
Abstract
BACKGROUND:
After ankle sprains, therapists may use proprioceptive training programs to manage residual symptoms and reduce the risk for recurrent injuries. However, evidence on program effectiveness is limited.
OBJECTIVE:
To investigate effectiveness of balance and proprioceptive neuromuscular facilitation (PNF) programs in individuals with sprain.
METHODS:
Participants were recruited from a rehabilitation center and were randomly allocated to a balance or PNF group. Both groups received 10 training sessions, within a six-week period. Ankle position sense, isokinetic strength and EMG activity were assessed by a blinded investigator at baseline, at the end of training and eight weeks after training. Recurrent injuries were recorded 12 months after training.
RESULTS:
Twenty participants provided follow-up data. Eight weeks after training, significant (
CONCLUSIONS:
For individuals with sprain, balance and PNF programs are recommended for ankle strengthening. They may also be effective in reducing the risk for recurrent injuries.
Keywords
Introduction
Ankle sprains are very common musculoskeletal injuries, and approximately 85% of these injuries are related to the weaker lateral ligaments [1]. After the sprain, most individuals prefer to use a conventional treatment approach [2], comprising early ankle mobilization and weight-bearing, often combined with use of external support, such as tape, brace or bandage. With the exception of complete ligament tears (grade 3), typical prognosis of the conventional treatment is a rapid decrease in disablement within two weeks [2]. However, residual symptoms are often apparent and a high percentage of individuals with conventionally treated sprain still experience pain in the performance of functional and sports activities one year post-injury [2]. It has also been reported that these individuals are predisposed to an increased risk for recurrent injuries and chronic ankle instability [3].
Recurrent injuries and chronic ankle instability are likely to originate from a significant loss of proprioceptive input from mechanoreceptors [4]. Proprioception is a neuromuscular process, including afferent and efferent signals in order to maintain proper positioning of the foot during gait and provide orientation for performance of functional activities [5]. Investigators commonly assess proprioception with the use of joint position sense, and individuals with sprain often exhibit deficits in the position sense of the injured ankle [6]. Moreover, strength of the muscles around the ankle, especially the ankle evertors, is often decreased after the sprain [6]. Therapists should assess and address ankle strength in clinical practice, as potential deficits are related to increased risk for recurrent injuries and chronic ankle instability [4]. In addition, for individuals with sprain, electromyographic (EMG) activities of peroneus longus and tibialis anterior muscles are important for maintaining dynamic stability of the foot [7] and after the sprain they need to sustain within normal range. There are suggestions, and therapists also need to consider that individuals with chronic ankle instability often exhibit deficits in EMG activity of these two muscles [8].
For sprains, it seems that the individuals who exhibit significant deficits in joint position sense, strength and EMG activity of the injured ankle are in increased risk for sustaining recurrent injuries or developing chronic ankle instability [4, 8]. In this context, clinical guidelines recommend participation in proprioceptive training programs after the sprain, which include balance activities and techniques promoting functional movements, to improve ankle strength and coordination [3]. Nevertheless, these recommendations are supported by weak evidence, as the relevant studies are limited and they are characterized by methodological flaws, such as poor description of cohort characteristics, inappropriate managing of missing data and assessment bias [3]. Clinical guidelines also highlight the need for further research into the effects of different proprioceptive training programs in individuals with sprain [3].
For individuals with sprain, research findings indicate that participation in balance and running activities, twice a week, was not able to improve joint inversion sense and strength of the injured ankle [9]. It is of note that, for ankle strengthening after the sprain most investigators have applied protocols of strength and functional training, which included eccentric and resistive exercises [10, 11] and sport-related activities [12], rather than protocols of proprioceptive training [9]. For sprains, eight weeks of ankle disk training also improved the reaction time of the tibialis anterior muscle during sudden simulated inversion perturbations [13]. In addition, most research evidence confirms that balance training, with the use of activities on ankle disk or wobble board, may be effective in reducing future ankle injuries [14, 15, 16].
In clinical practice, therapists use proprioceptive neuromuscular facilitation (PNF) training programs in order to enhance proprioceptors and promote response of neuromuscular mechanisms [17]. The PNF patterns usually have diagonal direction and aim to stimulate the performance of functional movements, using strengthening (facilitation) and relaxation (inhibition) of muscle groups [17]. In PNF literature, programs of PNF training are often used for the rehabilitation of a number of chronic musculoskeletal injuries, including ankle instability [18], low back pain [19] and patellofemoral pain syndrome [20], with goals to improve strength [18, 19] and EMG activity of muscles [20]. To our knowledge, there are no studies investigating the effectiveness of PNF training on ankle sprains. Taking into consideration that PNF techniques have also been used to improve joint position sense in healthy individuals [21], we hypothesized that PNF training may improve ankle position sense, strength and EMG activity in ankle sprains. For individuals with sprain, balance training can be used prophylactically in an effort to reduce future ankle injuries [14, 15, 16]. It would be beneficial to elucidate for the first time comparative effectiveness of PNF training on recurrent injury rate. The aims of this study were to investigate the effects of two supervised proprioceptive training programs, balance and PNF, on ankle position sense, strength, EMG activity and recurrent injury rate in individuals with post-acute ankle sprain.
Methods
Our study was undertaken in conformity with the Code of Ethics of the World Medical Association (Declaration of Helsinki), printed in the British Medical Journal (18 July 1964). This was a randomized two-group, pre-post treatment design, with a blinded assessor. The study was prospectively registered at a clinical trial registry (ID: NCT01853462).
Participants
Participants for the study were recruited from a rehabilitation centre, and a total of 34 individuals were initially invited to participate. These individuals exhibited a post-acute ankle sprain (mean: 11 weeks since sprain) and they experienced pain in the performance of functional or sport activities. For inclusion, it was required that the individuals had a clinical diagnosis of ankle sprain by an orthopedic specialist and they had not participated in any form of supervised training after the injury. The following exclusion criteria were also defined: chronic ankle instability, grade 3 ankle sprain, medial or interosseous (syndesmotic) ligament ankle sprain, concurrent fracture, history of nerve injury or ankle surgery to the lower limbs and further ankle injury after the sprain. Individuals with any injuries that impeded participation in the training sessions of the study were also excluded.
The principal investigator initially screened the eligibility criteria of our study, via an interview. All prospective participants were instructed to show for consideration all clinical documentation and diagnostic testing findings related to the ankle sprain in order to confirm the grade and ligaments affected. Suitability for participation was confirmed by an orthopedic specialist, who also obtained a medical history of the sprain. Information concerning aetiology and mechanism of injury, symptoms and conventional treatment of choice were recorded. In addition, the principal investigator performed a clinical examination of the injured ankle including palpation and assessment for the presence of swelling, hemorrhaging, tenderness and ligament laxity. Range of motion and strength were also assessed manually, compared to the uninjured ankle. During the screening procedure, the investigators were blinded to the group allocation of participants and concealed allocation was attained. According to the inclusion and exclusion criteria of the study, 12 out of the 34 initially invited individuals with sprains were excluded, and 22 individuals were eligible for participation. Prior to participation, verbal explanations and written information sheets concerning the study protocol were provided to all individuals, who then signed a consent form, approved by the university ethics committee. The principal investigator collected demographic and anthropometric data for each participant, and information concerning the sprain and level of sports activity were also recorded.
Participants were allocated to one of the two groups by a statistician, who was blinded to the aims of the study, using computer generated number lists. Stratified randomization was implemented, ensuring that the balance and PNF groups were balanced for gender, sprain history to the injured ankle and sports activity level. For sports activity, high level was defined as participation in sports for more than 3 hours per week [22]. After initiation of the study, two female participants discontinued training, due to increased professional commitments (balance group) and non-related lower back injury (PNF group), and 20 participants completed the intervention.
Testing procedures
An independent investigator, blinded to the group allocation of participants, was responsible for the assessment of outcomes. For ankle position sense, strength and EMG activity, each assessment session lasted between 60 and 70 minutes. In order to minimize the effects of fatigue on testing procedures, joint position sense was assessed first and strength and EMG measurements followed. A second day, the same investigator collected data concerning pain, ankle range of motion (ROM), functional and balance performance, as part of an additional study performed by our research team [23]. Data were collected at baseline, at the end of training (follow-up 1) and eight weeks after training (follow-up 2). For potential recurrent ankle injuries, data were collected 12 months after training.
Joint position sense
A Biodex System II Pro isokinetic dynamometer (Biodex Medical; Shirley, NY) was used to assess active joint position sense at the sprained ankle, for three test positions: 10
Initially, the instigator moved the foot through the complete non-painful plantar flexion and dorsiflexion ROM for each participant, and then to the test position, where it was held for 15 sec [25]. Each participant received instructions to concentrate to that position and reproduce it in the assessment. The investigator then moved the foot to the extreme opposite non-painful ROM (i.e. to plantar flexion for the dorsiflexion test position, and to dorsiflexion for plantar flexion test positions). Participants were then requested to actively move the foot in order to reproduce the test position, and push a stop button immediately when they thought that the test position was matched. Prior to testing, participants were informed concerning the applied protocol and a practice session was performed, followed by 30 sec of rest [25].
Muscle strength
The Biodex dynamometer was used for the isokinetic testing of the sprained ankle, and peak torque scores were recorded in Nm. Initially, testing was performed for dorsiflexion-plantar flexion, and afterwards for eversion-inversion, at controlled 30
One isokinetic test comprised five cycles of maximal concentric muscle contractions, at test velocity. For each test velocity, peak scores were used for the analysis. During a cycle, each participant moved his/her sprained ankle through the complete, non-painful ROM of the tested movement: from complete plantar flexion to complete dorsiflexion and back to complete plantar flexion, and from complete inversion to complete eversion and back to complete inversion. Prior to testing, ROM limits were set for each participant including all movements of the ankle. Gravity torque was also recorded with ankle in neutral position and it was used to correct isokinetic ankle plantarflexion/dorsiflexion torque. In addition, each participant performed five submaximal cycles of practice at test speed in order to familiarize with the procedure, and a 2 min rest period followed until the initiation of testing [26]. For lateral ankle sprains, the test-retest reliability of isokinetic testing has demonstrated intra-class correlation coefficients between 0.89 and 0.92 for eversion at 120
Electromyographic activity
Surface EMG data were recorded for peroneus longus and tibialis anterior muscles of the sprained ankle, during isokinetic testing at 30
A Shimmer3 EMG Unit (Dublin), which acquired signals at 1024 Hz, was used for collection of EMG recordings. The input impedance of the differential amplifier was 22 megaohms, with 110 dB common mode rejection ratio and a signal-to-noise ratio of 0.75 dB. The investigator stabilized two EMG units to the tested limb with straps and connected each unit with the electrodes of a muscle. The third EMG unit was attached to the arm of the dynamometer and it was used as an accelerometer to define precisely the initiation of movement. For the normalization of EMG signals, EMG activity of the specified muscle during maximal voluntary isometric contraction (MVIC) was used as a reference value. Prior to isokinetic testing, each participant performed three 5 sec MVICs for each muscle, and there was a 30 sec rest between two MVICs. For the peroneus longus muscle, EMGs were recorded during MVICs of the evertor muscles. For the tibialis anterior muscle, EMGs were recorded during MVICs of the dorsiflexor muscles. During performance of MVICs, the position of participants was the same with strength isokinetic testing, and ankle and subtalar joints were in neutral position. For the MVICs, the resistance was provided by the Biodex ankle apparatus, in relation to the tested muscle. For each muscle, prior to performance of MVICs the investigator emphasized that maximal effort was required for each muscle contraction, and all participants performed one practice trial so as to familiarize with the procedure. During testing, verbal reinforcement was provided to all participants. Prior to isokinetic testing, a 3 min rest was included.
The MyoResearch XP software package (Noraxon Inc., Scottsdale) was used for analysis of EMG data. Analog to digital converters provided digital representation of the EMG input analogue signals into the computer by a 24-bit signed integer value to each sample, using Bluetooth. A Butterworth band-pass filter was applied at 8 Hz and 500 Hz, using a full-wave rectification. Smoothing was performed using the root mean square of the rectified signal. During strength testing, the three contraction cycles producing the greatest amount of EMG activity at test velocity were identified, and the mean score (in mVolts) was computed for the normalization of EMG data. For data normalization, the mean score of the MVICs of the peroneus longus and tibialis anterior muscles producing the greatest amount of EMG activity was also used. The normalized data were used for further analyses.
Recurrent injury rate
The independent assessor contacted all participants by telephone, 12 months after training, and recorded potential recurrent injuries to the ankle.
Training procedures
Within a six-week period, the same physiotherapist provided 10 supervised training sessions to all study participants, at a rehabilitation research laboratory. Each session lasted 50 to 60 min, and participants received clear instructions to discontinue a session since they experienced significant pain or fatigue. For both groups, training ended with 4 min of walking on toes and heels, in forward and backward directions, with 60 sec in-between rest. Participants were directed to abstain from any form of additional training during the study.
Balance protocol
The balance protocol was designed according to the rehabilitation guidelines of ankle sprains in clinical practice [3]. The protocol consisted of wobble board, firm surface and soft surface activities, with the eyes open. Initially, participants performed wobble board exercises on both legs, for 7 min, with no rest intervals. During training, feet were parallel and participants were instructed to balance, while moving board’s edge at saggital plane (back to front), frontal plane (left to right) and circulating directions. Moreover, each participant tried to stand on the wobble board for 15 sec, using only the sprained leg. The sprained-leg stance exercise included 16 repetitions, and there was a 30 sec rest after 4 repetitions.
The activities on firm surface (floor) involved performance of 40 squats on the sprained leg, with 6 sec duration per squat. The depth of squats was dependent on the exercise tolerance of each individual. Following eight squats, 30 sec rest was provided. In addition, participants performed a distance hop series exercise, using the sprained leg. This exercise consisted of 6 hops in primary and diagonal patterns, and balance was maintained for 5 sec after each hop. The distance hop series exercise comprised 8 repetitions, with 30 sec rest after each repetition. For activities on soft surface, a foam pad was utilized, and participants tried to balance using the sprained leg, while performing resistance band exercises with the opposite leg. The duration of the soft surface exercise was 15 sec, and 16 repetitions were performed, with a 30 sec rest after 4 repetitions. Moreover, 60 sec and 2 min rest intervals were included after each exercise and between different training activities, respectively. Apart from the hop series exercises, balance training was performed without footwear. The wobble board and foam pad used in our study were of Thera-Band equipment (Akron, Ohio).
PNF protocol
The PNF protocol comprised two different techniques: rhythmic stabilization (RS) and combination of isotonics (COI) [19]. During application, participants were in supine position, on a treatment table, facing the therapist. The PNF protocol was applied to the sprained leg, with the knee in extension, for both diagonals of the lower extremity, at the end of the upper and lower range of each diagonal. The therapist provided maximal resistance, according to the needs of each individual. In order to emphasize training of the foot and ankle, timing for emphasis was implemented and the therapist prevented all hip and knee motions of the performed PNF pattern. The position of the therapist’s hands was contingent on the technique and diagonal under application and conformed to the PNF principles.
The RS technique was applied first and comprised alternating isometric muscle contractions of agonistic and antagonistic muscles, against resistance, with 10 sec total duration and no intended motion [19]. The COI technique was applied after 2 min and it included combined concentric, stabilizing and eccentric contractions of agonistic muscles, with no rest between contractions [19]: resisted active concentric contraction for 5 sec, resisted isometric contraction for 5 sec and resisted eccentric contraction for 5 sec. For both RS and COI techniques, each set included 5 to 15 repetitions, according to the endurance of each individual [3]. Maximal effort was requested for all repetitions. Rest intervals of 30 sec were included between sets. The duration of each technique was 20 min, including rest intervals. Prior to application, the therapist provided clear instructions concerning the correct performance of each PNF technique to the specified diagonal.
Statistical analysis
For joint position sense, muscle strength and EMG normalized data, the non-parametric Friedman test was used to determine the within-group differences of each outcome measure across the assessment time points. The significance level was
Characteristics of participants in each group
Characteristics of participants in each group
Mean (SD) balance group scores and Friedman test results across time points for joint position sense (degrees of error)
Mean (SD) PNF group scores and Friedman test results across time points for joint position sense (degrees of error)
Table 1 shows the characteristics of the 20 participants who completed the intervention; these were similar between the balance and PNF groups. At baseline, no significant (
Mean (SD) balance group scores and Friedman test results across time points for peak torque (Nm)
Mean (SD) balance group scores and Friedman test results across time points for peak torque (Nm)
Mean (SD) PNF group scores and Friedman test results across time points for peak torque (Nm)
For joint position sense, post hoc tests indicated that the balance group significantly improved against baseline for 15
Both groups significantly (
No significant (
Mean (SD) normalized peroneus longus EMG activity across assessment time points for balance and PNF groups, during ankle plantar flexion testing at 120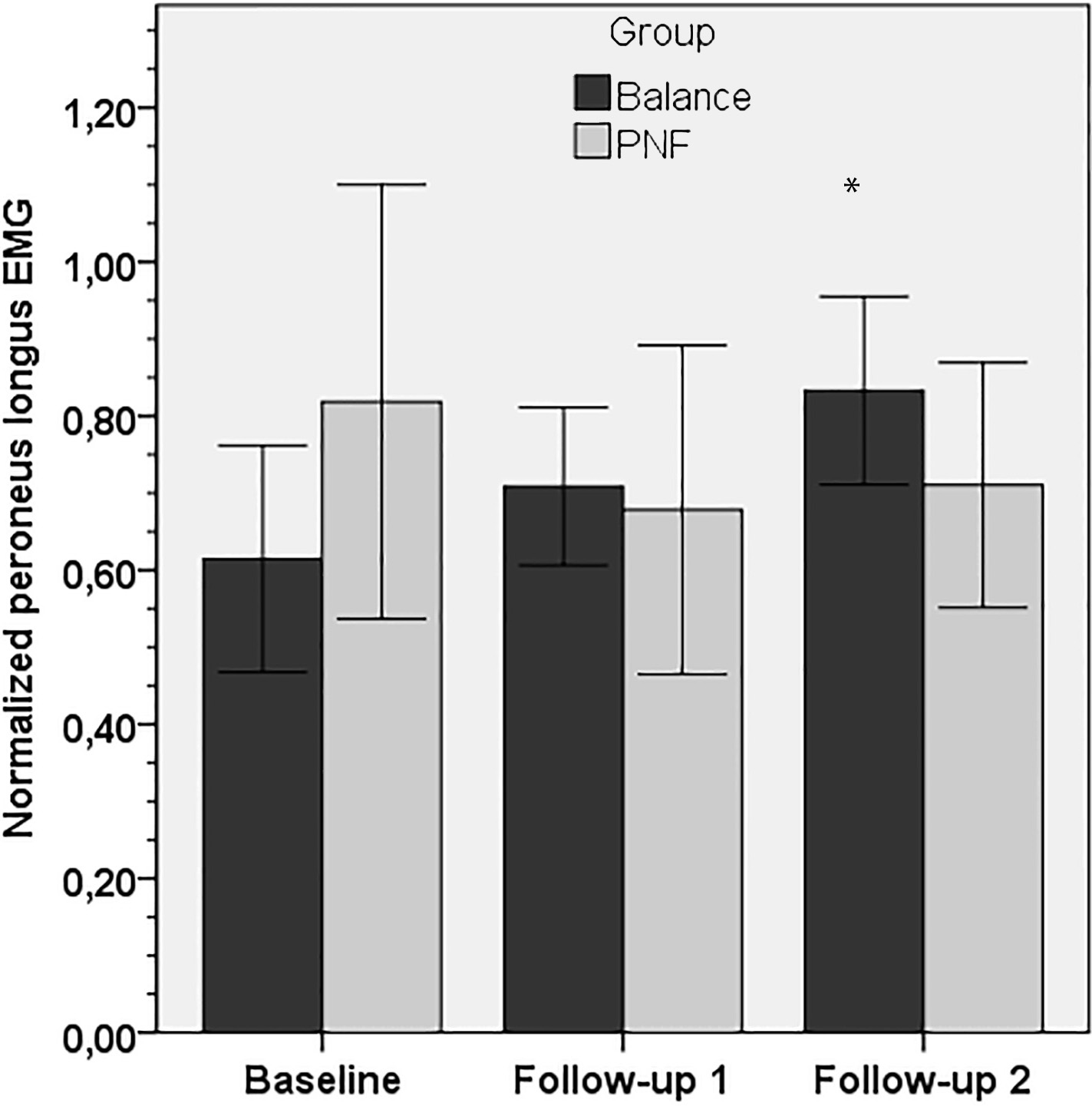
Mean (SD) normalized tibialis anterior EMG activity across assessment time points for balance and PNF groups, during ankle inversion testing at 30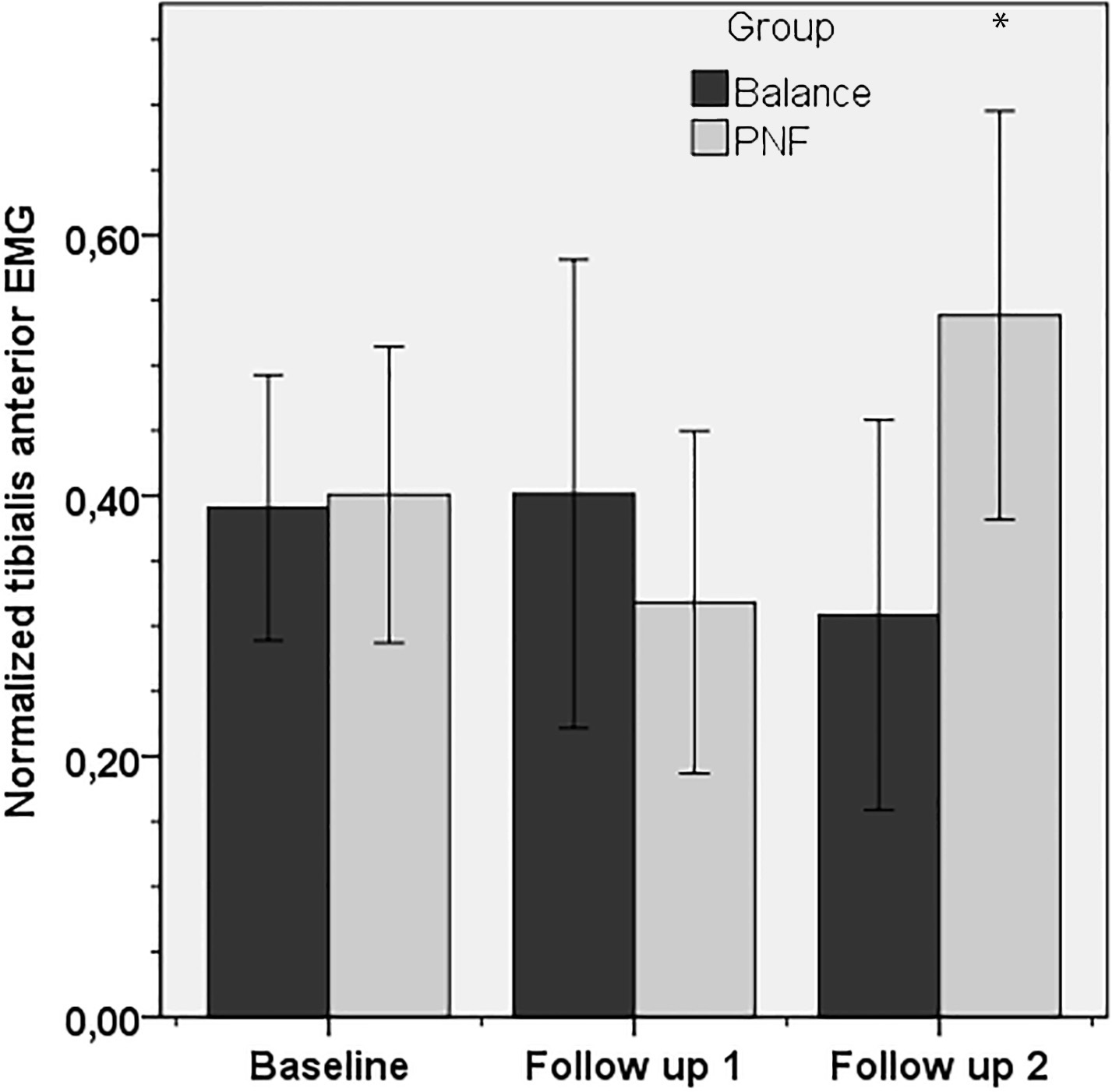
For the peroneus longus muscle, the balance group exhibited no significant (
For EMG activity, most between-group differences against baseline were not significant (
No recurrent ankle injuries were observed for the balance group. For the PNF group, 20% of the participants (two females with high sports activity level and sprain history to the injured ankle) sustained a recurrent sprain to the lateral ankle ligaments within 12 months after the intervention. Although the recurrent injury rate differed between balance and PNF groups, this difference was not significant (
The main finding of this study is that both balance and PNF training programs are effective in strengthening the ankle muscles. In addition, they may be effective in reducing recurrent ankle injuries. In addition, eight weeks after training the balance program improved ankle plantar flexion sense and EMG activity of the peroneus longus muscle during plantar flexion strength testing. Eight weeks after training, the PNF program improved EMG activity of the tibialis anterior muscle during inversion strength testing, but there was no improvement for ankle position sense. For all significant improvements, the effect sizes were large indicating clinical significance.
In our study, there were no significant changes after training in most measures of joint position sense, for both balance and PNF groups (Tables 2 and 3). However, for the balance group we found significant improvement for 15
Joint position sense is the ability to replicate positions of a joint using active or passive movement cues. The active replication of joint positions is thought to measure activity in the muscle spindle receptors [5]. Hence, increments in the activity of the muscle spindle receptors may explain the improvements in active joint position sense observed in our study. In our study, we assessed joint position sense in a not weight-bearing position. As the magnitude of mechanical stress that is imposed on a joint is significantly different between weight-bearing and non-weight-bearing activity [5], the non-significant findings for the balance group in our study might be justified by the specificity of the applied protocol, which included solely performance of weight-bearing exercises. This, however, was not the case with PNF protocol, as participants in the PNF group performed exercises in non-weight-bearing positions and similarly there were no significant changes in most joint position sense measures after training. Further studies investigating the effectiveness of balance and PNF programs on ankle position sense in individuals with ankle sprain should be conducted.
In our study, eight weeks after training both groups improved ankle inversion and plantar flexion strength, but there was no improvement in dorsiflexion strength (Tables 4 and 5). Eight weeks after training, solely the balance group improved ankle eversion strength. In concordance with our findings, evidence in individuals with sprain confirms improvement in eversion strength after participation in strength and functional training, including eccentric exercises [10, 11] and soccer-specific activities [12]. In addition, participation in programs including eccentric and resistive strength exercises for a six-week period improved ankle inversion strength in individuals with sprain [11]. A two-week functional training program of soccer-specific activities also improved plantar flexion strength of an athlete with ankle sprain [12]. Although these findings confirm conclusions in our study, it should be mentioned that investigators in most of these studies applied protocols of strength training. In our study, we applied two protocols of proprioceptive training, balance and PNF, and most measures of ankle strength also improved after training for both protocols. These findings confirm the strengthening ability of balance and PNF protocols in sprains and recommend their use in clinical practice for ankle strengthening, as an additional approach to strength protocols to obtain optimal results.
For ankle sprains, Holme et al. [9] assessed the effects of proprioceptive training on muscle strength of the injured ankle. In opposition to our conclusions, the investigators found no gains in isometric ankle strength four months post-injury for the individuals who participated in balance and running activities, against a control group of conventional treatment [9]. However, Holme et al. [9] assessed effectiveness in relation to the uninjured ankle and there were no baseline measurements due to the acute phase of the sprain. Owing to absence of pre- and post-intervention effects, comparisons with our study should be made with caution. Concerning the application of PNF protocols, Hall et al. [18] have recently investigated the effects of the slow reversal PNF technique, which consists of a concentric contraction of antagonistic muscles followed by a concentric contraction of agonistic muscles [17], on isometric ankle strength in individuals with chronic ankle instability. After PNF training for six weeks, strength improved for inversion and eversion, but there were no improvements for dorsiflexion and plantar flexion [18]. In our findings, the PNF group showed no significant improvement in dorsiflexion and eversion strength measures, eight weeks after training. We hypothesize that during the application of PNF patterns in our study, the investigator failed to provide an adequate amount of manual resistance in dorsiflexion and eversion directions in order to induce a significant change. In clinical practice, PNF therapists should consider the utilization of additional open and closed kinetic chain exercises to improve strength for ankle dorsiflexion and eversion.
In our study, we recorded EMG activities of the peroneus longus and tibialis anterior muscles during isokinetic testing of the ankle. Eight weeks after training, EMG activity of the balance group significantly improved during plantar flexion at 120
Ankle sprains to the lateral ligaments are inversion injuries that occur in the plantar-flexed position. It has been reported that peroneus longus and tibialis anterior are the first muscles to contract in response to such injurious perturbations [13]. In this context, it could be suggested that EMG activities of peroneus longus muscle-during eversion isokinetic testing- and tibialis anterior muscle-during dorsiflexion testing- are important for the prevention of recurrent lateral ligament sprains. In our study, eight weeks after training we recorded no significant changes in EMG activity of these muscles during eversion and dorsiflexion testing. Nevertheless, our findings reveal the roles of the peroneus longus and tibialis anterior muscles as ankle plantar flexor and invertor muscles, eight weeks after balance and PNF training, respectively. For ankle sprains, research concerning effectiveness of various proprioceptive training programs on EMG activity of the ankle is necessary.
The recurrent rate of ankle sprains is noteworthy and most patients with a history of ankle sprain will sustain at least one additional sprain in the future [30]. These recurrences increase disability and lead to chronic ankle instability and pain in 20% to 50% of cases [31]. For sprains, the high rate of recurrent injuries and the associated risk for chronic instability and pain highlight the importance of using effective training programs in clinical practice. In our study, 12 months after sprain, there were no recurrent injuries for the balance training group, whereas for the PNF training group the recurrent injury rate was 20%. Although relevant evidence is not unanimous [31], most systematic reviews and randomized clinical trials in individuals with ankle sprain confirm our findings, indicating that the balance training programs, with the use of an ankle disk or wobble board, can be used prophylactically in order to reduce recurrent injuries [14, 15, 16]. It has also been reported that the six-week balance protocols may be effective in reducing recurrent injuries for up to one year [14]. This is in agreement with our study. To our knowledge, this is the first study investigating the effects of PNF training on recurrent injuries after the sprain. Our findings indicate that the rhythmic stabilization and combination of isotonics techniques, when applied in combination, could be effective in reducing the risk for recurrent ankle injuries. For this purpose, we recommend their use in clinical practice as alternative approach to balance training.
In our study, we hypothesize that the applied balance and PNF protocols induced adaptations in ankle neurophysiology and morphology, as demonstrated by the improvements observed for plantar flexion position sense, strength and EMG activity of the ankle. Potential neurophysiological adaptations are changes in various physiological processes, such as the sensory appreciation of specific peripheral mechanoreceptors, nerve conduction velocity, pool excitability of alpha motoneurons and gamma-efferent motor activity in muscle spindles [5, 31]. Possible adaptations in morphology are changes in the cross-sectional area of muscles, size of myofibrils and/or structure of ligaments [31]. It could be suggested that proprioceptive training in our study increased the motor control and coordination of participants during the performance of functional or sport activities and as a consequence, recurrent injuries were effectively prevented. The mechanisms through which proprioceptive training programs may prevent recurrent ankle injuries are still unclear [31]. Implementation of enhanced assessment techniques seems beneficial for investigating these mechanisms.
This study is not without limitations. We used a relatively small number of participants in each group (
Conclusion
This study shows clinically significant improvements in ankle strength after ten 50–60 min sessions of supervised balance or PNF training programs in individuals with sprain. In addition, 12 months after training, there were no recurrent injuries for the balance group and 80% of participants in the PNF group were free of further injuries. Eight weeks after training, clinically significant improvements were found for the balance group in ankle plantar flexion sense and EMG activity of the peroneus longus muscle during plantar flexion strength testing; the PNF group also improved EMG activity of the tibialis anterior muscle during inversion strength testing. For individuals with sprain, further studies investigating effectiveness of balance and PNF training programs should be conducted to confirm these findings.
Conflict of interest
No financial support was obtained for this research project and the authors claim no conflict of interest.