There is a growing interest in identifying markers of pulmonary function that are predictive of peripheral muscle dysfunction in chronic obstructive pulmonary disease (COPD); however, studies of this relationship have yielded contradictory results in the literature.
OBJECTIVES:
To evaluate the strength and endurance of the quadriceps and hamstring muscles according to gender and to evaluate the associations between lower limb muscle function and lung function, health-related quality of life (HRQoL) and 25-hydroxivitamin D3 (25(OH)D) levels in patients with COPD.
METHODS:
Forty-two patients with COPD and 42 matched healthy controls underwent knee isokinetic dynamometry at 75 and 240/s as well as isometric handgrip strength testing. All patients underwent pulmonary function tests and measurement of 25(OH)D. HRQoL was evaluated using the COPD Assessment Test (CAT), the 36-Item Short-Form Health Survey (SF-36) and the Saint George’s Respiratory Questionnaire (SGRQ).
RESULTS:
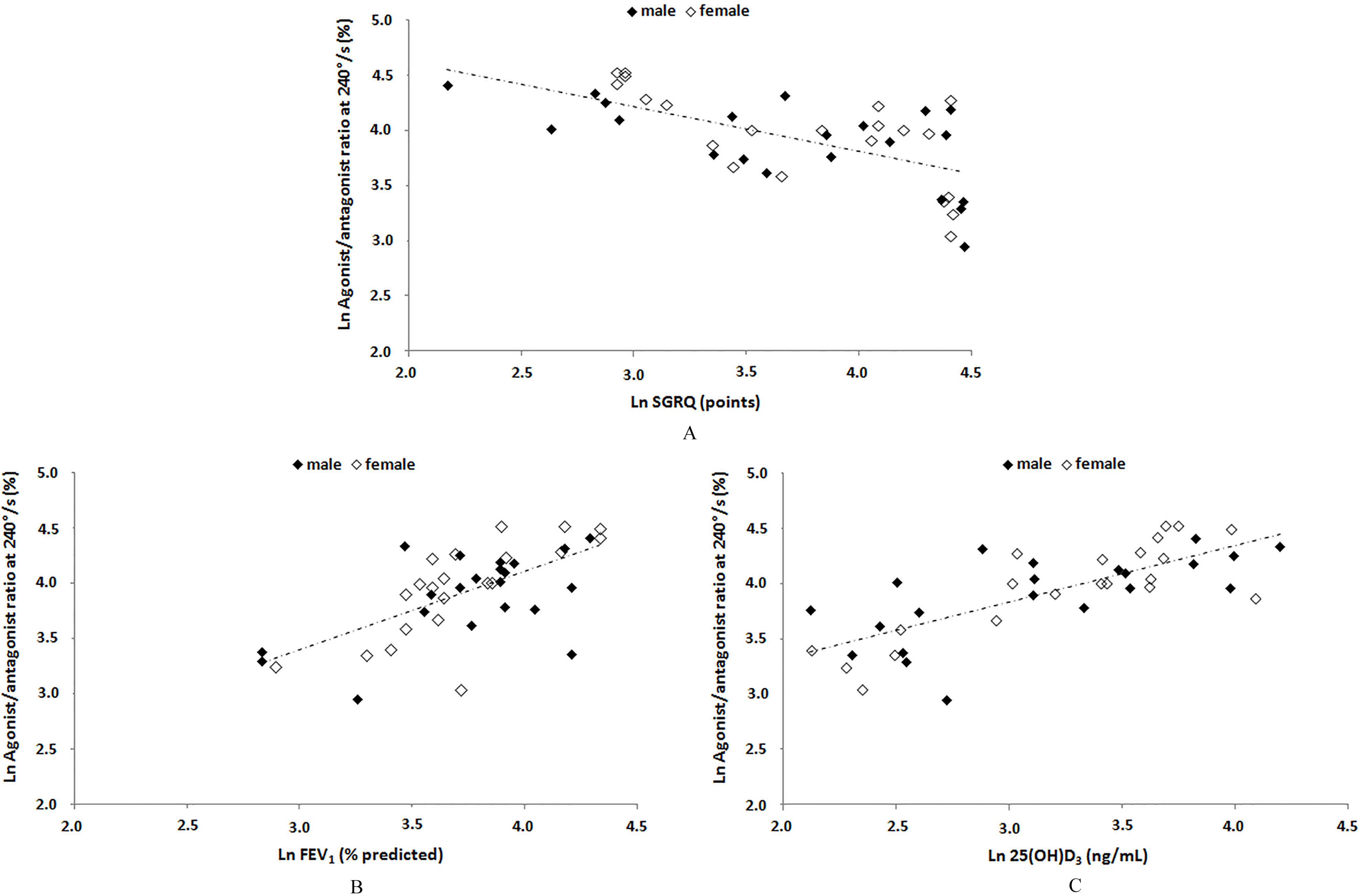
Most isokinetic parameters showed differences between males and females as well as between COPD patients and controls; the greatest differences were observed among females with COPD and their matched controls. The strongest correlations were observed between the isokinetic parameters and the SF-36 physical component summary (PCS) and SGRQ and pulmonary function variables, especially at the higher velocity. At this velocity, the agonist/antagonist ratio was positively correlated with the SF-36 PCS (r 0.65), 25(OH)D levels (r 0.76) and forced expiratory volume in one second (r 0.65) and was negatively correlated with the CAT (r 0.53) and the SGRQ (r 0.64) ( 0.001 for all correlations). The associations between the isokinetic parameters and 25(OH)D levels were stronger when endurance was tested.
CONCLUSIONS:
Patients with COPD show a reduction in both strength and endurance, especially in females. The relationships between muscle function, lung function, HRQoL and 25(OH)D levels are most striking when endurance and hamstring/quadriceps muscle balance are tested. In COPD, forced expiratory volume in one second is the strongest marker of lung function that predicts muscle dysfunction.
Muscle dysfunction is defined as the inability of a muscle to perform its task as a result of loss of strength, endurance or both [1, 2, 3, 4]. Muscle dysfunction is an important systemic effect of chronic obstructive pulmonary disease (COPD), and the mechanisms of its development are still not fully understood [1, 2, 3, 4, 5, 6, 7]. Decreased muscle strength in the lower limbs, especially the quadriceps, occurs at a rate that is two to four times faster in patients with COPD; a reduction of 20–30% in muscle strength can be seen in patients with COPD compared to healthy individuals [1, 8, 9, 10]. This muscle dysfunction has important clinical consequences for these patients because quadriceps dysfunction is associated with low exercise tolerance, an increased use of health resources and poorer survival [1, 11, 12, 13, 14, 15]. Although the isometric maximum voluntary contraction (QMVC) measure is widely used, isokinetic dynamometry has been increasingly utilized in clinical practice in recent years and is currently considered to be the gold standard for assessing muscle dysfunction in several clinical conditions [16, 17]. This isokinetic test had introduced a new dimension in the analysis of muscle function, under the principle that muscle groups can be fully exerted throughout the entire range of joint motion [17]. Despite its clinical utility, the isokinetic test has not been extensively explored in patients with COPD.
There is growing interest in identifying markers of pulmonary function that are predictive of peripheral muscle dysfunction in COPD due to the close relationship between peripheral muscle dysfunction and clinical outcomes in lung disease [18]; however, the study of this relationship has yielded contradictory results in the literature. One study showed that patients with COPD and quadriceps dysfunction had greater airflow obstruction and lung hyperinflation [19], while another study found that patients with quadriceps dysfunction had similar airway obstruction to patients without dysfunction [7]. Although the effects of 25-hydroxivitamin D (25(OH)D) on skeletal muscle are not fully understood, it has been shown that 25(OH)D helps to maintain muscle mass [20, 21]. In a recent study, Ausín et al. [5] demonstrated that 25(OH)D levels were lower in patients with COPD compared to healthy controls; furthermore, they observed that 25(OH)D levels were directly associated with muscle strength measured by handgrip and QMVC measures, but this finding was observed only in females. It remains unclear whether 25(OH)D deficiency differentially affects strength and endurance on more objective measures in patients with COPD.
Lower limb muscle dysfunction is known to be correlated with variables such as age and body mass; additionally, males typically have higher muscular strength compared to females [19]. Thus, when evaluating muscle dysfunction and effort intolerance in COPD patients, it is important to look at males and females separately [19]. Muscle dysfunction in patients with COPD can vary greatly when assessed by QMVC measures [5, 7, 19]; therefore, studies on muscle dysfunction in this patient population should utilize isokinetic dynamometry, which is considered the gold standard. In addition, functional deterioration in COPD patients does not occur homogeneously in all muscle groups, implying that health-related quality of life (HRQoL) is affected in different ways [1, 22]. We hypothesized that the impact of COPD on the strength and endurance of knee musculature is varied and that these dysfunctions are not uniform in relation to gender, lung function and quality of life. Thus, the objectives of the present study were to evaluate muscle dysfunction utilizing isokinetic dynamometry according to gender and to evaluate the associations between strength and endurance measures and HRQoL, lung function and 25(OH)D levels in patients with COPD.
Methods
Participants
Between April 2015 and March 2017, a cross-sectional, observational study was conducted in which 61 consecutive COPD patients were evaluated. The patients were recruited at Newton Bethlem Hospital in Rio de Janeiro, Brazil. The inclusion criteria were patients of both genders with age 40 years, smoking history of at least 10 pack-years and a diagnosis of COPD confirmed via spirometry, which indicated a forced expiratory volume in one second (FEV)/forced capacity vital ratio less than 70% [11]. Patients who had any of the following exclusion criteria were excluded from the study: FEV 80%; respiratory exacerbations in the last four weeks; regular participation in a physical reconditioning programme during the previous 12 months; use of oral corticosteroid or long-term supplemental oxygen therapy; impairment of normal biomechanical movement; and individuals who were considered “very active” by the International Physical Activity Questionnaire (IPAQ) [23]. We also evaluated a sex-, age-, body mass-, height- and body mass index-matched control group, utilizing the following exclusion criteria: history of smoking or previous cardiopulmonary disease, impairment of normal biomechanical movement and individuals who were considered “very active” by the IPAQ [23]. The protocol was approved by the Research Ethics Committee of the Augusto Motta University Centre under number CAAE-52711116.7.0000.5235, and all subjects were informed of the benefits and risks of the investigation prior to signing an institutionally approved informed consent document to participate in this study.
Measurements
Patients underwent clinical evaluations, which included medication use, the modified Medical Research Council (mMRC) scale and the COPD Assessment Test (CAT) questionnaire. The mMRC scale is a subjective tool that assesses limitations in activities of daily living (ADLs); this instrument uses a 5-item scale, with patients selecting which item indicates their level of limitation in ADLs due to severity of dyspnoea [11]. The CAT is a specific questionnaire used to quantify the overall impact of COPD on the patient’s health status. This one-dimensional measure contains 8 items. At the end of the test, the scores of all of the responses are summed. The total score ranges from 0 to 40, and higher scores indicate poorer health status [24].
All patients were classified into stages I-IV and A-D according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria [11]. The severity classification of airflow limitation was based on FEV values after salbutamol use as follows: GOLD I (mild, FEV 80% predicted); GOLD II (moderate, 50% FEV 80% predicted); GOLD III (severe, 30% FEV 50% predicted); and GOLD IV (very severe, FEV 30% predicted). We also used the ABCD assessment tool, which is based on the mMRC scale, CAT questionnaire and exacerbations history (0 or 1 not leading to hospital admission vs. 2 or 1 leading to hospital admission). Thus, the patients were classified as follows: A (mMRC 0–1, CAT 10 and exacerbations history 0 or 1 not leading to hospital admission); B (mMRC 2, CAT 10 and exacerbations history 0 or 1 not leading to hospital admission); C (mMRC 0–1, CAT 10 and exacerbations history 2 or 1 leading to hospital admission); and D (mMRC 2, CAT 10 and exacerbations history 2 or 1 leading to hospital admission) [11].
The HRQoL was evaluated utilizing the 36-item Short-Form Health Survey (SF-36) and the Saint George’s Respiratory Questionnaire (SGRQ); both were translated into the Portuguese language and validated for use in Brazil [25]. The SF-36 is a generic HRQoL instrument composed of 36 items that are grouped into eight dimensions and divided into two general components: the 21-item physical component summary (PCS) and the 14-item mental component summary (MCS). Scores on the SF-36 are converted to a 100-point scale; higher scores indicate better HRQoL. The SGRQ is a 76-item questionnaire that is grouped into the following three domains: symptoms, activity and psychosocial impact. The scores on each domain of the SGRQ can reach a maximum of 100 points; lower scores indicate a better HRQoL.
Plasma samples were tested for 25(OH)D using a radioimmunoassay kit (DiaSorin, Stillwater, MN, USA); 25(OH)D deficiency was defined when plasma 25(OH)D levels were 20 ng/mL [26].
All patients underwent pulmonary function tests (PFTs) (spirometry, body plethysmography and respiratory muscle strength) using the Collins Plus Pulmonary Function Testing System (Warren E. Collins, Inc., Braintree, MA, USA). All PFTs followed the guidelines defined by the American Thoracic Society [27], and reference values for the Brazilian population were considered [28].
The isometric handgrip strength (IHGS) test was measured utilizing an isometric hydraulic dynamometer (SH5001, Saehan Corporation, Korea) in the patient’s dominant hand. After proper positioning, they were instructed to perform three maximum voluntary contractions with a 60-second interval between each contraction; the highest value was used for analysis [29].
Anthropometry, clinical and pulmonary function data of the studied sample
Variable
Males with COPD
Females with COPD
Male controls
Female controls
( 21)
( 21)
( 21)
( 21)
Demographic and anthropometric data
Age (years), mean (SD)
67.9
(8.7)
66.3
(7.3)
64.7 (8.3)
63.7 (6.1)
BMI (kg/m), mean (SD)
23.6
(5.8)
23.9
(4.3)
25.4 (3.6)
25.1 (3.4)
GOLD stages, (%)
II
9
(42.9)
5
(23.8)
–
–
III–IV
12
(57.1)
16
(76.2)
–
–
A–B
7
(33.3)
7
(33.3)
–
–
C–D
14
(66.7)
14
(66.7)
–
–
Clinical data
mMRC scale, (%)
2
10
(47.6)
9
(42.9)
–
–
2
11
(52.4)
12
(57.1)
–
–
CAT score (points)
14
(7–26)
18
(8–26.5)
–
–
SF36 PCS (points), mean (SD)
48.6
(19.3)
43.2
(20.1)
–
–
SF36 MCS (points), mean (SD)
56.5
(10.3)
59.2
(9.9)
–
–
SGRQ (points), median (IQR range)
47
(23.5–79)
46
(22–76.5)
25(OH)D (ng/mL), median (IQR range)
22.2
(12.6–39.7)
26
(15.6–39)
Lung function
FVC (% predicted), mean (SD)
76.4
(15.3)
72.2
(13.8)
–
–
FEV (% predicted), mean (SD)
45.7
(15.4)
43.4
(15.5)
–
–
FEV/FVC (%), mean (SD)
46.2
(13.3)
47.6
(12.6)
–
–
TLC (% predicted), (IQR range)
112
(105–122)
115
(105–162)
–
–
RV (% predicted), (IQR range)
173
(142–226)
175
(147–329)
–
–
RV/TLC (%), mean (SD)
63.2
(10.1)
65.1
(13.3)
–
–
MIP (% predicted), mean (SD)
37.9
(10.8)
42.8
(16.4)
–
–
MEP (% predicted), mean (SD)
35.7
(12.4)
36
(15)
–
–
HGS (kgf), mean (SD)
29.3
(6.9)
22.7
(4.6)
33.7 (7.8)
26.4 (7.1)
Values are means (standard deviations [SD]), medians (IQR ranges) or (%). BMI body mass index; GOLD Global Initiative for Obstructive Lung Disease; mMRC modified medical Research Council; CAT COPD assessment test; SF36 PCS 36-Item Short Form Health Survey-physical component summary; SF36 MCS 36-Item Short Form Health Survey-mental component summary; SGRQ Saint George’s Respiratory Questionnaire; 25(OH)D 25-hydroxivitamin D; FVC forced vital capacity; FEV forced expiratory volume in one second; TLC total lung capacity; RV residual volume; MIP maximal inspiratory pressure; MEP maximal expiratory pressure; HGS hand grip strength. 0.005 between males and females with COPD.
Parameters of isokinetic dynamometry of the knee
Variable
Males with COPD
Females with COPD
Male controls
Female controls
( 21)
( 21)
( 21)
( 21)
Extension PT at 75/s (Nm), mean (SD)
110
(29.4)
65.1
(24.4)
152
(42.11)
118
(38.5)
Flexion PT at 75/s (Nm), mean (SD)
51.7
(15.4)
35.4
(19.1)
91.7
(34.7)
65.7
(24.5)
Extension MRTW at 75/s (J), mean (SD)
131
(28.4)
76.6
(26.3)
175
(43.7)
137
(46.4)
Flexion MRTW at 75/s (J), mean (SD)
62.2
(18)
42.8
(21.3)
114
(41.8)
89.8
(43.5)
Extension total work at 75/s (J), mean (SD)
610
(137)
361
(162)
816
(220)
561
(172)
Flexion total work at 75/s (J), mean (SD)
272
(86.3)
165
(77.5)
524
(203)
395
(110)
Extension work fatigue at 75/s (%), median (IQR range)
16.2
(7.9–19.6)
15.2
(12–21)
18.1
(8–35.3)
18.9
(11.3–29)
Flexion work fatigue at 75/s (%), median (IQR range)
18
(7.5–20.1)
18.5
(12.8–31)
19.4
(11.4–24)
19.6
(16–23.3)
Agonist/antagonist ratio at 75/s (%), mean (SD)
52.7
(15.7)
49.2
(12.1)
59.3
(11.9)
63.1
(7.9)
Extension PT at 240/s (Nm), mean (SD)
65.8
(12.6)
31.4
(9.5)
88.8
(23.6)
59.5
(15.1)
Flexion PT at 240/s (Nm), mean (SD)
39.1
(14)
20.6
(12.1)
65.8
(23.1)
41.4
(22.2)
Extension MRTW at 240/s (J), mean (SD)
73.4
(25.7)
41.5
(19.5)
103
(33.1)
72.3
(23.3)
Flexion MRTW at 240/s (J), median (IQR range)
38.2
(18–46.7)
20.4
(11–28.2)
70
(44.1–102)
47.4
(33.8–64)
Extension total work at 240/s (J), mean (SD)
817
(291)
387
(208)
1244
(357)
890
(286)
Flexion total work at 240/s (J), median (IQR range)
403
(183–529)
231
(114–347)
759
(520–1207)
674
(391–899)
Extension work fatigue at 240/s (%), mean (SD)
30.5
(12.3)
31.3
(14)
39.9
(12.8)
35.6
(14.8)
Flexion work fatigue at 240/s (%), mean (SD)
43.1
(18.9)
29
(10.1)
50.2
(16.8)
39.1
(18.4)
Agonist/antagonist ratio at 240/s (%), mean (SD)
46.8
(12)
42.3
(11.6)
70.9
(19.4)
73.6
(16.5)
Values are means (SD) or medians (IQR ranges). PT peak torque; MRTW maximum repetition of the total work. 0.01 between males and females with COPD and between males with COPD and controls. 0.001 between females with COPD and controls. 0.001 between males and females with COPD and between males with COPD and controls. 0.005 between males and females with COPD. 0.01 between males with COPD and controls. 0.001 between males and females with COPD. 0.05 between males with COPD and controls. 0.005 between females with COPD and controls.
Pearson’s correlation coefficients between the isokinetic dynamometry of the knee, quality of life and vitamin D levels of patients with COPD
Variable
CAT score
SF36 PCS
SF36 MCS
SGRQ
25(OH)D
Extension PT at 75/s (Nm)
0.19
0.37
0.09
0.23
0.27
Flexion PT at 75/s (Nm)
0.27
0.49
0.04
0.38
0.43
Extension MRTW at 75/s (J)
0.16
0.32
0.15
0.20
0.28
Flexion MRTW at 75/s (J)
0.28
0.49
0.11
0.42
0.45
Extension total work at 75/s (J)
0.16
0.33
0.14
0.21
0.28
Flexion total work at 75/s (J)
0.28
0.50
0.10
0.40
0.50
Extension work fatigue at 75/s (%)
0.07
0.20
0.26
0.14
0.35
Flexion work fatigue at 75/s (%)
0.04
0.05
0.21
0.05
0.09
Agonist/antagonist ratio at 75/s (%)
0.43
0.63
0.06
0.63
0.59
Extension PT at 240/s (Nm)
0.26
0.40
0.13
0.32
0.36
Flexion PT at 240/s (Nm)
0.41
0.58
0.04
0.56
0.58
Extension MRTW at 240/s (J)
0.28
0.45
0.20
0.37
0.44
Flexion MRTW at 240/s (J)
0.42
0.62
0.06
0.59
0.65
Extension total work at 240/s (J)
0.24
0.40
0.17
0.29
0.42
Flexion total work at 240/s (J)
0.40
0.60
0.10
0.58
0.69
Extension work fatigue at 240/s (%)
0.35
0.53
0.06
0.55
0.51
Flexion work fatigue at 240/s (%)
0.34
0.18
0.07
0.24
0.02
Agonist/antagonist ratio at 240/s (%)
0.53
0.65
0.01
0.64
0.76
PT peak torque; MRTW maximum repetition of the total work; CAT COPD assessment test; SF36 PCS 36-Item Short Form Health Survey-physical component summary; SF36 MCS 36-Item Short Form Health Survey-mental component summary; SGRQ Saint George’s Respiratory Questionnaire; 25(OH)D 25-hydroxivitamin D. The values in bold refer to significant differences. 0.05. 0.01. 0.005. 0.001.
Pearson’s correlation coefficients between the isokinetic dynamometry of the knee, lung function and handgrip strength of patients with COPD
Variable
FEV
TLC
RV
MIP
MEP
HGS
Extension PT at 75/s (Nm)
0.49
0.26
0.39
0.08
0.09
0.33
Flexion PT at 75/s (Nm)
0.57
0.34
0.47
0.06
0.13
0.15
Extension MRTW at 75/s (J)
0.38
0.27
0.37
0.08
0.07
0.10
Flexion MRTW at 75/s (J)
0.49
0.29
0.42
0.12
0.10
0.11
Extension total work at 75/s (J)
0.37
0.25
0.35
0.09
0.07
0.14
Flexion total work at 75/s (J)
0.47
0.33
0.46
0.16
0.15
0.10
Extension work fatigue at 75/s (%)
0.31
0.05
0.14
0.31
0.07
0.02
Flexion work fatigue at 75/s (%)
0.19
0.02
0.03
0.04
0.06
0.13
Agonist/antagonist ratio at 75/s (%)
0.50
0.30
0.42
0.32
0.20
0.13
Extension PT at 240/s (Nm)
0.59
0.31
0.45
0.04
0.20
0.18
Flexion PT at 240/s (Nm)
0.69
0.34
0.52
0.17
0.23
0.31
Extension MRTW at 240/s (J)
0.58
0.31
0.45
0.04
0.26
0.17
Flexion MRTW at 240/s (J)
0.67
0.27
0.46
0.27
0.25
0.32
Extension total work at 240/s (J)
0.57
0.28
0.44
0.02
0.22
0.15
Flexion total work at 240/s (J)
0.57
0.22
0.39
0.30
0.24
0.23
Extension work fatigue at 240/s (%)
0.48
0.19
0.32
0.04
0.17
0.03
Flexion work fatigue at 240/s (%)
0.32
0.31
0.33
0.25
0.30
0.05
Agonist/antagonist ratio at 240/s (%)
0.65
0.31
0.46
0.43
0.40
0.33
PT peak torque; MRTW maximum repetition of the total work; FEV forced expiratory volume in one second; TLC total lung capacity; RV residual volume; MIP maximal inspiratory pressure; MEP maximal expiratory pressure; HGS hand grip strength. The values in bold refer to significant differences. 0.05. 0.01. 0.005. 0.001.
The muscles of the knee joint were evaluated utilizing an isokinetic dynamometer of the knee (Biodex System 4 PRO, Biodex Medical Systems, Inc., Shirley, NY, USA) from the Admiral Adalberto Nunes Physical Education Centre (Brazilian Navy), Rio de Janeiro, Brazil. Before each test, the patient underwent a familiarization exercise that included three submaximal repetitions using only the dominant lower limb [30]. After familiarization, the strength and endurance analyses were performed utilizing angular velocities of 75 and 240/s, respectively; two sets of 15 repetitions were conducted during each analysis [31]. Between each test, a two-minute rest period was granted. The concentric-concentric mode was selected for each evaluation. The following variables were analysed: peak torque (PT, the maximum force at any given point of during the entire range of motion), maximum repetition of the total work (MRTW, the total muscle strength in the repetition that had the highest production of muscle work), total work (the ability to generate muscle force throughout the entire range of motion), work fatigue (the relationship between the first third and last third of the muscle work performed) and agonist/antagonist ratio (PT of the hamstring muscles divided by PT of the quadriceps during a given velocity of contraction) [32, 33]. The highest differential value each of the variables was analysed.
Data analysis
The data were analysed using the SAS 6.11 software suite (SAS Institute, Inc., Cary, NC, USA). A previous analysis was performed to verify the normality of the variables utilizing the Shapiro-Wilk test and a graphical analysis of the histograms. Because some variables showed non-Gaussian distribution, a natural logarithmic transformation was applied to allow parametric tests to be used. The described analysis was expressed with the appropriate measures of central tendency and dispersion. The comparisons of the anthropometric variables, clinical data, lung function and dynamometry among the four groups were made utilizing one-way analysis of variance (ANOVA) statistics and Tukey’s multiple comparisons tests. The comparison between the two patient groups was made utilizing Student’s t-test for independent samples. The categorical data were compared utilizing the chi-squared test. The associations between the isokinetic dynamometry and numerical variables were analysed utilizing the Pearson correlation coefficient; furthermore, the dichotomous categorical variables were analysed utilizing Student’s t-test for independent samples. Forward stepwise regression analysis was used to identify the pulmonary function variables that were independently related to the parameters of isokinetic dynamometry of the knee. Statistical significance was set at 0.05.
Relationship of the natural logarithm (Ln) of agonist/antagonist ratio at 75/s with the natural logarithm (Ln) of Saint George’s Respiratory Questionnaire (SGRQ) (0.64, 0.0001) (A), the natural logarithm (Ln) of forced expiratory volume in one second (FEV) ( 0.65, 0.0001) (B) and the natural logarithm (Ln) of 25-hydroxivitamin D (25(OH)D) ( 0.76, 0.0001) (C).
Forward stepwise regression models for parameters of isokinetic dynamometry of the knee using pulmonary function variables
Outcome variable
Independent variables
B
SE
value
Cumulative R
Extension PT at 75/s (Nm)
FEV
0.598
0.170
0.001
0.24
Flexion PT at 75/s (Nm)
FEV
0.773
0.177
0.001
0.32
Extension MRTW at 75/s (J)
FEV
0.468
0.180
0.013
0.14
Flexion MRTW at 75/s (J)
FEV
0.703
0.199
0.001
0.24
Extension total work at 75/s (J)
FEV
0.467
0.185
0.016
0.14
Flexion total work at 75/s (J)
FEV
0.682
0.200
0.002
0.22
Extension work fatigue at 75/s (%)
FEV
0.530
0.260
0.048
0.10
Flexion work fatigue at 75/s (%)
Agonist/antagonist ratio at 75/s (%)
FEV
0.377
0.103
0.001
0.25
Extension PT at 240/s (Nm)
FEV
0.759
0.166
0.001
0.34
Flexion PT at 240/s (Nm)
FEV
1.029
0.173
0.001
0.47
Extension MRTW at 240/s (J)
FEV
0.857
0.191
0.001
0.33
Flexion MRTW at 240/s (J)
FEV
1.423
0.251
0.001
0.45
Extension total work at 240/s (J)
FEV
0.812
0.187
0.001
0.32
Flexion total work at 240/s (J)
FEV
1.252
0.286
0.001
0.32
Extension work fatigue at 240/s (%)
FEV
0.640
0.186
0.001
0.23
Flexion work fatigue at 240/s (%)
RV
0.434
0.195
0.032
0.11
Agonist/antagonist ratio at 240/s (%)
FEV
0.641
0.126
0.001
0.51
MIP
0.332
0.125
0.011
B regression coefficient; SE standard error; PT peak torque; MRTW maximum repetition of the total work; FEV forced expiratory volume in one second; RV residual volume; MIP maximal inspiratory pressure. No variables were retained for the regression model.
Results
Among the 61 patients who were evaluated, 19 were excluded for the following reasons: refusal to participate in the study ( 10), respiratory infection in the month prior to recruitment ( 4), home oxygen therapy ( 3) and lower limb deformity ( 2). Thus, the study sample consisted of 21 males and 21 females. The mean smoking load was 58.2 (standard deviation (SD) 24.9) and 40 (SD 21.4) pack-years for males and females, respectively ( 0.09). The times from initial diagnosis of the disease were 7.83 (SD 4.24) and 6.50 (SD 3.75) years for males and females, respectively ( 0.26). All but three patients were treated with bronchodilators and/or inhaled corticosteroids. 25(OH)D deficiency was noted in 35.7% of the patients. The anthropometric variables, clinical data, lung function and handgrip strength of males and females with COPD and their respective controls, as well as the comparisons between these subjects, are summarized in Table 1.
Comparisons between the males and females with COPD according to the variables provided by isokinetic dynamometry of the knee are shown in Table 2. Most of the isokinetic parameters showed differences between COPD patients and their respective controls, as well as between males and females with COPD; however, the greatest differences were seen between females with COPD and their respective controls.
We evaluated the correlations between isokinetic dynamometry variables of the knee with HRQoL, 25(OH)D levels, lung function and handgrip strength in patients with COPD (Tables 3 and 4, Fig. 1). The strongest correlations were observed between the isokinetic parameters and the SF-36 PCS, the SGRQ, 25(OH)D levels, FEV and residual volume (RV), especially at an angular velocity of 240/s.
We further investigated whether the pulmonary function variables would demonstrate an independent role in predicting of the strength or endurance in these patients. The results of forward stepwise regression analysis for prediction of the variables of isokinetic dynamometry of the knee are shown in Table 5. We found that FEV was the only independent predictor of the variables of isokinetic dynamometry of the knee at an angular velocity of 75/s (except for flexion work fatigue); the explanatory capacity between the models showed a maximum cumulative R of 0.32. Similarly, FEV was the only independent predictor of knee isokinetic dynamometry variables at an angular velocity of 240/s (except for flexion work fatigue and agonist/antagonist ratio); the explanatory capacity between the models showed a maximum cumulative R of 0.51.
Discussion
The main finding of the present study is that a reduction of knee muscle strength and endurance is present in males and females with COPD compared to their respective controls; furthermore, this reduction is more pronounced in females. In these patients, knee muscle dysfunction is associated with a poorer pulmonary function, lower HRQoL and 25(OH)D deficiency; moreover, these associations are more striking in patients with greater abnormalities in their hamstring/quadriceps ratio. In COPD, FEV is the major marker of pulmonary function that predicts loss of strength and/or endurance. In addition, endurance, compared to muscle strength, showed stronger associations with HRQoL, lung function and 25(OH)D levels.
Our study objectively showed the importance of knee muscle dysfunction in patients with COPD in comparison to healthy controls. Pleguezuelos et al. [22] observed a similar reduction in the strength of knee extensors and flexors in males with COPD, although they did not evaluate female patients. In contrast, Menon et al. [34] did not observe significant differences in the PT and total work in extension of patients with COPD compared to controls; however, these authors evaluated only 12 COPD patients and did not separate their cohort by gender. In COPD, skeletal muscle dysfunction is the result of several factors, including deconditioning, local inflammation and the use of oral steroids, which promotes structural and functional changes in contractile tissue [1, 2, 3, 4, 5, 6, 22, 35, 36, 37]. Like our findings, other studies [5, 22] have not observed a significant reduction in handgrip strength in COPD patients, indicating that muscles are more preserved in the upper limbs. This result is likely due to greater preservation of muscle conditioning and the fact that the muscle function of the upper limbs is more related to activities of daily living than the pathogenesis of COPD. Thus, a downward disease spiral theory has been hypothesized in which worsening dyspnoea leads to a sedentary lifestyle and deconditioning of the locomotor muscles; consequently, greater inactivity and damage to the musculature of the lower limbs results [19]. Moreover, the differences between the upper and lower limbs of COPD patients show that muscle dysfunction differs between muscle compartments; this finding is of paramount importance in the design of physical reconditioning programmes for these patients. Interestingly, we observed a greater knee muscle dysfunction in females compared to males. Previous studies have investigated the influence of gender on muscle function in COPD [6, 37]. The factors that are responsible for the greater susceptibility of females to lower limb musculature changes have been debated [6, 37]; however, the greater functional damage seen in females can be at least partially explained by decreased physical activity and a lower percentage of type II fibres.
Most studies on peripheral muscle function in COPD have focused on strength rather than endurance; however, endurance assessments may be more sensitive and valuable for the study of interventions that specifically target lower limb muscles [1]. In the present study, we utilized both low (75/s) and high (240/s) angular velocity. With lower generated torque and more repetitions, the higher angular velocity is often used to reflect muscle endurance, which is a characteristic attributed to type II fibres [34]. Interestingly, we found more robust associations between isokinetic measures of endurance and clinical variables as well as between endurance and markers of airflow obstruction. In COPD, there is a progressive transformation of the type of muscle fibres from type I to II [1, 34]; the latter are more easily fatigued; therefore, we believe that this transformation makes the muscle more vulnerable to stress at high angular velocities, resulting in a greater exposure to muscular dysfunction when endurance is tested. Interestingly, functional capacity (assessed utilizing the 6-minute walk test) appears to be more related to endurance than knee muscle strength testing in subjects with COPD [38]. Thus, our findings show the importance of evaluating the endurance of knee musculature in addition to endurance training programmes to improve the functional capacity of subjects with COPD. A more objective assessment of endurance may identify patients who are at increased risk for exercise intolerance and premature death [1].
In the present study, the strongest correlations between isokinetic parameters and lung function indices were noted in two important markers of bronchial obstruction (FEV and RV), especially when endurance was tested. Similar to our findings, a recent study in males with COPD demonstrated an association between lung function and both muscle mass (assessed by magnetic resonance imaging) and lower limb strength (assessed by leg press exercise); furthermore, this study showed a reduced inspiratory capacity to total lung capacity ratio that was associated with inflammatory markers and the overall level of physical activity [39].
In our study, we also sought a marker of pulmonary function that could predict muscle dysfunction using forward stepwise regression analysis. Thus, we found that FEV was the major marker of lung function to predict loss of strength and/or endurance. In COPD, the level of FEV is used to grade the severity of obstruction, and FEV is linked better to prognosis than any other single test of pulmonary function; moreover, patients with markedly reduced FEV values are much more likely to die from COPD [10, 11, 40]. In our study, it is worth noting that the explanatory capacity of FEV was much higher to predict a reduction in endurance than loss of strength (51% vs. 32%). Interestingly, Menon et al. [34] evaluated quadriceps biopsies of patients with COPD and found a positive correlation between the proportion of type I fibres and FEV; furthermore, the same study noted that neutrophils are more prevalent in the quadriceps of COPD patients when compared to controls. Thus, neutrophilic inflammation may indicate a link between pulmonary and systemic abnormalities, including changes in skeletal muscle. Neutrophils enact muscle damage via the release of proteolytic enzymes and free radicals; their presence in COPD may contribute to muscle dysfunction [34, 41].
In the present study, we observed strong correlations between knee isokinetic parameters and HRQoL [1]. Similar to our findings, Seymour et al. [19] observed a deterioration in HRQoL measured using the SGRQ in patients with COPD and dysfunction of knee musculature assessed using the QMVC measure. In COPD, the impairment of myogenesis has been suggested as a potential mechanism for cachexia, which in turn may be associated with a progressive deterioration in HRQoL [42]. Interestingly, we observed that the agonist/antagonist ratio was the isokinetic parameter that was most strongly associated with HRQoL. The more severe impairment of the hamstrings may be explained, at least in part, by the greater amount of time that these patients spend seated compared to healthy individuals. While a patient is seated, the hamstrings are in a shortened position because the knee is flexed at 90, thus reducing the number of sarcomeres in series; therefore, the muscle area adapts to this new length [22]. With this in mind, exercises that strengthen flexor muscles may be a salient strategy for rehabilitation programmes in patients with COPD.
Vitamin D deficiency is a problem that affects a substantial proportion of the general population, with a prevalence that is estimated at more than 1 billion people worldwide [43]. There is a positive association between vitamin D and peripheral muscle function, and several studies have shown that age-related loss of muscle mass and strength is more prevalent in older adults with lower levels of 25(OH)D [44, 45]. In fact, the 25(OH)D receptor is abundantly expressed within the lower limb muscles, where it mediates various gene promoters; therefore, the 25(OH)D pathway may play an important role in maintaining the health of this muscle group [1, 46]. In patients with COPD, the association that we observed in our study between 25(OH)D levels and muscle function is not surprising [21, 47]; however, the correlations were stronger between 25(OH)D levels and the endurance parameters compared to the strength parameters. One possible explanation for this finding is the progressive change in the type of fibres observed in COPD because type II fibres are more abundant in COPD patients and are more prone to fatigue. Thus, 25(OH)D supplementation in these patients may be an interesting approach to increase the performance of lower limb muscles and, consequently, fatigue tolerance [21].
One strength of the present study is that we evaluated several parameters provided by isokinetic testing (i.e., those related to both strength and endurance); accordingly, these parameters may be vital to the physical reconditioning of patients with COPD, especially the agonist/antagonist ratio. However, our study also has limitations. First, the cross-sectional design and relatively small sample make it difficult to generalize our findings. Second, the 25(OH)D status in the control group was not measured; this information would be useful for a better understanding of the relationship between 25(OH)D levels and peripheral muscle function. Further research is still needed to determine the relevance of isokinetic measures for functional performance and to develop adequate load protocols for endurance training programmes for patients with COPD.
In conclusion, the present study shows that patients with COPD have reductions in both strength and endurance; furthermore, these reductions are more marked in females. Muscle dysfunction, especially an imbalance between the quadriceps and hamstring muscles, is strongly related to worsening HRQoL and 25(OH)D deficiency. The associations between muscle function, lung function, HRQoL and 25(OH)D levels are stronger when endurance is tested. In these patients, FEV is the strongest marker of lung function to predict loss of strength, endurance or both. Our results may have implications for the understanding of the pathogenesis of skeletal muscle dysfunction in COPD and the development of physical reconditioning programmes for these patients.
Footnotes
Acknowledgments
We are grateful to CNPq (#304625/2016-7) and FAPERJ (#E-26/010.001564/2016) for their financial support.
Conflict of interest
None.
References
1.
MaltaisFDecramerMCasaburiRBarreiroEBurelleYDebigaréR, et al. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014; 189(9): e15-62.
2.
BarreiroEBustamanteVCejudoPGáldizJBGeaJde LucasPMartínez-LlorensJ, et al. Guidelines for the evaluation and treatment of muscle dysfunction in patients with chronic obstructive pulmonary disease. Arch Bronconeumol. 2015; 51(8): 384-95.
3.
KimHCMofarrahiMHussainSN. Skeletal muscle dysfunction in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2008; 3(4): 637-58.
4.
GeaJPascualSCasadevallCOrozco-LeviMBarreiroE. Muscle dysfunction in chronic obstructive pulmonary disease: update on causes and biological findings. J Thorac Dis. 2015; 7(10): E418-38.
5.
AusínPMartínez-LlorensJSabaté-BrescoMCasadevallCBarreiroEGeaJ. Sex differences in function and structure of the quadriceps muscle in chronic obstructive pulmonary disease patients. Chron Respir Dis. 2016; 14(2): 127-39.
6.
EvansRAKaplovitchEBeauchampMKDolmageTEGoldsteinRSGilliesCL, et al. Is quadriceps endurance reduced in COPD? a systematic review. Chest. 2015; 147(3): 673-84.
7.
NellessenAGDonáriaLHernandesNAPittaF. Analysis of three different equations for predicting quadriceps femoris muscle strength in patients with COPD. J Bras Pneumol. 2015; 41(4): 305-12.
8.
SpruitMAPittaFGarveyCZuWallackRLRobertsCMCollinsEG, et al. Differences in content and organisational aspects of pulmonary rehabilitation programmes. Eur Respir J. 2014; 43(5): 1326-37.
9.
KharbandaSRamakrishnaAKrishnanS. Prevalence of quadriceps muscle weakness in patients with COPD and its association with disease severity. Int J Chron Obstruct Pulmon Dis. 2015; 10: 1727-35.
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease [homepage on the Internet]. 2017 [updated 2017 May 16; cited 2017 Jul 25]. Available from: http://www.goldcopd.org/.
12.
NybergASaeyDMaltaisF. Why and how limb muscle mass and function should be measured in patients with COPD. Ann Am Thorac Soc. 2015; 12(9): 1269-77.
13.
RibeiroFLépinePAGarceau-BolducCCoatsVAllardEMaltaisFSaeyD. Test-retest reliability of lower limb isokinetic endurance in COPD: a comparison of angular velocities. Int J Chron Obstruct Pulmon Dis. 2015; 10: 1163-72.
14.
BarreiroEGeaJ. Respiratory and limb muscle dysfunction in COPD. COPD. 2014; 12(4): 1-14.
15.
GeaJAgustíARocaJ. Pathophysiology of muscle dysfunction in COPD. J Appl Physiol. 2013; 114(9): 1222-34.
16.
HomemTGuimarãesFSSantosMSKasukiLGadelhaMRLopesAJ. Balance control and peripheral muscle function in aging: a comparison between individuals with acromegaly and healthy subjects. J Aging Phys Act. 2017; 25(2): 218-27.
17.
RodriguesFMDemeyerHHornikxMCamilloCACalik-KutukcuEBurtinC, et al. Validity and reliability of strain gauge measurement of volitional quadriceps force in patients with COPD. Chron Respir Dis. 2017; 14(3): 289-97.
18.
MartinezLPittaF. A pulmonary index able to predict peripheral muscle function in COPD. Rev Port Pneumol. 2017; 23(1): 1-2.
19.
SeymourJMSpruitMAHopkinsonNSNatanekSAManWDJacksonA, et al. The prevalence of quadriceps weakness in COPD and the relationship with disease severity. Eur Respir J. 2010; 36(1): 81-8.
20.
ZhangLYuanQY. Vitamin D should be supplemented more actively in elderly patients with coronary heart disease combined with COPD. Int J Chron Obstruct Pulmon Dis. 2016; 11: 1359-65.
21.
YumrutepeTAytemurZABaysalOTaskapanHTaskapanCMHacievliyagilSS. Relationship between vitamin D and lung function, physical performance and balance on patients with stage I-III chronic obstructive pulmonary disease. Rev Assoc Med Bras. 2015; 61(2): 132-8.
22.
PleguezuelosEEsquinasCMorenoEGuiraoLOrtizJGarcia-AlsinaJ, et al. Muscular dysfunction in COPD: systemic effect or deconditioning? Lung. 2016; 194(2): 249-57.
23.
BarbozaMLBarbosaACSpinaGDSperandioEFArantesRLGagliardiAR, et al. Association between physical activity in daily life and pulmonary function in adult smokers. J Bras Pneumol. 2016; 42(2): 130-5.
24.
SilvaGPMoranoMTVianaCMMagalhãesCBPereiraED. Portuguese-language version of the COPD Assessment Test: validation for use in Brazil. J Bras Pneumol. 2013; 39(4): 402-8.
25.
WehrmeisterFCKnorstMJardimJRMacedoECNoalRBMartínez-MesaJ, et al. Pulmonary rehabilitation programs for patients with COPD. J Bras Pneumol. 2011; 37(4): 544-55.
26.
ParkYKimYSKangYAShinJHOhYMSeoJB, et al. Relationship between vitamin D-binding protein polymorphisms and blood vitamin D level in Korean patients with COPD. Int J Chron Obstruct Pulmon Dis. 2016; 11: 731-8.
27.
RedlichCATarloSMHankinsonJLTownsendMCEschenbacherWLVon EssenSG, et al. Official American Thoracic Society technical standards: spirometry in the occupational setting. Am J Respir Crit Care Med. 2014; 189(8): 983-93.
28.
Sociedade Brasileira de Pneumologia. Diretrizes para Testes de Função Pulmonar. J Pneumol. 2002; 28(suppl 3): 1-82.
29.
CrosbyCAWehbeMAMawrB. Hand strength: normative values. J Hand Surg Am. 1994; 19(4): 665-70.
30.
FelicioDCPereiraDSQueirozBZAssumpçãoAMDiasJMDPereiraLSM. Isokinetic performance of knee flexor and extensor muscles in community-dwelling elderly women. Fisioter Mov. 2015; 28(3): 555-62.
31.
LopesAJFerreiraASWalchanEMSoaresMSBunnPSGuimarãesFS. Explanatory models of muscle performance in acromegaly patients evaluated by knee isokinetic dynamometry: implications for rehabilitation. Hum Mov Sci. 2016; 49: 160-9.
32.
WalchanEMGuimarãesFSSoaresMSPinhoLKJGadelhaMRLopesAJ. Parameters of knee isokinetic dynamometry in individuals with acromegaly: association with growth hormone levels and general fatigue. Isokinet Exerc Sci. 2016; 24(4): 331-40.
33.
DvirZ. Isokinetics: Muscle Testing, Interpretation and Clinical Applications. 2nd ed. New York: Churchill Livingstone; 2004.
34.
MenonMKHouchenLSinghSJMorganMDBraddingPSteinerMC. Inflammatory and satellite cells in the quadriceps of patients with COPD and response to resistance training. Chest. 2012; 142(5): 1134-42.
35.
WaschkiBKirstenAMHolzOMuellerKCSchaperMSackAL, et al. Disease progression and changes in physical activity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015; 192(3): 295-306.
36.
RoblesPGMathurSJanaudis-FereiraTDolmageTEGoldsteinRSBrooksD. Measurement of peripheral muscle strength in individuals with chronic obstructive pulmonary disease: a systematic review. J Cardiopulm Rehabil Prev. 2011; 31(1): 11-24.
37.
Janaudis-FerreiraTWadellKSundelinGLindströmB. Thigh muscle strength and endurance in patients with COPD compared with healthy controls. Respir Med. 2006; 100(8): 1451-7.
38.
NybergATörnbergAWadellK. Correlation between limb muscle endurance, strength, and functional capacity in people with chronic obstructive pulmonary disease. Physiother Can. 2016; 68(1): 46-53.
39.
CebolleroPZambom-FerraresiFHernándezMHuetoJCascanteJAntonMM. Inspiratory fraction as a marker of skeletal muscle dysfunction in patients with COPD. Rev Port Pneumol. 2017; 23(1): 3-9.
40.
KohansalRMartinez-CamblorPAgustíABuistASManninoDMSorianoJB. The natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohort. Am J Respir Crit Care Med. 2009; 180(1): 3-10.
41.
ChoudhuryGRabinovichRMacNeeW. Comorbidities and systemic effects of chronic obstructive pulmonary disease. Clin Chest Med. 2014; 35(10): 101-30.
42.
HansenMJGualanoRCBozinovskiSVlahosRAndersonGP. Therapeutic prospects to treat skeletal muscle wasting in COPD (chronic obstructive lung disease). Pharmacol Ther. 2006; 109(1-2): 162-72.
43.
HolickMFChenTC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008; 87(4): 1080S-6S.
44.
BalogunSAitkenDWinzenbergTWillsKScottDCallisayaM, et al. Longitudinal associations of serum 25-hydroxyvitamin-D, physical activity, and knee pain and dysfunction with muscle loss in community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2017 [Epub ahead of print].
45.
LiuGLuLSunQYeXSunLLiuX, et al. Poor vitamin D status is prospectively associated with greater muscle mass loss in middle-aged and elderly Chinese individuals. J Acad Nutr Diet. 2014; 114(10): 1544-51.
46.
ZhuBZhuBXiaoCZhengZ. Vitamin D deficiency is associated with the severity of COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015; 10: 1907-16.
47.
JacksonASShrikrishnaDKellyJLHartNMoxhamJPolkeyMI, et al. Vitamin D and skeletal muscle strength and endurance in COPD. Eur Respir J. 2013; 41(2): 309-16.