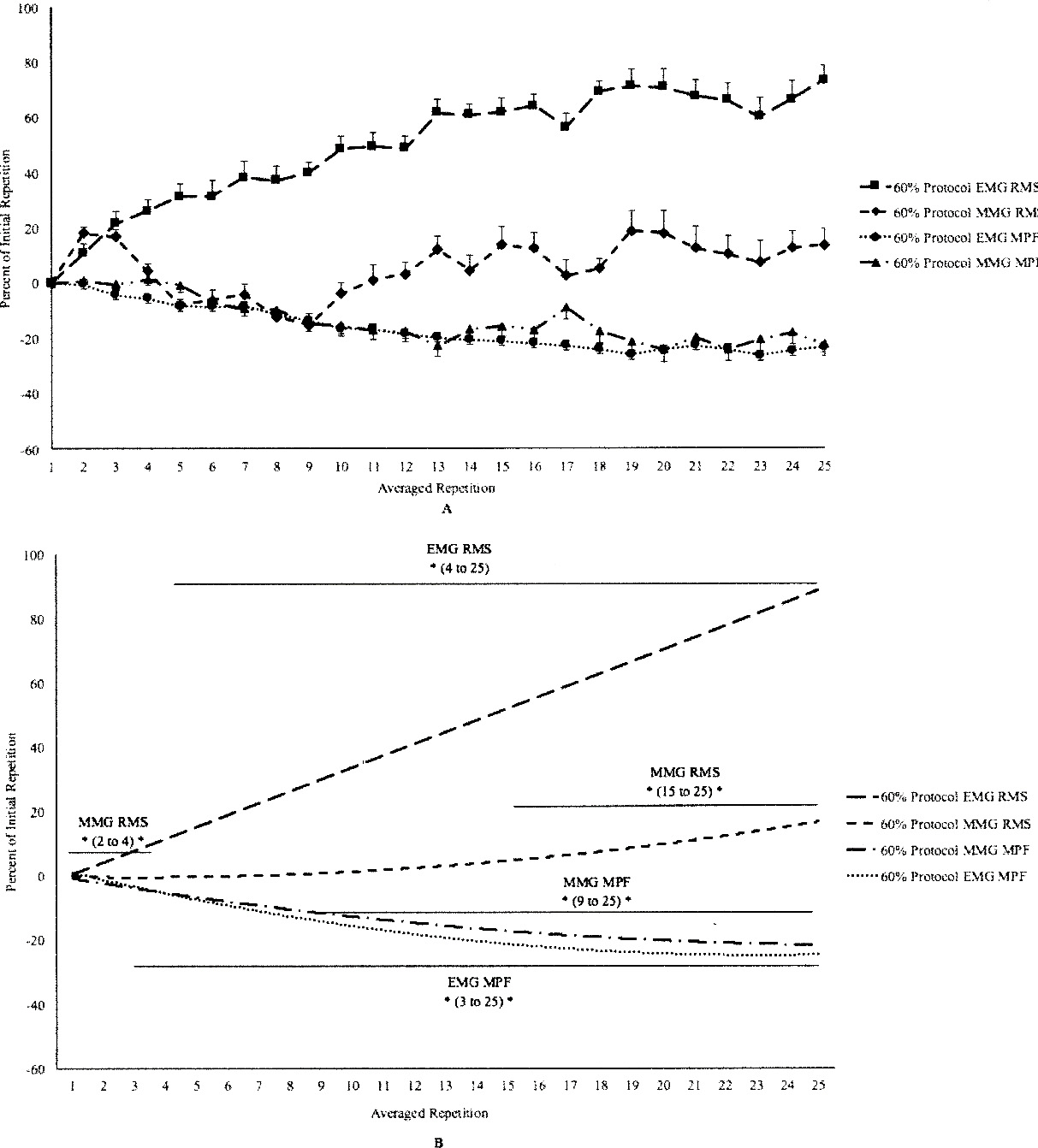
The raw EMG and MMG signals were digitized at 2 kHz with a 16-bit analog-to-digital converter (Model MP150, BIOPAC Systems, Inc., Santa Barbra, CA) and stored in a personal computer for subsequent analysis. All signal processing was performed using custom programs written with LabVIEW programming software (Version 13.0, National Instruments, Austin TX). The EMG amplitude (root mean square; RMS, EMG mean power frequency (MPF), MMG RMS, and MMG MPF values were calculated from 2-s epochs corresponding to the middle 33% of each repetition. All subjects submaximal EMG RMS, EMG MPF, MMG RMS, and MMG MPF values were normalized as a percentage (%) of each subjects initial averaged repetition. In addition, the EMG RMS, EMG MPF, MMG RMS, and MMG MPF values from 2 consecutive repetitions were averaged (i.e. repetitions 1 and 2 were averaged, then repetitions 3 and 4 etc., totaling 25 averaged repetitions) so the total torque production for each average of 2 repetitions was 60% MVIC. That is, for the 60% MVIC intermittent isometric protocol, repetitions 1 and 2 were both equal to 60% MVIC (60% MVIC
A) Mean and standard error (SE) for the time course of changes in electromyographic (EMG) and mechanomyographic (MMG) amplitude (root mean square; RMS) and frequency (mean power frequency; MPF) during averaged 25 intermittent isometric muscle actions at 40/80% maximal voluntary isometric contraction (MVIC). B) Shows the results of the polynomial regression analyses as well as significant values from the ANOVA with post-hoc student Newman-Keuls tests. Solid lines and their associated * (X to X) * Indicate the repetition range and neuromuscular parameter that was significantly different from repetition initial repetition of each neuromuscular parameter (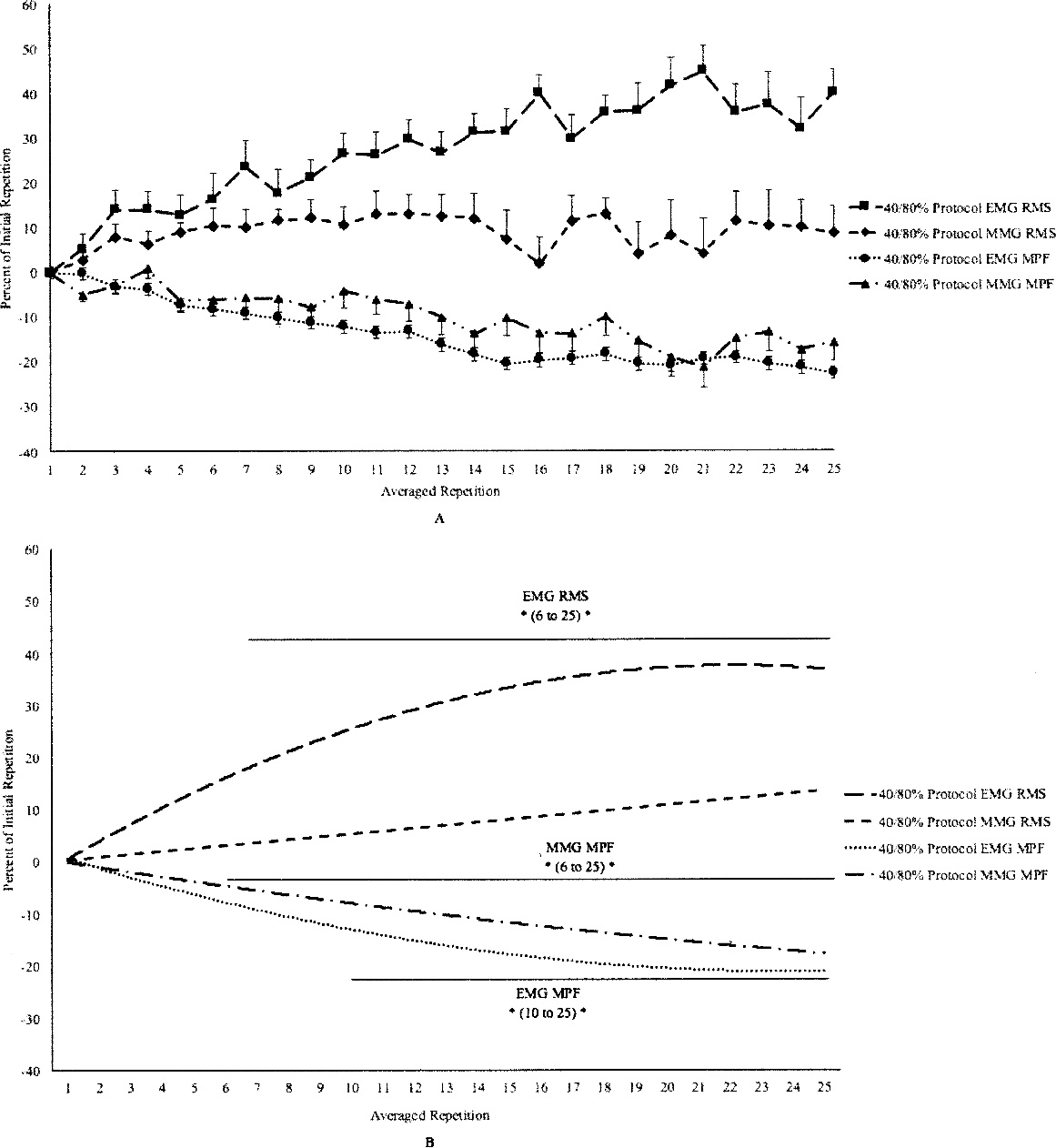
All analyses were performed on the composite of all subjects. Polynomial regression analyses were used to determine the patterns (i.e. linear, quadratic, or cubic) for the mean, normalized (% of initial repetition) EMG RMS, EMG MPF, MMG RMS, and MMG MPF versus repetition relationships for the 60 and 40/80% MVIC protocols. The time course of changes in EMG RMS, EMG MPF, MMG RMS, and MMG MPF for both the 60 and 40/80% MVIC protocols were identified by one-way repeated measures ANOVA 1 (neuromuscular parameters [EMG RMS, MMG RMS, EMG MPF, MMG MPF])
Results
60% MVIC protocol time course of changes
Figure 2A and B show the results of the polynomial regression analyses and one-way repeated measures ANOVAs with post-hoc Student Newman-Keuls tests for the normalized EMG RMS (
40/80% MVIC protocol time course of changes
Figure 3A and B show the results of the polynomial regression analyses and one-way repeated measures ANOVAs with post-hoc Student Newman-Keuls tests for the normalized EMG RMS (
Discussion
Time course of changes in neuromuscular responses
The time course of changes in neuromuscular responses were different between the 60% and 40/80% MVIC protocols (Fig. 2A and B). The initial increase then decrease from MMG RMS in the first 8 averaged repetitions were unique responses which may be explained by changes in the post-activation potentiation [17]. For example, Sonne and Potvin [17] suggested that during the first cycles of an intermittent muscle action post-activation potentiation may affect force production under certain conditions. Thus, potentially altering the motor unit activation strategies used to maintain the required force production during the beginning of an intermittent work bout. The 40/80% MVIC protocol had less pronounced changes in neuromuscular responses compared to the 60% MVIC protocol (Fig. 3A and 3B). That is, there were no changes in any of the neuromuscular parameters during the first 5 averaged repetitions in the 40/80% MVIC protocol. In addition, the 40/80% MVIC protocol had less pronounced fatigue-related changes in the neuromuscular parameters during the 25 averaged repetitions (Figs 2B and 3B). Thus, the patterns of fatigue-related neuromuscular responses during these alternating and constant force muscle actions were different than those reported by previous studies which examined intermittent [12, 14, 23, 24] or sustained [25, 26, 27] isometric muscle actions at various intensities. For example, Smith et al. [12] reported quadratic and linear increases in EMG RMS and MMG RMS, respectively, from the VL which began at repetition 5 and continued throughout the 50 intermittent isometric muscle actions at 60% MVIC. Smith et al. [12] also reported quadratic decreases in EMG MPF and MMG MPF from the VL which began at repetition 20 and continued throughout the fatiguing work bout. Kouzaki et al. [14], however, reported decreases from the VL, VM, and RF muscles for EMG amplitude, MMG amplitude, EMG median frequency, and MMG median frequency which began at repetition 5, plateaued at repetitions 40, 35, 15, and 20, respectively, and continued to the end of the 50 maximal, intermittent, isometric muscle actions. Thus, the findings of the current investigation, in conjunction with previous studies [12, 14], indicated that the time course of changes in these neuromuscular responses were intensity-specific during intermittent isometric muscle actions as well as sensitive to differences in the way in which force was applied when equal, averaged force was performed (i.e. repeated force at 60% MVIC versus alternating forces at 40% then 80% MVIC).
60% versus 40/80% MVIC protocol
Both protocols (60% and 40/80% MVIC) resulted in decreases in EMG MPF, however, the time course of changes suggested that the 60% MVIC protocol began to manifest fatigue-related decreases before the 40/80% MVIC protocol. During the 60% MVIC protocol, EMG MPF decreased significantly from the initial repetition at repetition 3 compared to repetition 10 during the 40/80% MVIC protocol (Figs 2B and 3B). The earlier decrease in EMG MPF suggested a more rapid buildup of metabolic byproducts, perhaps due to greater blood flow occlusion [28, 29, 30]. For example, Cayot et al. [31] found less blood flow occlusion in the VL at 20 and 40% MVIC than at 60 and 80% MVIC muscle actions.
The present study indicated that alternating forces (40/80% MVIC) resulted in less pronounced fatigue-related changes in neuromuscular responses than repeated muscle actions at the same force (60% MVIC) when equal, averaged force was maintained throughout the fatiguing work bout. Specifically, the 60% MVIC protocol exhibited earlier and greater increases in EMG RMS and MMG RMS as well as an earlier decrease in EMG MPF than the 40/80% MVIC protocol. These findings were similar to those reported by Yung et al. [16] who indicated that sustained, intermittent, and sinusoidal muscle actions each exhibit unique neuromuscular and fatigue-related responses from the elbow flexors although all protocols averaged 15% MVIC. During the 40/80% MVIC protocol, in the current study, there was an earlier decrease in MMG MPF compared to the 60% MVIC protocol. The earlier increase in EMG RMS during the 60% MVIC protocol (repetition 4) compared to the 40/80% MVIC protocol (repetition 6) suggested that an earlier increase in muscle activation was required during the repeated muscle actions at the same force compared to the alternating force muscle actions. In addition, EMG RMS increased by approximately 85% throughout the fatiguing work bout at 60% MVIC, but only 40% for the 40/80% MVIC protocol. Furthermore, the EMG RMS during the 40/80% protocol plateaued from approximately repetitions 19 to 25, which suggested that no further increases in muscle activation were required to maintain the alternating force protocol. The EMG RMS during the 60% MVIC protocol, however, increased linearly to the end of the fatiguing work bout which suggested that with each repetition there was an increase in the muscle activation required to maintain the repeated muscle actions at the same force. Fatigue-related increases in the amplitude of the EMG signal (EMG RMS) are associated with increases in motor unit recruitment, firing rate, and/or synchronization [2, 32]. Furthermore, MMG RMS reflects motor unit recruitment, while MMG MPF qualitatively reflects the global firing rate of the activated motor units. In the present study, EMG RMS increased during both fatiguing protocols, but MMG RMS, increased only during the 60% MVIC protocol. Thus, the increases in EMG RMS and MMG RMS, but decrease in MMG MPF during the 60% MVIC protocol suggested that the increase in muscle activation was likely due to increases in motor unit recruitment and/or synchronization, but not the global motor unit firing rate. The increase in EMG RMS and decrease in MMG MPF, without a change in MMG RMS during the 40/80% MVIC protocol, however, suggested that the increase in muscle activation was likely due to an increase in synchronization to provide efficient force production during the development of fatigue [33] and not motor unit recruitment or global firing rate.
The current study has potential limitations that need to be considered which include the unique measurement characteristics associated with the collection of the EMG and MMG signals as well as potential differences in the metabolic cost of each averaged 40/80% and 60% MVIC muscle action. For the EMG signal, there are conflicting reports regarding if the EMG amplitude and force relationship is linear or non-linear. In general, there is agreement that EMG amplitude increases with an increase in force, however, some studies have reported a non-linear relationship while others have indicated a linear relationship [34, 35, 36]. The majority of studies, however, have reported a linear relationship for EMG amplitude and force. In addition, it has been suggested [35] that the VL exhibits the most reliable and reliable EMG/force relationship values. It has been reported that increases in MMG amplitude occurs up to 70–100% MVIC [34, 37, 38]. Thus, it is likely that 80% MVIC muscle actions exhibited greater MMG amplitude values compared to the 40 and 60% MVIC muscle actions. In addition, this study did not measure the metabolic cost for the 40/80% or 60% MVIC protocol. Therefore, it is plausible that there were differences in the metabolic cost for performing different intensity muscle actions. Although, it has been reported that isometric leg extensions at low and high stimulated frequency resulted in comparable metabolic costs regardless of intensity [39].
In summary, the 60% MVIC protocol resulted in more pronounced fatigue-related responses than the 40/80% MVIC protocol. The 60% MVIC protocol was characterized by earlier and greater increases in EMG RMS and MMG RMS, as well as earlier decreases in EMG MPF. The differences between protocols in the patterns of timing of neuromuscular responses may have been due to less blood flow occlusion and, therefore, less fatigue-related buildup of metabolic byproducts during the 40/80% MVIC protocol. Both protocols, however, exhibited decreases in MMG MPF which suggested fatigue-related reductions in the global motor unit firing rate of the activated motor units to provide an economical activation of the muscle. Thus, the current findings suggested that the alternating force production protocol (40/80% MVIC) may exhibited less pronounced fatigue-related characteristics than repeating contractions at the same level of force (60% MVIC).
Conflict of interest
None of the authors have anything to disclose.