
Abstract
BACKGROUND:
The high variability in muscle performance, especially in muscle strength, typical of people with multiple sclerosis (PwMS) implies that in order for strength variations to be clinically interpretable, the extent of variability should be properly quantified.
OBJECTIVE:
To establish the responsiveness of maximal isokinetic strength measurements obtained from the ankle dorsiflexors of PwMS and of a cohort of matched healthy controls.
METHODS:
Twenty PwMS and 20 healthy controls participated in this study. All subjects underwent a dedicated familiarization session and then three isokinetic testing sessions (Test 1; 1-day retest; 1-week retest) in which the peak moment (PM) and maximal work (MW) were recorded in the more affected side.
RESULTS:
PwMS proved significantly weaker than controls (
CONCLUSIONS:
The responsiveness of the strength and work findings in this cohort indicates that isokinetic measurements of dorsiflexion performance in PwMS may effectively be employed for detecting the efficiency of an intervention in spite of the fluctuating nature of this disease.
Keywords
Introduction
Reproducibility and responsiveness are two closely related methodological properties of clinical measurements [2]. Reproducibility, also known as test-retest reliability, is the ability to measure attributes in a consistent manner when administered on several occasions [2]. Responsiveness is the ability to detect relevant changes over time [13]. The recent decade saw a significant shift towards the preferential employment of the latter in rehabilitation research. This trend reflects the growing understanding that more than assessing the stability of a trait or a test measure, what is needed is a decision rule for assessing the efficiency of an intervention. Such a decision rule, which inevitably incorporates an element of reproducibility, is expressed by a number, termed the ‘cutoff score’. This score differentiates a meaningful change in performance from a non-meaningful one, even if statistically significant, which falls within the so-called error zone. The error (or measurement error) reflects the cumulative effect of of the ‘subject/patient’, ‘examiner’, ‘test instrument’, ‘protocol’, and the ‘test environment’ factors [27, 35]. One of the most common indicators of responsiveness is the smallest real difference (SRD). Significantly, if following an intervention, a change in an outcome parameter (OP) relative to the baseline level exceeds the SRD, this change is considered clinically important, otherwise the apparent ‘change’ carries no clinically meaningful value. Obviously, a higher reproducibility (e.g. higher intraclass correlation coefficients, ICCs) contributes to better responsiveness (e.g. lower SRD) but the relationship is not 1:1. Furthermore, the analysis of the responsiveness of relevant OPs is essential for assessing the efficiency of clinical interventions and for developing new evaluation methods.
These considerations are particularly pertinent for evaluating muscle performance in conditions characterized by high variability and inconsistent responses to an intervention such as those occurring in patients with multiple sclerosis (PwMS). These patients are characterized by fluctuations in their compromised muscle mechanical function (muscle strength, muscle power, explosive muscle strength and increased fatigability) [15, 19, 30], due to their impaired ability to fully activate the tested muscles [17, 32]. It has been proposed that quantitative assessment of muscle performance in PwMS may be biased by daily variability in strength or fatigue [18, 31].
The reproducibility of muscle performance findings in PwMS has been the topic of a few studies which reported excellent test-retest reproducibility of strength and fatigue parameters [3, 18, 27, 32]. However, all these studies: i) related mainly to ICCs, which are known to be insensitive to changes that occur within a group in a uniform mode [29]; ii) limited the basis for estimating reproducibility to two time points (test and retest) only, although the inclusion of a third time point in a non-consecutive day has been shown in different patient populations to portray this trait in a more clinically meaningful way [39]; iii) did not perform responsiveness analysis.
These shortcomings have motivated the present investigation, which focused on the responsiveness of isokinetic strength and work parameters of the ankle dorsiflexors in PwMS and in a matched cohort of healthy subjects, at 3 different time points. The ankle dorsiflexors were chosen as they are one of the most common sites of weakness in neurological conditions, particularly, in MS [40]. Therefore, the primary aim of the study was to establish cut-off values for clinically meaningful changes relating to the performance of the dorsiflexors in PwMS and healthy controls. In addition, the study characterized the dynamometric profile of the participants and explored any pattern of practice-based improvements [4].
Materials and methods
Subjects
This study is a continuation of a previously published single-system interventional case series of 8 PwMS [22], whose baseline assessments of isokinetic strength have been considered also for the current investigation. Twenty PwMS with predominantly unilateral muscle weakness of the dorsiflexors were recruited from those participating in a larger interventional trial taking place in the University Hospital facilities. Inclusion criteria were: diagnosis of relapsing-remittent MS according to 2010 revision of diagnostic criteria [28]; patient-reported evidence of strength asymmetry between dorsiflexor muscles; age
Measurements of ankle dorsiflexion muscles’ strength
Bilateral concentric assessment of ankle dorsiflexors was conducted by the same examiner at a consistent time of the day, using an isokinetic dynamometer (Biodex System 3, Biodex, Shirley, NY, USA). The test was conducted in the sitting position with the trunk inclined at 85
In the next formal familiarization session, which was aimed at controlling the potential learning effect of practice-based improvements [4], the position settings previously recorded were verified and the subject was required to perform 2 sets of 4 submaximal single concentric dorsiflexions, with the first set carried out at a comfortable, self-selected level of exertion, and the second set performed at a moderate effort. These procedures resembled those employed for the warm-up phase preceding the criterion strength test. As in the orientation session, participants were requested to monitor the force traces on the PC screen located in front of them. This session was aimed at controlling potential practice-based improvements [4].
Prior to the formal testing sessions, all subjects underwent a 5-minute warm-up by performing two sets of 2-to-4 concentric submaximal repetitions at 45
Demographic and clinical features of participants
Demographic and clinical features of participants
PwMS, patients with multiple sclerosis; Controls, healthy subjects; M, males; F, females; values are expressed as mean
Dynamometric features of the ankle dorsiflexion muscles by group, limb and testing session
LA, Less-affected limb; MA, Most-affected limb; DOM, Dominant; nDOM, non-dominant; PM, Peak Moment in Newton meter; MW, maximal Work in Joules; SD, Standard Deviation; C.I., Confidence Interval;
Statistical analysis was performed using the SPSS software (version 18) for Windows (SPSS Inc, Chicago, IL, USA). The highest PM value (in Nm) and MW value (in J) were recorded and used in the analysis. The MW/PM ratio was also calculated (in J/Nm). One-way ANOVA was employed to compare age, weight and the strength levels in the two groups. The Chi-square test was used to compare groups by gender. Means, standard deviations (SD) and 95% confidence intervals (CI) were calculated by side for PM and MW across the 3 testing sessions. Each OP was determined as the maximum value recorded among the tests. The equality of variances was assessed by the Levene’s test. A repeated-measures analysis of variance (ANOVA) was conducted to compare measurements among the sessions in the 2 groups to verify the repeatability of maximal isokinetic strength measurements in PwMS in comparison with healthy subjects. To control for any bias deriving from gender pooling, the strength levels were compared by two-way ANOVA between the groups with and without the male subjects. Significance was set at
Reproducibility and responsiveness of maximal strength measurements from the ankle dorsiflexion muscles by group, limb testing session
Reproducibility and responsiveness of maximal strength measurements from the ankle dorsiflexion muscles by group, limb testing session
LA, Less-affected limb; MA, Most-affected limb; DOM, Dominant; nDOM, non-dominant; PM, Peak Moment in Newton meter; MW, maximal Work in Joule; ICC, Intraclass Correlation Coefficient (two-way random); C.I., Confidence Interval; SRDi, Individual Smallest Real Difference; SRDi%, Individual Smallest Real Difference in percentage. SRDi absolute values follow the same unit of measurement of the relative outcome measure. All tests were conducted at 45
All participants completed the 3 testing sessions. All tests were well tolerated by the subjects and no exacerbation and/or injuries occurred in the PwMS group throughout the entire duration of the study. Demographic and clinical characteristics of the participants are detailed in Table 1.
No differences emerged between groups for age, weight, height and gender. Since no difference in isokinetic strength was detected between males and females within each group, pooled data are reported.
People with MS were significantly weaker than healthy controls in all OP, with strength deficits ranging 37–38% in PM and 42–55% in MW, at large to very large effect sizes (Cohen’s
No inter-side difference in strength was found in controls. In PwMS the more-affected limb was significantly weaker than the less-affected one both in PM (14.5%,
The MW/PM ratio was significantly higher (
Representative concentric ankle dorsiflexion moment-angular position (‘isokinetic strength’) curves obtained at an angular velocity of 45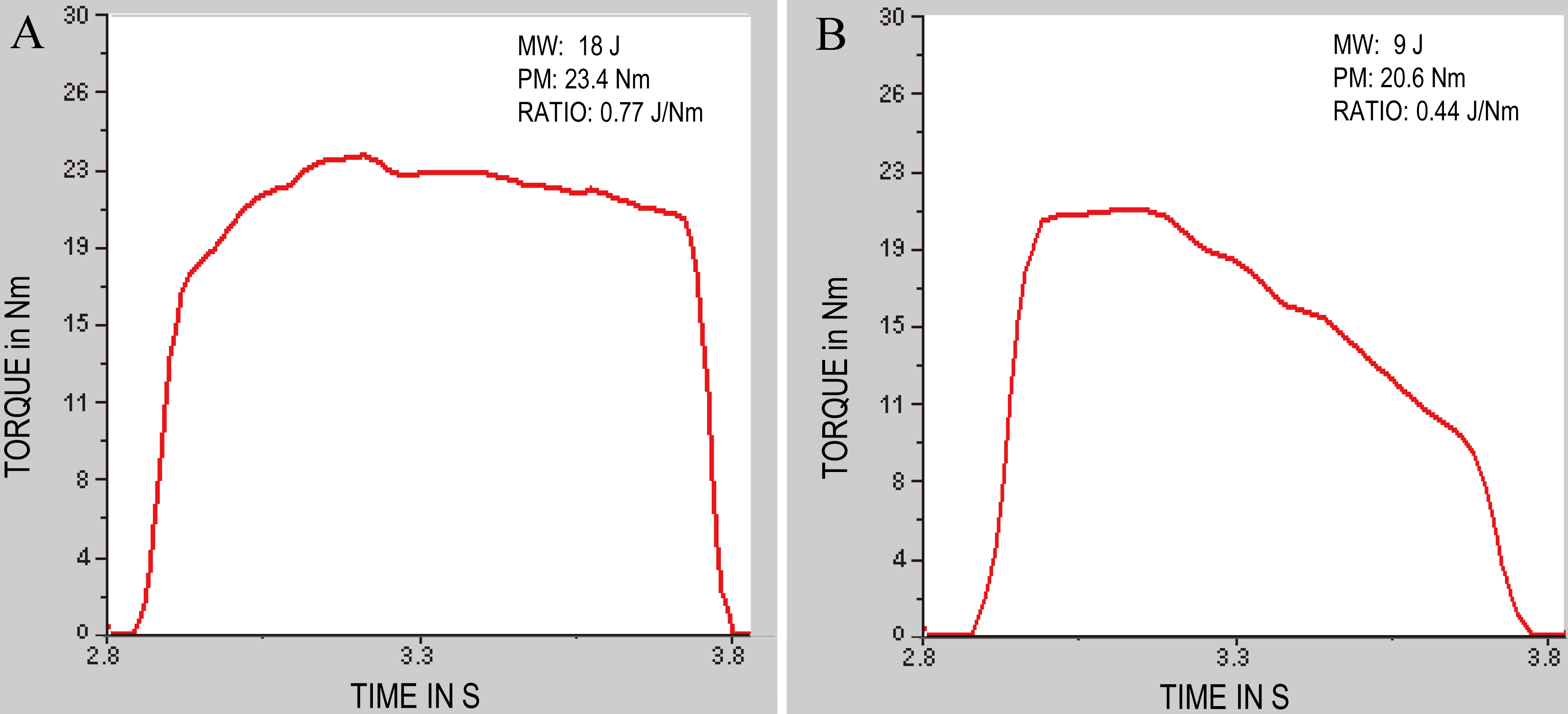
Descriptive statistics for the isokinetic findings of dorsiflexors’ strength are presented in Table 2.
The repeated-measures ANOVA, which was run separately for each group, revealed a main effect of the testing session in the PwMS group in both PM and MW. Bonferroni-adjusted pairwise comparisons detected significant reductions in both OP from the less-affected limb between sessions 1 and 2 (PM:
A main effect of the testing session was detected also in the control group. Pairwise comparisons revealed significant increases (8.4%) only in the non-dominant limb in PM between sessions 1 and 3 and in MW between sessions 1 and 2 and sessions 1 and 3, at small effect sizes (Cohen’s
The significant Session*Group interactions revealed that the temporal pattern of the changes over the 3 testing sessions was statistically different between the more-affected limb of PwMS and the non-dominant limb of controls (PM: F
Reproducibility and responsiveness
The values of the ICC (reproducibility) and responsiveness (SRDi and SRDi%) of the PW and MW measurements are detailed by group, limb and type of comparison in Table 3. Relative reproducibility analyses performed separately for females and males within each group revealed that the scores calculated for females only were very similar to the pooled data reported in Table 3. In detail, in female PwMS (
The SRDi values relating to the PM of both legs in PwMS were appreciably lower than their MW-related counterparts: 11.4 vs 13% and 19.4 vs 19.8%, respectively and even lower than the parallel scores calculated for the controls (13.8 vs 14.4%).
Discussion
The main finding of this study is that the responsiveness of maximal isokinetic performance of the ankle dorsiflexors in PwMS is clinically acceptable and hence may serve for the interpretation of the changes in strength observed following conservative interventions in this population that is characterized by high fluctuations in muscle performance [18].
General aspects
As expected, PwMS proved significantly weaker than controls, strongly supporting previous findings pointing to some 30–70% reduction in strength [26, 30, 32, 37]. On the other hand, the extent of asymmetry between the stronger and the weaker limb was differently portrayed by MW (significant inter-limb deficit of 20–24%) than by PM (non-significant inter-limb deficit of 12–14%). Linear correlation analysis showed that only 36–64% of the variability in one of these OPs is directly influenced by the other, suggesting that PM and MW relate differently to muscle function, echoing recent studies of the ankle dorsiflexors in healthy subjects both at baseline and after training [23, 24]. In particular, since MW represents the dissipated muscular output over the entire range of joint motion [25], adding it to the PM may complement the assessment of muscle performance in PwMS, who experience difficulties in maintaining the strength levels over distance and over time [30].
Furthermore, inspection of the morphology of the dynamometric curves and the calculation of the MW/ PM ratio revealed a significant difference between healthy subjects and PwMS. In the former, the MW obtained during a maximal dorsiflexion effort was 58% of the PM, while in the latter it was only 38%. These findings indicate that in PwMS the capacity of the dorsiflexors to sustain muscle tension over a given ankle range of motion is likely to be more affected than the ability to exert an instantaneous PM. It is worth noting that the analysis was based on the use of a relatively low angular velocity (45
Reproducibility over sessions
Reproducibility of PM and MW measurements, as assessed by ICC, proved excellent in PwMS and healthy subjects, regardless of gender. This general finding supports previous research relating to the ability of isokinetic dynamometry to yield clinically acceptable consistency of strength measurements in healthy subjects [12] as well as in PwMS under dynamic [17] and isometric conditions [3, 27, 32]. However, despite the high ICCs, significant inter-session differences were observed within each group, indicating that both PwMS and healthy controls performed differently depending on the time point of assessment. Despite the dedicated familiarization procedures, the two groups showed a different pattern of change across sessions, with strength increasing from session 1 to 2 in controls, while declining from session 1 to 3 in PwMS, in line with a recent single-system case series [22]. Even though a certain amount of practice-based improvement (
From a statistical standpoint, the results provided by the repeated-measures ANOVA and ICC analyses seem to be contradictory. Weir [38] suggests that an ICC can be large (indicating good reliability) while the ANOVA shows a significant trials effect. Indeed, as long as they are consistent across all the subjects (as indicated by all ICCs
Taken as a whole, the findings seem to confirm that, despite the employment of methodological procedures to optimize the consistency of the measurements, the assessment of maximal strength in PwMS is particularly challenging. Our cohort of PwMS achieved their peak performances in the first session, thus suggesting that one test may be sufficient to obtain valid findings. However, implementing 3 testing sessions revealed a trend of declining strength across sessions, which otherwise would have not been captured by a single test. Although the present study remains inconclusive as to how many tests are advisable for assessing PwMS, defining such variability across at least 3 sessions is a valuable information to adequately characterize the dynamometric profile of this population.
Responsiveness
Based on the results of the present study, any change in muscle performance falling below the individual cut-off value, expressed by SRDi, should be discarded even if statistically significant since it can be attributed to the measurement noise. This concept is particularly meaningful in terms of an intervention, since not every observed difference is clinically meaningful. Indeed, clinically meaningful improvements are at best no less than 10% and typically around 20–30% in orthopedic conditions [7], 26–55% in stroke survivors [20] and 11–39% in individuals with post-polio syndrome [10]. Importantly, the PM-based SRDi scores ranged 11.4–13% in PwMS and 13.8–14.4% in the controls, with the value for the more affected side in PwMS (13%) lower than the corresponding values for both the dominant and non-dominant sides in the controls. Noteworthy, in PwMS the PM-based SRDi scores were 40–50% lower than their MW counterparts, indicating that for these patients, a meaningful improvement in isokinetic strength could be detected relatively earlier by using the PM rather than the MW as the OP of choice. That said, the SRDi for MW for the ankle dorsiflexors in PwMS is coincident with what has been indicated as a clinically meaningful margin for real improvement in muscle function [8]. The findings thus indicate that in spite of inter-session differences in isokinetic strength and work capacity, the responsiveness of these measures is very well within clinically acceptable limits and may therefore serve for determination of clinically meaningful improvement or deterioration of these isokinetic markers, due to intervention or naturally occurring variations. Using the specific SRDi figures obtained in the ankle dorsiflexors of PwMS with same characteristics and measured isokinetically at relatively low velocities may practically translate into proclaiming that a change of slightly over 13% in the PM should be interpreted as clinically meaningful, thus informing a decision relating to the nature of the intervention.
In conclusion, measurements of maximal isokinetic concentric dorsiflexion strength obtained from PwMS proved to be highly reproducible, temporally unstable albeit in a clinically irrelevant manner but significantly well responsive to change. If the findings of this study are to be generalized to other muscle groups, contraction types and angular velocities, appropriate procedures should be instituted in PwMS when assessing physical capacities and/or the occurrence of meaningful changes that may be induced by rehabilitative interventions. These procedures should include methodological steps such as the inclusion of a proper familiarization protocol. Moreover, a comprehensive statistical approach should be employed in order to establish reproducibility and responsiveness of the measurements. Finally, the employment of the ANOVA for checking measurements’ stability over time and of the effect size for clinical relevance analyses may help to optimize the quantification and interpretation of test-retest results, which is particularly challenging in “unstable” individuals such as PwMS.
Study limitations
This study focused only on concentric testing. Eccentric measurements would have provided important information as lengthening contractions have a functional role in gait as well as in other functional activities. However, they were not included in order to keep the patients as mechanically unloaded as possible.
Another limitation was the employment of a single test velocity. However, the addition of more test velocities would not have necessarily changed the tenor of the main findings, as revealed by a study of orthopedic patients [41]. Admittedly, the efficiency of multiple velocity testing in MS requires further exploration, although the difficulty that these patients exhibit when exercising at high angular velocities should be taken into proper account [36].
In terms of sample size, although the present study is in line with the recommendation that reliability studies should enroll at least 15–20 patients [11], the present results need to be confirmed over a larger sample.
Finally, and as a precaution, the present findings should, at this point, not be generalized to muscle groups other than the ankle dorsiflexors considering their neurophysiological and biomechanical peculiarities [34].
Practical applications
In general, the massive increase of the literature dealing with new strategies to characterize muscle strength in PwMS is a decisive proof for the growing interest in new competencies and methodologies which are derived from exercise physiology and sports sciences. This interest has recently stimulated a translational process mandating the inclusion of exercise and strength conditioning experts in the multidisciplinary clinical team of neurologists, physiatrists and physiotherapists.
From the more focused viewpoint, strength and conditioning professionals involved in testing and rehabilitation of muscle strength in PwMS should be aware of the unique importance of the concept of responsiveness when adjusting or designing an intervention program. They should also take note of the additive value of using the MW when assessing the performance of people afflicted with this disease.
Footnotes
Acknowledgments
We wish to thank Paul Gottlieb, MA (Cantab), MPhil, for editing the manuscript. This work was supported by Fondazione Italiana Sclerosi Multipla (FISM Grant 2016/R/11).
Conflict of interest
The authors declare no conflict of interest.