
Abstract
BACKGROUND:
Assessing players’ leg strength ratios prior to season is important in order to measure performance and identify weaknesses. Leg ratios are calculated by dividing the moment of hamstring by quadriceps. The simple (concentric only) HQ ratio and the dynamic control ratio (DCR) (Hamstring eccentric/Quadriceps concentric) are used to detect asymmetry, knee strength, and bilateral deficit (BD). However, open (OKC) and closed kinetic chain (CKC) tests potentially provide different information regarding muscle strength and balance.
OBJECTIVE:
The purpose of this study was to measure the abovementioned ratios in male and female amateur rugby union players and to assess difference between OKC and CKC tests.
METHODS:
Six males (age
RESULTS:
The non-dominant leg simple ratio (0.81
CONCLUSION:
The DCR may be more sport specific when measuring knee strength, while an OKC test is more likely to detect BD due to muscle isolation.
Introduction
The demands of rugby union include periods where players must display maximal effort strength and power along with periods of high-intensity sprinting and low-intensity running [1]. Cunniffe et al. used a global positioning system to determine the physiological demands of rugby union players and reported 27% of the game was spent jogging (6–12 km/h), 24% moderate-intensity running (12–18 km/h), and 6% high-intensity running (
Injuries to the muscles, ligaments, and tendons of the lower limbs are the most common sites in rugby union players [3]. Brooks et al. reported that hamstring injuries are the second most common injury during a game and that anterior cruciate ligament tears result in the most missed time in rugby union players [4]. These injuries have been associated with large differences in strength between the quadriceps and hamstrings muscle groups [5, 6, 7]. A common method of assessment is through isokinetic dynamometry which measures concentric hamstring strength to quadriceps strength ratios (HQR). Croisier et al. reported that athletes with a HQR greater than 16.5% have a higher hamstring injury frequency [5, 6]. Another issue is eccentric hamstring strength. The literature suggests that weaker eccentric knee flexor strength is an indicator for hamstring injury reoccurrence [8, 9]. Therefore, along with screening HQR imbalances, hamstring eccentric strength measurement is also important.
The simple ratio and the DCR are common measurements for leg strength evaluation. The former measures maximal concentric peak moment of the hamstrings divided by the concentric peak moment of the quadriceps, while the latter is defined as the eccentric peak moment of the hamstrings divided by the concentric peak moment of the quadriceps. In a study with elite rugby union players, Brown et al. reported players had 0.64–0.68 simple ratios [10, 11]. More recently, Ruas et al. reported DCR values of 0.78–0.82 for dominant leg and 0.72–0.78 for non-dominant leg in elite soccer players [12]. DCR may be a more valid measurement due to the decelerative function of the hamstrings and their ability to stabilize the knee during sporting movements [13].
Rugby union is a closed kinetic chain (CKC) field sport with maximum bouts of speed, power, strength, and physicality. CKC exercises constitute body segments affixed to the ground, requiring intermuscular coordination across multiple joints compared to open kinetic chain (OKC) exercises where limb segments are free to move. OKC tests have historically been used predominately in rehabilitation programs, while strength testing generally consists of CKC exercises, (i.e. back squats, leg press, etc.). Some disagreement exists regarding whether OKC or CKC tests are more valid for assessment and rehabilitation purposes with much of the research focused on the latter. Escamilla et al. [14] examined kinetic and kinematic differences between back squat and leg extension during a three repetition maximum (RM) finding
Assessing a player’s strength capacity is important for determining position, eligibility, and return to play after injury. A bilateral strength deficit (BD) (difference between bilateral strength and the sum of both unilateral measures) greater than 10% could potentially put an athlete at greater risk for injury [17, 18]. The BD has been found in both upper and lower extremities, with larger differences in the lower limbs possibly due to postural stability requirements [19, 20]. Research has demonstrated that the BD increased with velocity, with no differences between contraction types [21]. Fast lower body muscle actions are used in most sporting events and are a primary mechanism in lower body injury, thus reducing BD may aid in both athletic performance and injury prevention. Researchers have investigated BD during a countermovement jump and sprint performance in elite sprinters and found that higher deficits were associated with less peak force in the rear leg, and less total impulse during the sprint start, resulting in lower overall performance in both the 60- and 100-meter runs [22]. A multitude of tests have been used to assess BD, with no research considering their effectiveness. The isometric mid-thigh pull (IMTP) is a CKC test examining multiple muscle groups force output involving the whole body, similar to rugby union, whereas isometric knee extension is an OKC test isolating the moment output of the quadriceps and hamstrings muscle groups only.
Due to the many requirements of the lower limbs associated with performance, multiple tests to measure the strength and power characteristics within and between legs are necessary. Favoring movements on the dominant vs. non-dominant leg may lead to imbalances that could result in injury. BD testing may identify imbalance between limbs and provide valuable information to coaches. Also, screening players for DCR by measuring isometric, eccentric and dynamic strength prior to the season may expose mode specific imbalances. Yeung et al. reported that preseason muscle imbalances may be a risk-factor for hamstring injury [23]. To the best of our knowledge, there is no research examining the values of HQ ratios in amateur rugby union players of both sexes. Measuring H/Q imbalances bilaterally and unilaterally in players during preseason can provide information regarding performance and injury risk. Therefore, the purpose of this study was two-fold: To measure HQ ratios in the dominant and non-dominant legs of male and female amateur rugby union players prior to the competitive season, and to determine differences between OKC and CKC tests in the BD.
Methods
Subjects
All participants read and signed an informed consent document that was approved by the University Institutional Review Board, in compliance with The Code of Ethics of the World Medical Association from the British Medical Journal (18 July 1964). Seventeen healthy amateur rugby union players (females,
Isometric mid-thigh pull/closed-kinetic chain test
Participants performed a bilateral IMTP [24], (Fig. 1) and maintained a ‘power position’ with a handheld goniometer measuring knees at 135
Bilateral isometric mid-thigh pull setup.
Unilateral isometric mid-thigh pull setup.
CKC BD was calculated using the equation below. Bilateral PF was calculated by averaging PF for all three trials. Dominant leg and non-dominant leg PF was calculated by averaging PF for the two trials of each leg.
CKC BD
The tests were performed on a Biodex dynamometer (System Pro 4, New York, NY, USA). Participants performed each test unilaterally and bilaterally with order randomized. The dynamometers axis of rotation was aligned with the lateral epicondyle of the knee being tested [25]. The bottom of the lever arm padding was placed just above the medial malleolus of the test leg [25]. The leg moved through a range of motion (ROM) of 90
Familiarization was conducted using a warm up for the quadriceps, isometrically, positioned at 60
Two sets were performed for the concentric knee flexion and extension test at 60
Two sets were performed for the isometric knee extension test with knee angle at 60
Two sets were performed for the isometric knee flexion test with knee angle at 35
Two sets were performed for the eccentric knee extension test at 60
OKC BD was calculated using the equation below. Bilateral PT was calculated by averaging PM of both bilateral isometric knee extension tests. Dominant and non-dominant leg PM was calculated averaging PM of the two isometric knee extension trials of each leg.
OKC BD
Two methods were used to calculate HQ ratios. For the simple, concentric hamstring (H) PM was calculated using the average PT of the two trials during the isokinetic knee extension and flexion tests in both legs. Quadriceps (Q) PM was calculated using the same method. The DCR was calculated using the average PM of the eccentric knee flexion trials in both legs. The PM of Q was calculated using the average from the isokinetic concentric knee extension trials.
Statistical analyses
A 3-way ANOVA (leg
Results
For ratios, there were no 3-way or 2-way interactions or main effect for sex, but there were main effects for leg and ratio. Therefore, data was collapsed across sex for further analysis. The non-dominant leg simple ratio (0.81
For BD, there was an interaction (Fig. 3). Males were significantly greater than females for the OKC but not the CKC.
Means and SD of interaction between OKC and CKC bilateral deficit by sex.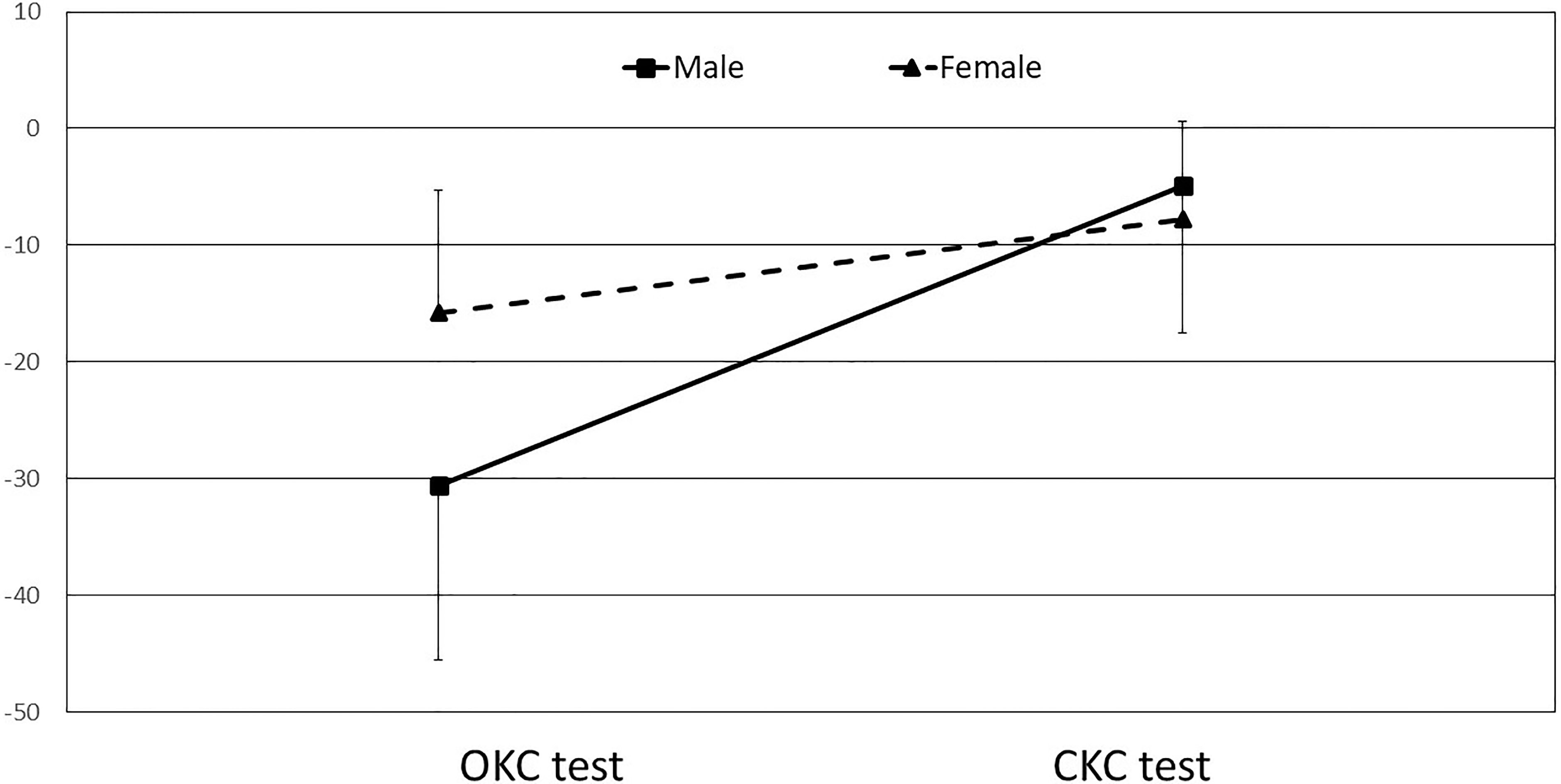
The purpose of this study was to explore the simple and DC ratios between dominant and non-dominant legs and sex as well as to determine the BD between OKC and CKC tests in amateur rugby union players. Greater simple and DCRs were observed in the non-dominant leg compared to the dominant leg and male players showed greater asymmetry for both ratios. This may be due to leg dominance. We classified dominance by kicking a ball, however the role of the hamstrings and quadriceps are much greater for rugby players. Leg dominance can also relate to the preferred push-off leg or deceleration. This may explain why a greater ratio was observed in the non-dominant kicking leg. The OKC BD was significantly greater than the CKC which may be due to OKC isolation of muscle groups as opposed to the CKC where muscles are measured together.
The simple ratio and DCR have been investigated extensively for field based sports [6, 10, 11, 12, 26, 27]. Previous literature has established that a simple ratio of less than 0.6 and a DCR of less than 1.0 may increase the risk of knee injuries [26, 27]. Brown et al. evaluated simple ratios in elite rugby union players and reported similar ratios to those found in the present study [11]. For the simple ratio in the present study, no participant recorded lower than 0.6. However, DCR scores were less than 1.0 in all participants. The DCR has been shown to be more applicable to running due to a reliance on eccentric hamstring strength [6]. Moreover, eccentric hamstring strength has been reported as an important marker against hamstring and other knee-injuries [8, 9]. The low DCR values observed in the present study may be due to the participants amateur status as they may not have been exposed to regular eccentric hamstring strength exercises as professional players are. Also, hamstrings were tested at 60
A previous study examining ratios in elite rugby union players displayed similar asymmetry [11] to that found in the current study. Asymmetries greater than 15% between legs have been associated with increased risk of knee injuries [6, 29]. Males in the current study had asymmetry values for the simple (14%) and DCR (13%) that were close to the 15% cut-off. Sex differences affecting knee strength include lower limb anatomy, hormonal profile, and ligament laxity [30, 31]. Typically, female athletes are at greater risk of knee injuries in comparison to males and show greater asymmetries due to previous injuries [32]. However, male athletes are also susceptible to knee injuries when testing with a DCR asymmetry
Sport success is a delicate balance between high performance and low injury rates. One phenomenon thought to contribute to increased injury rates is a large BD [21, 34]. Loading properties, differing high threshold motor unit activation, movement velocity, and neural drive all contribute to different force and impulse output [19, 21, 35]. The use of OKC exercises to assess BD is well-documented and exhibit a wide range from no deficit to 21% found in the current study [19, 34, 36, 37]. Most notably, Secher et al. [37] found BDs of 18% using the same OKC exercise as the current study. Most athletic events require movement and coordination across multiple joints, therefore CKC may be more sport specific.
Athletic assessments need to be sport-specific, effective and provide the most useful information for strength and conditioning professionals, making a comparison between OKC and CKC tests critical. The OKC test used in the current study produced greater BD than the CKC test. Previous studies investigating biomechanical differences between OKC and CKC tests have found CKC exercises to have increased co-contraction between quadriceps and hamstring muscles, serving to stabilize the knee joint during more complex movements [14, 15]. Activation of more muscle groups could cause compensation by weaker muscles, resulting in less BD.
Hay et al. [35] investigated BD during a dynamic leg press under 100% and 200% body weight conditions, finding slightly greater strength deficits of approximately 16.7% compared to the 6.7% found in the current study. Greater differences could be explained by different loads or the IMTP having to resist additional gravitational forces, and creating postural stability. Pain [38], consistent with our findings, demonstrated that power athletes exhibited an averaged 9.6% BD in jump height using a drop jump protocol. Drop jumps are similar to the IMTP in that they are gravity based.
Conclusion
Amateur rugby union players have greater HQR in their non-dominant legs and male players have greater asymmetry between legs than females. Simple ratio and DCR can result in different values and should be considered carefully in regards to the athlete, sporting demands, and health of the knee. OKC tests show a greater BD than CKC tests due to muscle group isolation. While CKC tests may be more sport-specific, they might mask weaknesses in athletes.
Conflict of interest
The authors declare no conflict of interest of any kind.