
Abstract
BACKGROUND & OBJECTIVE:
Outcomes of the pandemic COVID-19 varied from one country to another. We aimed to describe the association between the global recovery and mortality rates of COVID-19 cases in different countries and the Human Development Index (HDI) as a socioeconomic indicator.
METHODS:
A correlational (ecological) study design is used. The analysis used data from 173 countries. Poisson regression models were applied to study the relationship between HDI and pandemic recovery and mortality rates, adjusting for country median age and country male to female sex ratio.
RESULTS:
During the first three months, the global pooled recovery rate was 32.4%(95%CI 32.3%–32.5%), and the pooled mortality rate was 6.95%(95%CI 6.94%–6.99%). Regression models revealed that HDI was positively associated with recovery β= 1.37, p = 0.016. HDI was also positively associated with the mortality outcome β= 1.79, p = 0.016.
CONCLUSIONS:
Our findings imply that the positive association between the HDI and recovery rates is reflective of the pandemics’ preparedness. The positive association between the HDI and mortality rates points to vulnerabilities in approaches to tackle health crises. It is critical to better understand the connection between nations’ socioeconomic factors and their readiness for future pandemics in order to strengthen public health policies.
Keywords






Abbreviations:
World Health Organization
coronavirus disease 2019
Public Health Emergency of International Concern
Gross Domestic Product
Human Capital Index
Domestic General Government Health Expenditure
The Human Development Index
Bacillus Calmette-Guérin
Introduction
On 30 January 2020, the World Health Organization (WHO) declared coronavirus disease 2019 (COVID-19), a Public Health Emergency of International Concern (PHEIC), and on 11 March 2020, as a pandemic [1]. COVID-19 pandemic can be viewed beyond a global health problem; it can be regarded as a global human developmental crisis that affects socio-economic development of nations [2]. The pandemic is much more than a worldwide public health emergency; it is a universal human development crisis, reflecting our interaction with the ecosystem we are part of [3]. The continuation of this unprecedented global emergency affected many essential aspects of life and among the groups affected: families, youth, women, and students where many things had to be changed in their life [4, 5].
There are substantial variations between countries when it comes to COVID-19 detection and mortality rates, which appear to be highest in the United States and lowest in some Asian countries [4]. These variations exist even within different regions of individual countries [6]. Numerous authors have provided possible explanations for these variations, which ranged from individual-related factors (age, gender, race, ethnicity, smoking status, presence of chronic lung disease, and level of vitamin D3 or its supplementation), [7–15] environmental measures (temperature, humidity, level of pollution and ultraviolet radiation) [16–22] or country factors (population density, population mobility, geographical location in the form of latitude and timing or type of country-based mitigation measures such as testing) [23–32].
The socioeconomic approaches of assessing the associations between a country’s development and the epidemiology of COVID-19 are very scarce, particularly for outcomes of infections. Data derived from recent and historical studies on previous pandemics, including the influenza pandemics in 1918 and 2009, suggest that country-level socioeconomic factors can affect detection rates and clinical outcomes [33–35]. Accordingly, factors such as the age of the population, race, affluence, inequality, poverty, unemployment, insurance, or access to healthcare may account for these between-country or between-region variations [36]. Buja et al. (2020) identified several socioeconomic factors (rates of employment and public transportation usage) associated with significant differences in the rate of COVID-19 spread in 36 provinces of Northern Italy [37]. A similar publication identified other socioeconomic factors (age distribution, male to female ratio, and low-income) associated with significant differences in the number of detected COVID-19 cases in 177 neighbourhoods in New York City [38]. A study from the United Kingdom implicated the in-house density as the source of variation [39]. These publications examined individual socioeconomic factors in isolation and did not scrutinize the effect of several socioeconomic factors together. Furthermore, they investigated the association with the COVID-19 detection rate and did not consider clinical outcomes such as recovery and mortality rates. Further, a publication from Brazil evaluated the effect of several socioeconomic variables on COVID-19 exponential growth-phase infection and mortality rates across 36 countries. It demonstrated no associations with the Gross Domestic Product (GDP) per capita, Human Capital Index (HCI), or Domestic General Government Health Expenditure (GGHED) per capita [40]. This contradicts the findings of an American study that collected COVID-19 pandemic infection data and social-ecological data of 178 countries and found that the GDP per capita was significantly positively associated with cumulative mortality rates of COVID-19 [41].
The Human Development Index (HDI) is a composite marker of life expectancy, education, and per capita income indicators, which are utilized to classify countries into four tiers of human development [42, 43]. The psychometric properties of this measurement tool have been published [44]. The focus of HDI is to measure average achievements in human development in a society and is often used by countries as part of their long-term national strategic planning [45]. It has several components, such as life expectancy at birth, mean years of schooling; and, gross national income per capita. HDI is used to determine the relationship between the socioeconomic development of countries and the incidence of diseases. Several studies have examined the association between the HDI and the epidemiology of both communicable and non-communicable diseases, but none has focused on the epidemiology of COVID-19 [46].
Identifying socioeconomic variables associated with COVID-19 is vital for public health systems to guide mitigation strategies to improve health outcomes in a given area as part of ongoing global efforts to contain the pandemic and to drive future approaches that may tackle the possible resurgence of the disease [6, 37].
The objectives of this study were to describe the association between global recovery and mortality rates of COVID-19 cases and the HDI in different countries, attempt to explain the variation between-countries and determine the association between the global recovery and mortality rates of COVID-19 cases, and the HDI in different countries after adjusting for age and sex during the first three months of declaring it as a PHEIC.
Methods
Study design
A correlational (ecological) study design. The unit of analysis was the country. The study design served to make inferences about the ecological effects of HDI status on country-level mortality and recovery rates. It is not our intention to make inferences about the biological effects on individual disease risks [47, 48]. It permits performing comparisons using available country-level secondary data that may not be feasible to obtain at the individual-lever with the available time and resources.
Data sources
A total of 173 countries were included in the analyses. Inclusion criteria were: 1) the country has an HDI value for the year 2019 published in the Human Development Report (HDR)/United Nations [49], and 2) the country has secondary data on the COVID-19 pandemic, which include the total number of COVID-19 cases, number of recovered COVID-19 cases, number of deaths from COVID-19 and made available at world meter: coronavirus live update [50]. Secondary data on the median age and sex ratio per country were obtained from the United Nations –Department of Economics and Social Affairs [51].
For each country, the global recovery rate and global death rate were calculated by dividing the number of recovered/dead cases by the total number of reported COVID-19 cases. For modelling, the log transformation of the number of recoveries and the number of deaths was made. All data were accessed on 2 May 2020.
Data analyses
Poisson regression analysis models were used to study the association between COVID-19 outcome rates and HDI and to adjust for demographics (median age and male: female ratio) and country-level parameters. The following model for the number of observed recovered cases and the number of observed deaths was used: (μc) to COVID-19 virus was specified: log(μc) =β0 +β1*HDI +β2*median age +β3*male to female ratio + uc. In the equation, c stands for the country.
We repeated the analyses stratifying for the HDI rank categories; the following were used: very high, high, medium, and low human development.
All regression estimates and corresponding 95%confidence intervals (CI) and p-values were reported. The level of significance was considered less than 0.05. All data were analysed using Stata software version 16.1 (StataCorp, College Station, TX, USA). The Poisson model was fitted via the Poisson command.
Poisson regression is a type of regression analysis that uses a generalized linear model to describe count data and contingency tables. The response variable Y is assumed to have a Poisson distribution, and the logarithm of its anticipated value may be described by a linear combination of unknown factors in Poisson regression. When used to model contingency tables, a Poisson regression model is also known as a log-linear model [52].
Results
Within the first three months of the pandemic, there were about 3.5 million cases, with 1.1 million recoveries and approximately 250 thousand deaths. The global recovery rate was 32.4%(95%CI 32.3%–32.5%) and global mortality rate was 6.95%(95%CI 6.94%–6.99%).
Table 1 presents the associations between the global outcomes of COVID-19 and HDI. A total of 168 countries were analysed for the recovery rate and 152 for the mortality rate. Poisson regression models revealed that HDI was positively associated with the log recovery rate after adjusting for age and sex β= 1.37, p = 0.016. HDI was also positively associated with the log mortality rate after adjusting for age and sex β= 1.79, p = 0.016.
The association between the outcomes of COVID-19 and HDI
The association between the outcomes of COVID-19 and HDI
*Significant at 0.05 adjusting for median age and sex ratio.
After stratifying for the HDI rank categories, there were data from 61/62 (98.5%) countries from the very high human development, 49/55 (89%) countries from high human development, 29/37 (78.5%) countries from the medium human development, and 34/36 (94.5%) countries from low human development.
Figure 1 graphically depicts the association be-tween the COVID-19 recovery rate and HDI, and Figure 2 portrays the association between the COVID-19 mortality rate and HDI. For very high human development, the pooled recovery rate and the pooled mortality rate were 29.1%and 7.3%, respectively. The pooled recovery rate and pooled mortality rate were 52.8%and 5.5%, respectively, for countries with high human development. The corresponding values for the medium human development were 32.3%and 2.9%, respectively, and for those with low human development 27.2%and 2.9%, respec-tively.
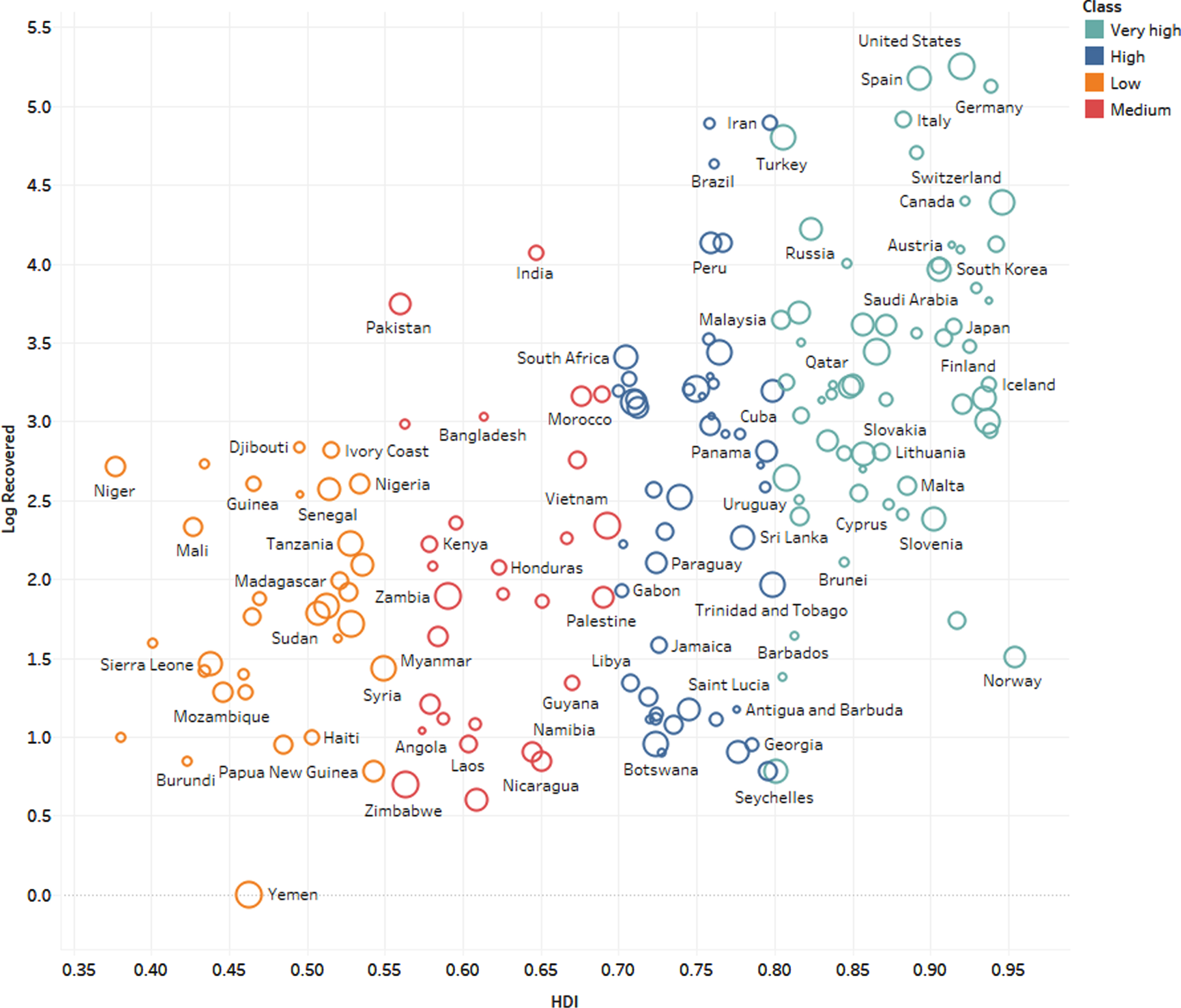
The COVID-19 recovery rates by HDI classes.
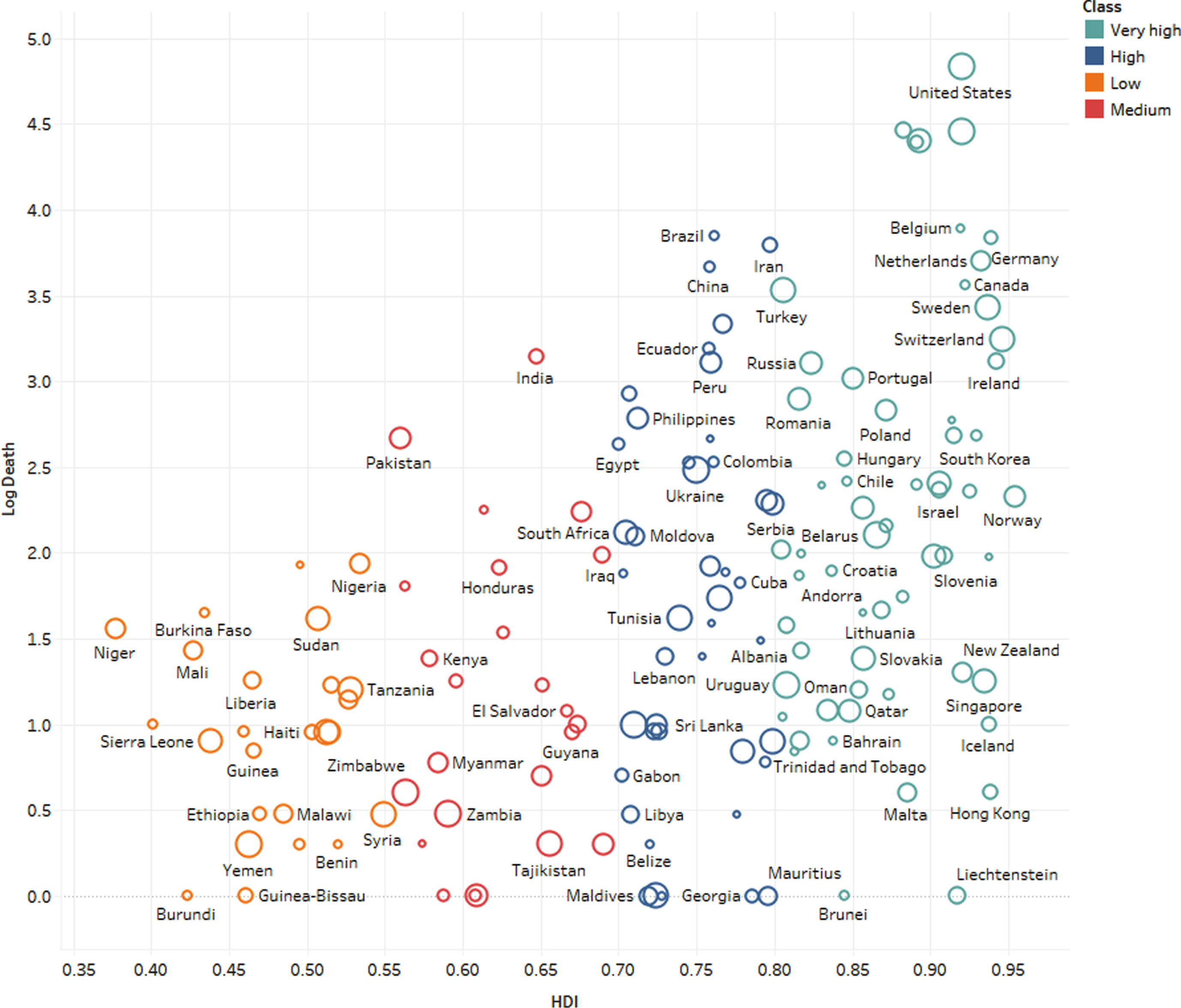
The COVID-19 mortality rate and HDI classes.
Table 2 presents the distribution by the HDI classification of COVID-19 recoveries, COVID-19 deaths, all-cause deaths, and total population. Very high HDI countries represent 16.2%of the world population, and their share in expected deaths from all causes is 18.6%; however, their share in COVID-19 deaths was 87.7%at the time of the study.
Distribution by human development index classification: COVID-19 recoveries, COVID-19 deaths, all-cause deaths and total population (percent)
Note: Data until 2 May 2020. Deaths from all causes extrapolated to 2020 with the 2016 crude mortality rate. COVID-19 data is reported for 173 countries, shares to all-cause deaths, and the total population include all countries of the world.
The World Health Organization has laid forth a timeline of pandemic stages. Interpandemic, “alert, pandemic, and transition are the four phases [53]. The stages of the pandemic risk assessment coincide with the phases of the continuum. The three steps of the risk assessment are preparedness, response, and recovery.
In this study, we attempted to assess the potential country-level determinants of COVID-19 recovery and mortality rates and explain the between-country variations assuming reasonably that surveillance systems and reporting fatalities were accurate and comparable. Our findings imply a significant positive association between the HDI and both the recovery and mortality rates.
It is expected that countries with a lower HDI will claim a high share of COVID-19 mortality [40, 54–56]. A high proportion of the urban population in countries with a lower HDI live in high-density areas such as slums, favelas, and camps where associated restrictions against personal freedom or primary economic needs (e.g., gaining access to food or water) may prove a potentially severe humanitarian crisis following exposure to an epidemic [54, 57]. Therefore, flattening the curve on COVID-19 may prove to be more difficult, resulting in higher case fatality. Moreover, health systems in low-income countries that face severe constraints in normal times regarding staffing and medical equipment are unlikely to possess the capacity to cope with the surge in demand, especially for those needing respiratory support [58, 59]. However, our data suggest that the mortality rate was higher in countries with a higher HDI.
Countries will have to make difficult decisions in the future. Individual responses to guidance on how to best avoid transmission will be as essential, if not more so, than official initiatives [60].
Although many aspects of the COVID-19 infection remain uncertain, it has been demonstrated that mortality trends are higher in older populations and males [14, 61–63]. The higher death rates from COVID-19 deaths in high-income counties were explained by the higher proportions of elderly populations [64]. However, in this report, we corrected both age and sex to account for these potential confounders. Moreover, developing countries with a lower HDI have been aging at a fast pace as it has been estimated that low- and middle-income countries contain 69%of the global population aged more than 60 years [13, 65]. Developing countries have noticeably more older people than the high-income countries, with the more than 70 years population being 1.8 times higher and the more than 60 years population 2.4 times higher than in high-income countries [64]. Therefore, age does not appear to be the reason behind the low shares of countries with a lower HDI in the global mortality of COVID-19.
To the best of our knowledge, the correlation between heterogeneity in healthcare and economic resources and COVID-19 related outcomes has been generally overlooked. A positive association has been reported in mainland China [66] and in Italy [67]. Lippi and colleagues found Spearman’s correlation coefficient of r = 0.53 between gross domestic product at current prices per inhabitant and toll of deaths in the 21 Italian regions and provinces. We have further expanded these analyses at the global level, both for COVID-19 infection incidence and mortality rates.
The current analysis is still preliminary because data about several confounders are lacking. We did not account for comorbidities, Bacillus Calmette-Guérin (BCG) vaccination status, or air quality. Comorbidities have been shown to increase the mortality of COVID-19 [68]. A recent global meta-analysis identified hypertension, respiratory system disease, and cardiovascular disease as risk factors for severe COVID-19 [69]. However, this covariate is unlikely to explain the increased mortality in countries with a high HDI, as comorbidities are very common in the developing world. A recent WHO report revealed that of 1.1 billion persons with hypertension, almost two-thirds reside in developing countries [70]. Moreover, the prevalence of diabetes is quickly rising in developing countries [71]. The lack of necessary basic level of health infrastructure in developing countries would entail that several diseases would be left untreated or under-treated, intensifying vulnerability to complications of COVID-19. In this context, it is also worth highlighting evidence inferring the misconception of claiming that low-income countries may be more immune to (or will be somewhat less affected by) the COVID-19 [72]. By excluding the theory of better immunity in developing countries, the analysis of this study elicits pertinent rationale for considering the interactions between the socioeconomic determinants and both the fatality and recovery rates.
A study has proposed that BCG childhood vaccination could partially explain the reduced morbidity and mortality of COVID-19 in some countries [73, 74], as it could decrease childhood mortality due to a decrease in sepsis and respiratory infections [75]. Several mechanisms have been proposed, including that BCG might cause long-term activation of innate immune cells [76]. The investigators reported that countries that do not have a policy of universal BCG vaccination (e.g., Italy and the USA) were more severely affected by COVID-19 than countries with universal and long-standing BCG policies (e.g., South Korea and Japan) [73]. However, this evidence is still not concrete, and more data are needed. Previous studies have revealed that the effects of BCG on monocytes last only for several months [77], questioning the duration of the immunity following BCG vaccination. Several studies are currently ongoing to determine the effect of BCG vaccination on COVID-19 outcome.
Another factor proposed by several publications was the air quality index, which correlated to the number of cases and deaths from COVID-19 [19–22]. These studies concluded that a small increase in long-term average exposure to fine particulate matter leads to a substantial increase in the spread and mortality rate of COVID-19.
The possibility that our results may reflect differences in the timing and nature of the country’s response (such as testing, case-tracking, isolation, and social distancing measures) to the COVID-19 outbreak cannot be ruled out [32]. It is also possible that countries with a lower HDI are at an earlier stage of the pandemic compared to high HDI countries. However, this explanation is unlikely as the disease has been around for three months, and it seems to have spread to almost every country in the world at this point [54]. Moreover, the lower HDI countries are expected to be less successful in the containment of the contagion [54].
Finally, the difference in mortality between the higher HDI countries and the lower HDI countries may be related to the adequacy of measurement and reporting of cases. A systematic review of studies that assessed the reliability of hospital data on the cause of death revealed that most of the selected studies reported a substantial misdiagnosis of causes of death in hospitals.[77] Additionally, current evidence indicates that COVID-19 deaths are being misattributed to other causes of death, particularly when death occurs at home [78]. According to a recent estimate, the death toll from COVID-19 in selected 14 countries may be 60%higher than reported in official counts [79]. The accuracy of official death statistics related to COVDI-19 is limited by how efficiently a country is testing people to confirm cases. It possible that countries with a lower HDI are not reporting the exact cause of death due to limited resources to diagnosed COVID-19 infection. For example, in Ecuador’s Guayas province, the reported official COVID-19 related deaths between 1 March and 15 April were 245; however, data on total deaths during the same period showed an increase of 350%[79].
Our study has two main limitations. First, our analyses were based on the first few months of the pandemic, and this needs to be revisited regularly throughout the pandemic phases. Second, as with all cross-country analyses, the potential exists for spurious statistical association produced by unmeasured and unknown confounding factors in the form of ecological fallacy [80–82]. Consequently, the associations observed at the country level may not reflect individual-level associations [83, 84]. The best guide we will have for the effects of pandemics on recovery and mortality rates of a future coronavirus are the studies of the previous epidemics. Therefore, in this preliminary ecological analysis, our attention is turned to the role of socioeconomic determinants in the pandemic COVID-19 recovery and mortality rates.
Unlike other studies that addressed the association of COVID-19 detection with individual social or economic variables, our study examined the association of COVID-19 outcomes with a valid and reliable composite of socioeconomic factors. It provided useful insight into explaining between-country variation in COVID-19 outcomes. To the best of our knowledge, our study is the first study to address the association of HDI and COVID-19 outcomes. Furthermore, the validity of the ecologic-effect estimate was enhanced by controlling for the available known confounders (gender and age). Further work is needed to fully understand the mechanisms by which HDI may have affected COVID-19 recovery and mortality rates.
In conclusion, the HDI is associated with the recovery rate, which is perhaps reflective of the levels of preparedness for pandemics. The positive association between the HDI and mortality rates may point to vulnerabilities in approaches to tackle health crises; this should be further investigated. Further research, using data from various phases of the pandemic and various strategies used including vaccination is need.
Footnotes
Acknowledgments
The authors have no acknowledgments. There is no funding for this study.
Author contributions
CONCEPTION: Haitham Jahrami and Amer AlDerazi
METHODOLOGY: Haitham Jahrami and Nicola Luigi Bragazzi
DATA COLLECTION: Haitham Jahrami, Amer AlDerazi and Nicola Luigi Bragazzi
INTERPRETATION OR ANALYSIS OF DATA: Haitham Jahrami, Ahmed S. BaHammam and Randah R. Hamadeh
PREPARATION OF THE MANUSCRIPT: Haitham Jahrami, Amer AlDerazi, Ahmed S. BaHammam, Randah R. Hamadeh and Mohamed Buheji
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Mohamed Buheji, Dunya, Ahmed and Ahmed Ebrahim
SUPERVISION: Mohamed Buheji and Haitham Jahrami
Conflict of interest
All authors have no conflict of interest to declare.
Ethical considerations
This is an ecologic study of online available data. Therefore, ethical approval was waived.