
Abstract
BACKGROUND:
Monitoring replanted digits remains a challenging task in microsurgical units. Previous studies have indicated the perfusion index (PI), a parameter directly proportional to the blood flow, might be a useful tool.
OBJECTIVE:
The PI is evaluated as a monitoring tool in patients with replanted digits.
METHODS:
This prospective, non-interventional study includes 31 patients with revascularized or replanted digits. After successful revascularization or replantation, the PI and peripheral oxygen saturation of the affected finger and its contralateral equivalent were measured simultaneously. The values were detected by the device Radical-97® Pulse CO-Oximeter® (Masimo Corporation, 52 Discovery, Irvine, CA 92618, USA).
RESULTS:
The median PI of affected fingers was 3.5±0.56 for revascularized and 2.2±0.8 for replanted fingers. The difference between the PI values of replanted digits and the healthy contralateral side was highly significant (p < 0.0001). The area under the curve in the receiver operating characteristics was 0.92 for a PI difference > 80.49% and predicted a loss of replant with a specificity of 100% and a sensitivity of 75%.
CONCLUSION:
The assessment of the PI in patients with reperfusion of a vascular compromised digit is a useful tool to continuously monitor peripheral perfusion. The dynamic behavior of the PI is essential to detect perfusion disturbance.
Introduction
Despite technical improvements such as suture material and microscopic developments (resolution, 3D, integrated fluorescence angiography) the replantation of digits and toes remains a challenging topic in microsurgical units [1]. In contrast to free flap surgery, postoperative management is still mostly performed by clinical evaluation of color, capillary refill, turgor, and temperature. Most technical devices are non-suitable due to the small vessel size of digital arteries. Fluorescence angiography, capillary microscopy or laser Doppler flowmetry offer a quite reliable perfusion visualization but the devices are cost- intensive and not very handy in clinical everyday routine [2–6].
Back in the 80s, continuous monitoring of peripheral oxygen saturation (SpO2) was used to monitor replanted digits [7]. This method was discarded during the following decades due to difficulties with sensors and the fact that the measured value depends on too many influencing factors. With the new SET-technology and the resulting more reliable measurements the monitoring with pulse oximeters has once again entered the stage. In most modern pulse oximeters, the perfusion index (PI) is calculated by using the photoelectric plethysmography function. PI is defined as the ratio of the pulsatile (arterial component) and the non-pulsatile (other tissues) components of the infrared light arriving at the receiver [8]. Pulsation of arterial blood causes a change in pulsatile volume while the non-pulsatile component remains constant. That way, volume changes in the vascular system are detected, which correspond to the perfusion. The infrared light signal is primarily influenced by blood flow and not by the arterial oxyhemoglobin levels of the blood at the sensor site and is thus calculated independently of oxygen saturation.
A previous study showed that monitoring free flaps and replanted digits via PI is easily possible [9]. The PI values in healthy adults between the digits of different hands revealed an almost identical dynamic which enables the method to detect perfusion disturbances in revascularized and replant digits [10].
We want to verify whether the PI values of revascularized and replanted digits differ from the perfusion in a healthy hand. This difference could be used to predict the outcome of replanted digits in the future. We plan to include all patients with injuries of digital blood vessels and successful anastomosis as they represent the “ideal replants”.
Materials and methods
This prospective study was approved by the local ethics committee of the University Hospital Regensburg (registry: Ethics committee University of Regensburg, registration number: 19-1419-101, date of registration: 05.06.2019, principal investigator: Dr. J. Hahn). The study was registered at the center for clinical studies at the University of Regensburg (registration number Z-2020-1373-0). The registration of the clinical trial occurred prior to the start of the trial and the manuscript adheres to the applicable CONSORT guidelines. The first patient was enrolled in March 2020 and the last patient was enrolled in April 2021.
Within the first 72 hours after surgery, we included all consentable patients > 18 years with successfully revascularized or replanted digits. The successfully revascularization of digital blood vessels was intraoperatively confirmed by a positive patency test. All participants received a participant’s briefing and written informed consent was obtained from all subjects. Patients with immediate visible postoperative vascular impairments were excluded to avoid further pressure or traction damage to the small vessels.
Microcirculation was detected by the device Rad-97™ Pulse CO-Oximeter® from Masimo (Masimo Corporation, 52 Discovery, Irvine, CA 92618, USA), which uses the Signal Extraction Technology (SET) and Signal Identification and Quality (Signal IQ) Technology [11, 12]. The device measures perfusion index, oxygen saturation, and pulse rate every 2 seconds. In addition, special types of finger pulse sensors (RD SET Neo Adhesive Sensor, Masimo Corporation, 52 Discovery, Irvine, CA 92618, USA) were used. The sensor was chosen due to small vessel sizes and highly vulnerable tissue with a perfusion being extremely prone to external compression or shear forces after a replantation. Therefore, it is of particular importance to use sensors that have very low dead weight and measure the diminutive size of the vessels adequately. This sensor is stabilized by a self-adhesive tape and are therefore less exposed to the risk of dislocation due to movement or additional bandages. The affected digit(s) and its contralateral equivalent(s) were simultaneously measured.
Measurements
During the measurements, patients were in a resting, lying position. Both forearms were placed in front of the body at heart level. All measurements were performed by the same investigator and under consistent external conditions. Measurements were interrupted for change of dressings, personal hygiene procedures or food intake.
Statistical analysis
The Masimo Instrument Configuration Tool was used to transfer the recorded data from the Masimo device to a PC. Microsoft Excel for Office 365 (Microsoft, Redmond, WA, USA) was used to convert the native data into a statistically evaluable data set. Analysis was performed using MedCalc statistical software version 22.013 (MedCalc Software Ltd, Ostend, Belgium, 2023). Results are expressed as median/ mean ∓ standard deviation (SD) or median/mean ∓ 95% confidence interval (95% CI). A paired t-test was used to calculate the differences between the affected digit and the healthy contralateral.
A p value < 0.05 was considered statistically significant.
Results
We included 17 patients with 20 replanted digits and 14 patients with revascularized digits (patients are also referred to as IDs). Most of the patients were male and had a median age of 43±17.3 in the replant-group and median age of 44±18.45 in revascularization-group. In most cases patients were right-handed and injured their adominant left hand. An overview of patient characteristics is given in the attachment (see Table 1). Median observation time was 36.25±31.01h for replanted digits and 17.5±7.54 h for revascularized digits.
Patient characteristics
Patient characteristics
Revascularized digits showed a median PI of 3.5±0.56 while the contralateral healthy equivalent showed a median PI of 3.9±0.46 (see Fig. 1 and Table 2). In comparison, the PI values showed a significant difference (p = 0.049).
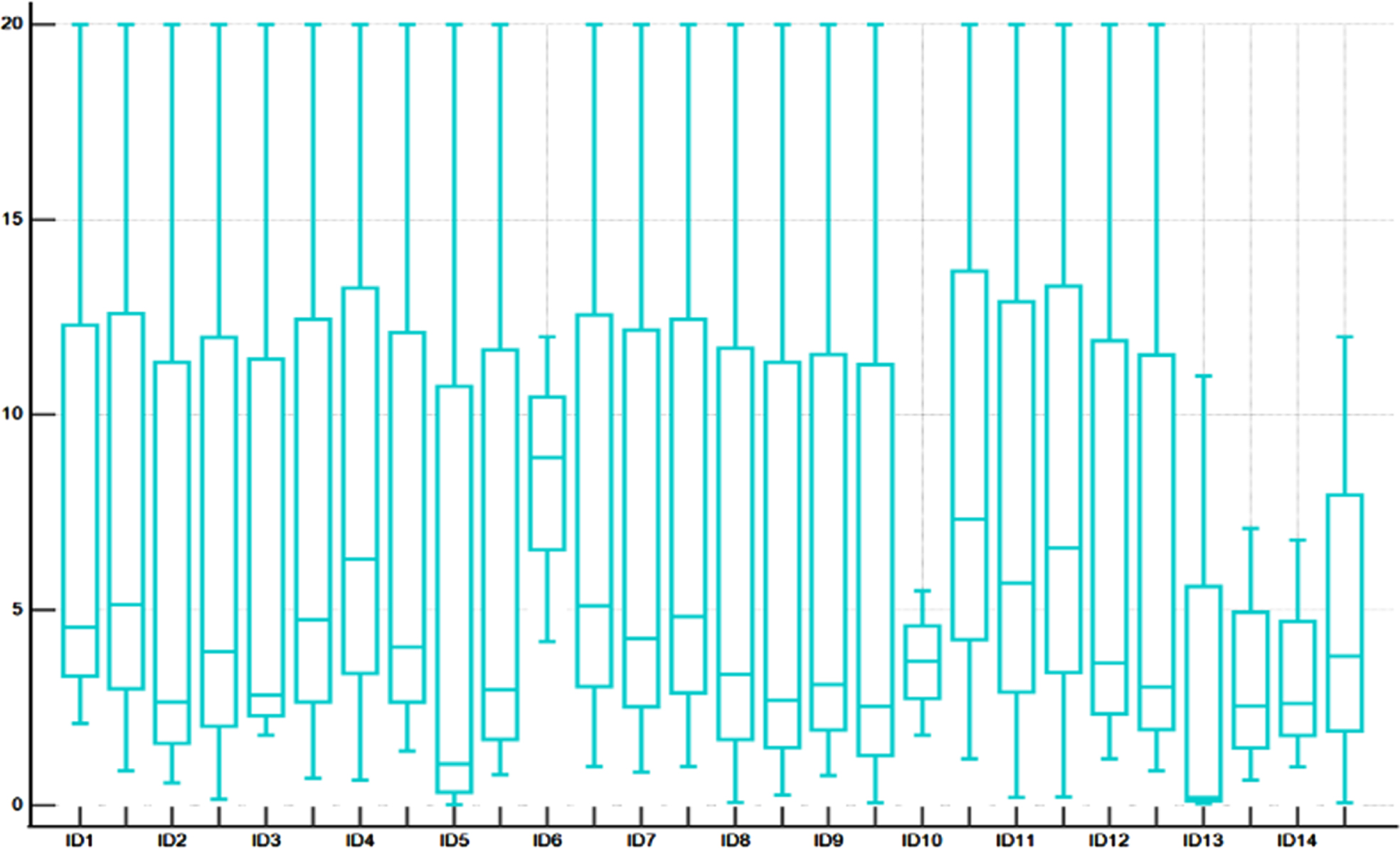
Distribution of PI values in each patient (ID), left boxplot represents the affected finger and right one the healthy equivalent.
PI Values of revasularized digits
Replanted digits had a median PI of 2.2±0.8. The contralateral equivalent showed a median of 4.70±0.61 (see Fig. 2 & Table 3). The differences between the affected side and the healthy contralateral were highly statistically significant (p < 0.001).
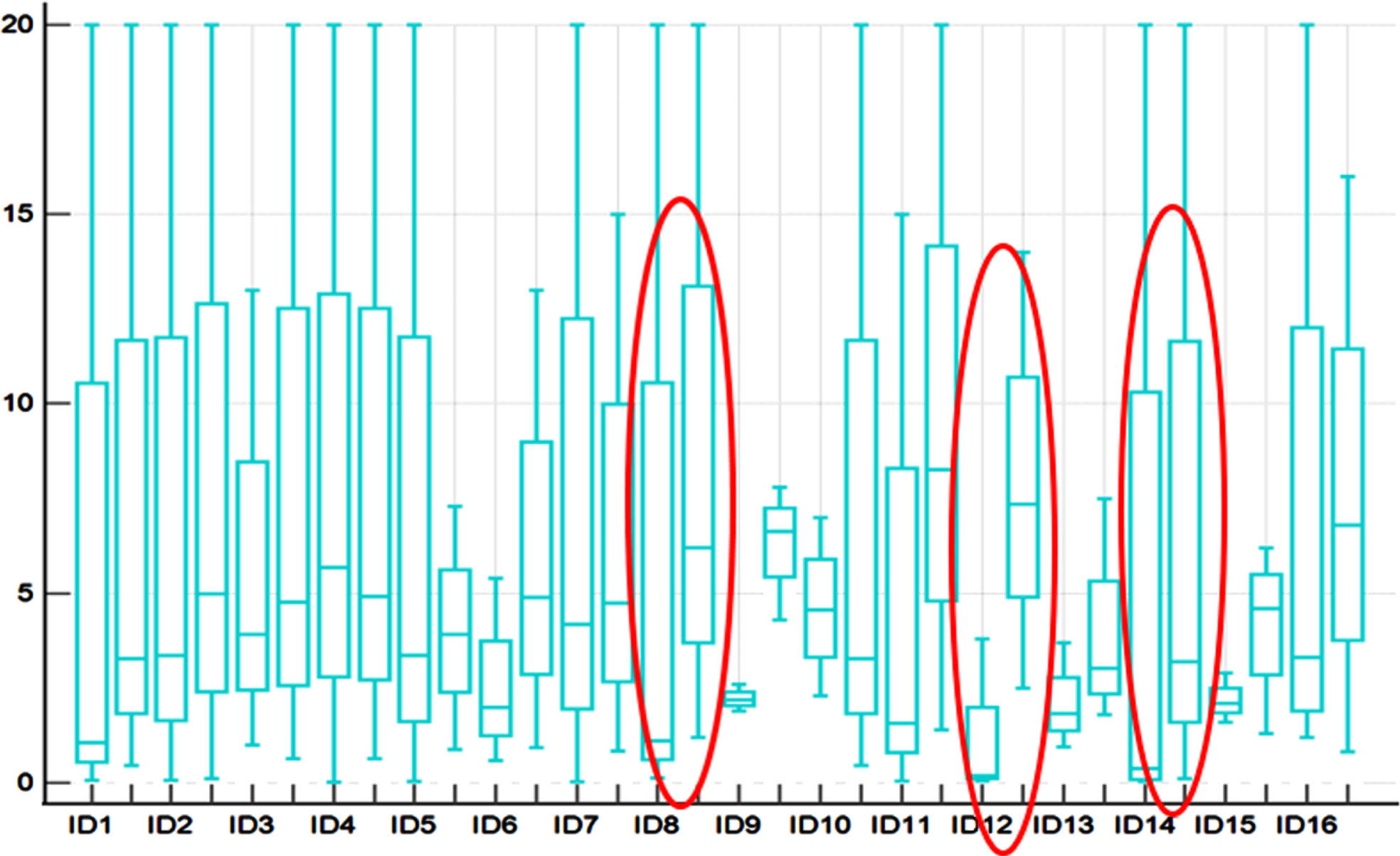
Distribution of PI values in each patient (ID), left boxplot represents the affected finger and right one the healthy equivalent. Non-successful replants are marked in red.
PI values of replanted digits
The median PI value of successfully replanted digits was 3.04 and very close to the PI values of revascularized digits with a median of 3.5. This difference was not statistically significant (p = 0.33) as “ideal replants” seem to match the perfusion profile of revascularized digits. Revascularized digits show an impairment in perfusion due to the injury of the blood vessel and probably also because of the damage to the surrounding tissue.
Partial necrosis and loss of replants
During postoperative follow-up, six patients with replanted digits presented with clinical signs of perfusion impairment and/or change in PI dynamics. One of the patients had a successfully revision surgery (ID 15). The other five patients developed a partial or full necrosis of the replanted digits and had to undergo secondary amputation or debridement. A revision surgery to address the vascular anastomosis was not an option for these patients because a lack of usable veins had already become apparent during the first surgery.
Tables 4 and 5 show the distribution of PI values the successful and non-successful replants.
PI in successful replants
PI in successful replants
PI in non-successful replants
In three of these patients the measurements were difficult from the beginning due to venous bleeding from the fenestrated nail. Therefore, the monitoring was only possible for a short duration of time (mean 26.33 h with a median of 1.8 h). During follow-up these patients showed a delayed partial necrosis of the replanted tissue and had to undergo a secondary debridement. The replantation itself was successful.
ID 10 presented with continuously dropping PI-values (see Fig. 3). This replant also showed clinical signs of rapid deteriorating, so the monitoring was stopped, and the patient hat a secondary amputation the next day.
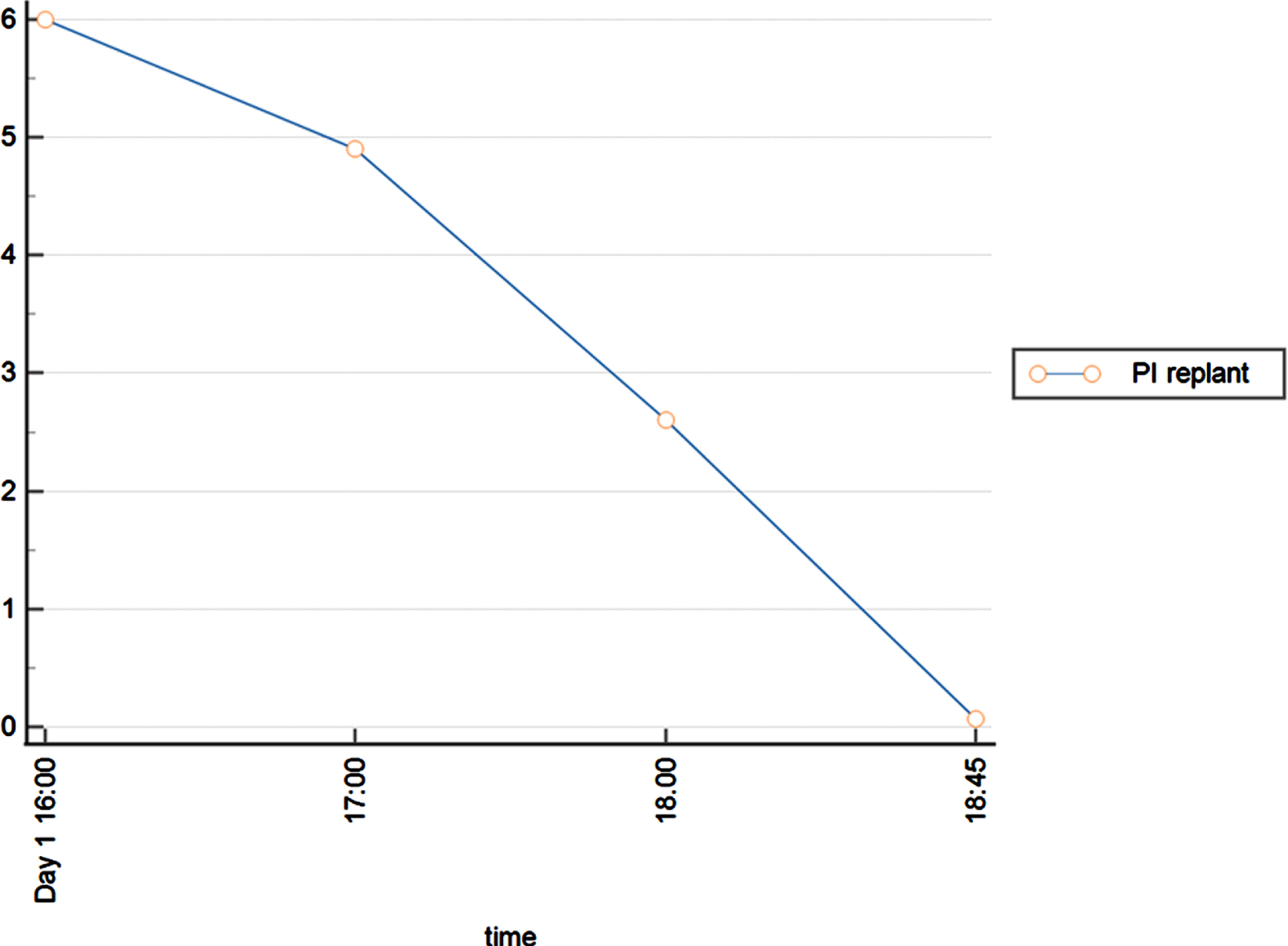
course of PI values in ID 10.
During observation ID 5 showed a drop in PI values at Day 2 (see Fig. 4). Afterwards the PI values stabilized for some hours before values started dropping again. The measurement was stopped as clinical signs of vascular impairment presented and the patient expressed the wish to drop out of the study. We assume that the initial drop was due to a venous thrombosis followed by an increased arterial input in an unsuccessful attempt to restitute perfusion.

course of PI values in ID 5.
Failed replants showed a median PI of 0.19. The difference between PI values of successful versus failed replants was highly statistically significant (p = 0.0056).
Therefore, we performed a receiver operating characteristics (ROC) analysis to see if this difference could be used to predict the outcome of the replanted digit. The analysis showed an area under the curve (AUC) of 0.92 for a difference of > 80.49% (see Fig. 5). There was a highly significant correlation for the percentual difference > 80.49% and a complete loss of replant in follow-up (p < 0.001). Sensitivity was 0.75 (95% CI 19.4-99.4), specificity 1.0 (95% CI 79.4-100).
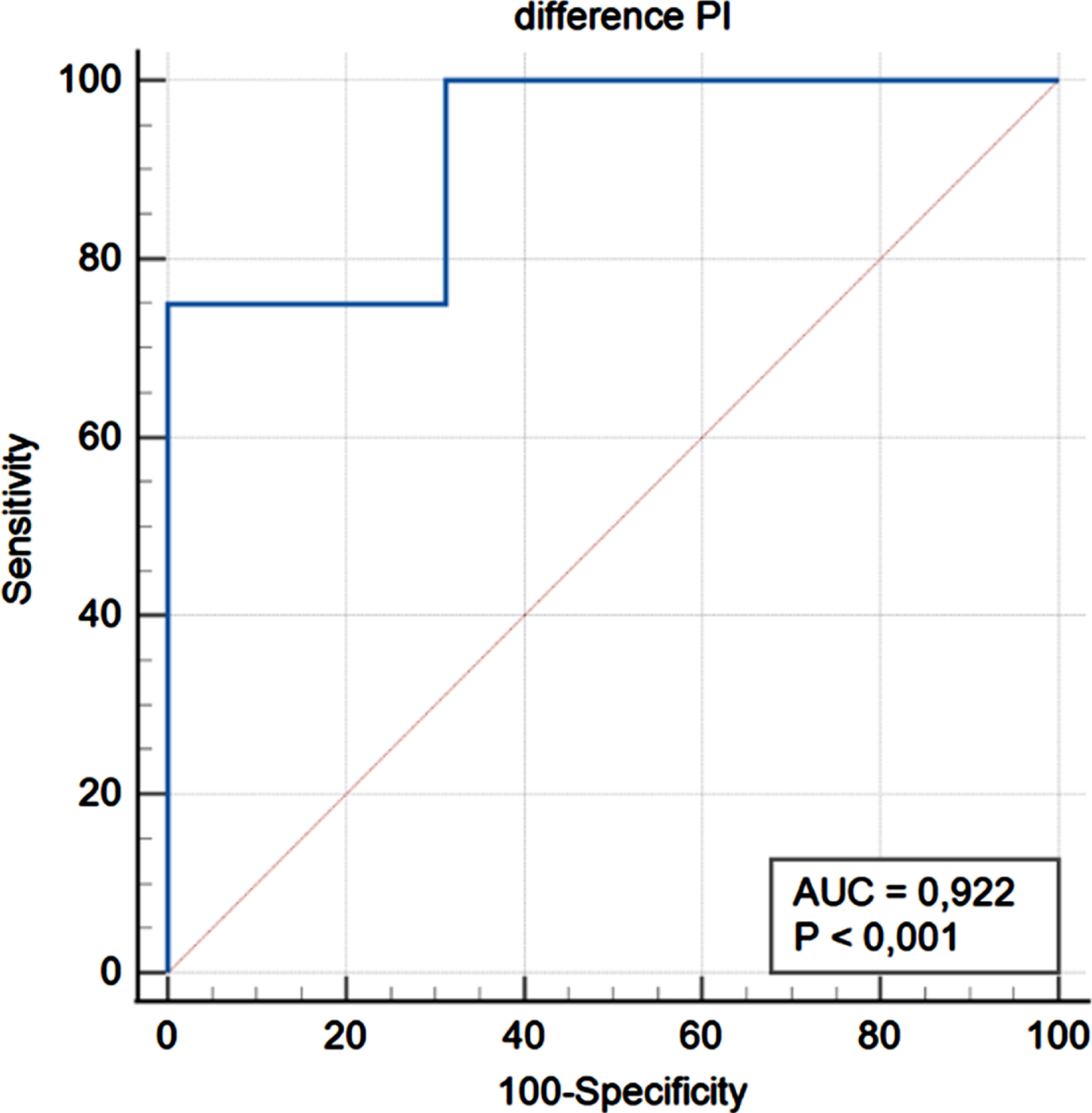
ROC analysis for PI differences > 80.49%.
When the PI cutoff values for loss of replant were calculated from the ROC curves, the cutoff was found to be 2.1 (AUC = 0.93, p < 0,001) with a sensitivity of 1.0 and a specificity of 0.75 (see Fig. 6).
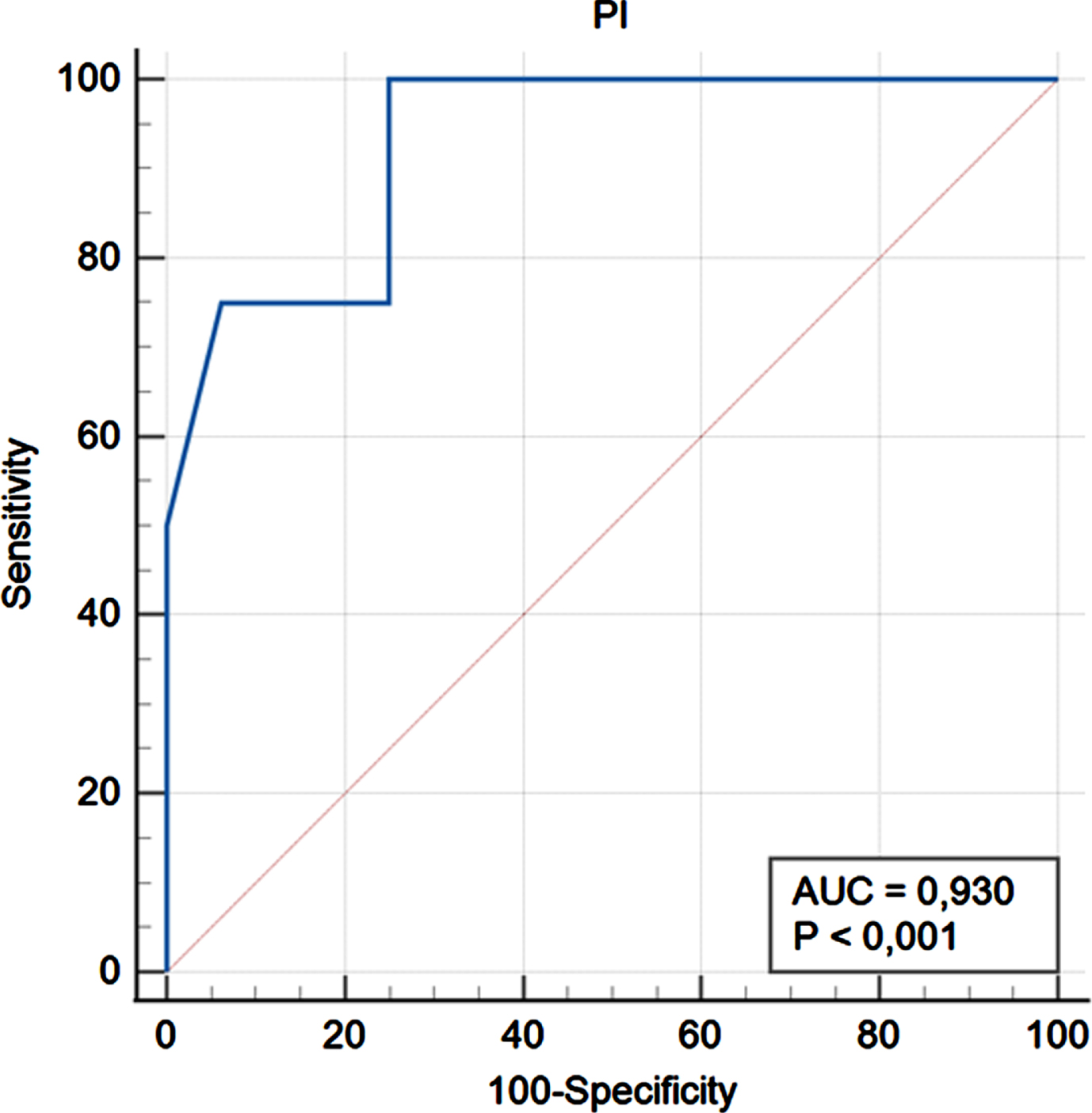
ROC analysis for PI values.
This study shows that PI measurements are a reliable monitoring tool for replanted digits. There is a significant difference in PI values of successfully and non-successfully replanted digits. The PI drops earlier than clinical evaluation shows any irregularities (see Fig. 4, ID 5). This offers the chance for an earlier decision for revision surgery (if possible and reasonable). Current studies show that early detection of vascular disturbances is crucial for the survival of the replant [1, 13].
The meaning of bilateral measurement is undeniable as interindividual PI values show a remarkable range. Different studies confirmed the skewed range of PI values between 0.34–11 in sitting objects [8, 10]. Changing position significantly influences the variation of PI values as Tapar et al showed [14]. While in a 45-degree back-up sitting position patients showed PI values with a mean of 4.5±2.5 which is comparable to our measurements (median of 4.65±0,63 in the non-affected equivalent of replant patients respectively 3.9±0.46 for the non-affected equivalent in revascularized digits).
In a baseline study at our institution in 2022, we demonstrated the close relation between the dynamic behavior in PI values of both hands in healthy adults. This almost identical pattern of both hands was the basic condition for monitoring replants [10].
There is also a significant difference between revascularized and healthy tissue as our monitoring data from reconstructed neurovascular bundles in digits show. Revascularized digits show an impairment in perfusion due to the injury of the blood vessel and probably also because of the surrounding tissue. Their PI values can be seen as the “ideal” PI values for successful replantation.
If the values of the critical perfused and later amputated replants (ID 8,12,14) are taken out of the invoice the PI values of successfully replanted digits are very close to these of revascularized digits (median 2.6 to median 3.5, percentage difference 26%). There is no statistically significant difference between these two groups (p = 0.33).
There have been several studies that linked low PI values with critically ill patients in intensive care units. Lima et al found a cutoff peripheral PI value of 1.4 correlated with the presence of diminished peripheral perfusion [8]. In a prospective, observational study, He et al detected the PI as an independent marker for the 30-day mortality in patients from intensive care units [15]. Their ROC analysis showed a cut-off for PI < 0.6.
A Swedish multi-center-study linked PI < 0.70 to low perfusion due to severe critical illness in neonates and emphasized its use as a screening tool for left heart obstructive disease in newborns [16].
We also observed rather low PI values in non-successful replants (median 0.19). The values of successfully and non- successfully replants differed significantly (p = 0.0056) (see table 4&5). The ROC analysis showed a cut-off for PI values < 2.1 linked to a loss of replant (AUC 0.93 (95% CI 0.723-0.996), p < 0.0001.). As there were only three losses of replant in our study, this value has yet to be confirmed in a study with a larger number of patients.
Another ROC analysis was performed to see if the difference between replant and contralateral healthy equivalent could be used to predict the outcome of the replanted digit. Analysis showed an area under the curve (AUC) of 0.92 for a difference > 80.49%. Sensitivity was 0.75 and specificity 1 (see Fig. 5).
Both ROC analysis combined (difference in PI values > 80.49 and PI < 2.1) can be used to advise patients about the potential outcome. Eventually it may spare patients a wait of days or even weeks before clinical demarcation of the replant shows and secondary amputation can be performed.
Compliance
Compliance was a big issue during the monitoring period as seven patients asked for an early drop-out. Due to the monitoring setting with both upper extremities connected to monitoring devices, patients had to be completely immobilized. This was usually not an issue during the first 48 hours as patients were still recovering from surgery and extremely motivated to support any action in potential favor for the replantation. Of course, patients were disconnected for measures e.g., changing of dressings, personal hygiene or food intake. After 48 hours the compliance usually dropped dramatically. A wireless observation might be a good option during the period of reduced bed rest and after clinical stabilization, intermitted observation (e.g., three times a day) should be considered.
Application and handling
At first glance, the application and handling of the measuring devices appears to be rather simple. However, application can be tricky in cases of venous bleeding due to nail fenestration or leash therapy. In these cases (n = 4) we used intermittent measurements immediately after changing of dressings. Nevertheless, handling and interpretation is much easier than in most monitoring devices such as fluorescence angiography, implantable venous flow coupler or contrast enhanced ultrasound [2, 18]. In addition, most monitoring procedures for free flaps are not applicable to replanted fingers due to the small vessel size of digits.
Limitations
PI values are detected every 2 seconds and very sensitive to changes in body environment (e.g. temperature, change of dressings) and body posture. This makes it crucial to measure the opposite side simultaneously to better assess the significance of the change. However, measurement of both sides is associated with a major limitation in patient comfort and significantly limits compliance. Therefore, the PI measurements might be more useful in patients with limited or critical reperfusion of replants and just in the first 48 to 72h after replantation.
Observation time in our study showed a great range (replants 36.25±31.01h) which was mainly caused by sensor application difficulties.
Conclusion
This study shows that the PI can be used to monitor replanted digits. It is crucial to monitor the affected digit as well as its healthy contralateral equivalent. Monitoring should be limited to the first 48- 72 hours to support the patient’s compliance.
Financial disclosures
None.
Conflicts of interest
Catharina Strauss (M.D.) and Sebastian Geis (M.D) received technical devices for this study from Masimo. There has been no role of Masimo in this study. All other authors have no conflict of interest.