
Abstract
BACKGROUND:
Complex injuries of the hand frequently result in loss of essential functional features. Common reconstructive procedures for soft tissue defects of the thumb or phalanges are locoregional flaps like Moberg-, Foucher-, Cross-Finger- or Littler flaps. Microneurovascular toe (joint-) transfers complete the arsenal of operative reconstructive procedures and allow for most detailed reconstructions. Our experiences with free toe transplants are reported and diversely discussed regarding contending procedures.
METHODS:
From 2010 until 2019 14 patients who received emergency or elective partial or complete toe transfers were compared with a control group (n = 12) treated with contending reconstructive procedures. Aim of the reconstructions was to cover the defect with well-vascularized, sensate tissue, while preserving length and range of motion in a reliable manner.
RESULTS:
The Kapandji score showed a significant difference (p- value = 0.04) with a score of 9.8 in comparison to control group (Kapandji index = 8.0).
CONCLUSION:
In our heterogenic patient collective free toe transplants have proven to achieve comparable functional results for reconstruction of two and tripartite phalanxes as opposed to common local reconstructive procedures.
Keywords
Abbreviations
Interphalangeal joint (thumb)
Distal interphalangeal joint
Proximal interphalangeal joint
Metacarpophalangeal joints
Two point- discrimination
Total active range of motion
Postoperative day
Introduction
Amputations of two or tripartite phalanges of the hand are a frequent phenomenon caused through private or work-related accidents. The hands represent an important and complex functional-anatomic part of the human musculoskeletal system. Loss of motor and tactile properties represent severe injuries which often result in loss of previous working capacity. Without adequate reconstruction functional and aesthetic impairments are inevitable. The organ of the hand is highly visible and its integrity contributes significantly to self-esteem and body image [1, 2].
The indication for replantation is dependent on the mechanism of injury, as a main predictor for successful replantation [3], and further includes affected finger rays, patient’s compliance and expectations as well as comorbidities [4, 5]. In accordance with Sir Harold Gillies’s well-known dictum “losses must be replaced in kind”[6] replantation of the thumb should be indicated whenever possible.
Per definition, so-called absolute indications for replantation comprise the thumb, multiple fingers, transmetacarpal or hand, and any upper extremity amputation in a child whatever level [7]. Fingertip amputations distal to the insertion of the Flexor digitorum superficialis (FDS) are also a good indication [8]. Injuries of the dominant hand are generally treated more consequently [9].
Other cases are more controversial because of poor functional outcome, especially for the index finger, which subsequently may often be functionally excluded. If revascularization fails or there are contraindications to primary replantation, a need for secondary reconstruction or replacement of the lost parts of the digit may arise. Today, the major concern is not “how to replant an amputated part”, but rather “how to make it functional” [10] In this regard, replantation without sensation and function is no longer considered acceptable.
Several options are available, ranging from no reconstruction, to non-microsurgical reconstruction [11], phalangisation [12], to partial or total microsurgical toe transplant to the hand. Reconstructive criteria of parts of the tripartite phalanges are different in comparison to the thumb. An ideal thumb reconstruction should create a digit that is similar in appearance and length to the contralateral thumb, is sensate and functional (pinch and grip), and is associated with minimal donor site morbidity [13–15]. The nail should be preserved or transplanted for an exact pinch [16]. Common parameters for decision- making of surgical procedures are amputation level and soft tissue compromise, age and profession, but furthermore patients’ preference, national culture, health care system and expertise of the treating surgeon [17].
Fingertip amputation is a common injury around the world. The treatment for this injury is controversial. Many techniques have been described, including occlusive dressing, simple revision amputation, skin grafting, local flaps like Epping flap oder Foucher flap [18, 19], island flaps (Venkataswami flap) [20], distant flaps, and free tissue transfer. Ideally, decision-making about what surgical technique to select should be based on a classification system as described by Merle et al. (Fig. 1) integrating functional and aesthetic aspects [21]. Succeeding non- vascularized joint transfer as published by Lexer as early as 1908, vascularised toe joint transfer is a well describe method, especially for replacing the PIP- joint (PIPJ) of the tripartite fingers in association with composite tissue defects [22]. The advantages of lower risks associated with complete free toe transfers compared to prosthetic joint implants faces the sub- optimal range of motion and the extension lag resulting from the poorly developed extensor tendon mechanism in the toe. Several surgical modifications were tested to improve finger’s extension and the total range of motion [23, 24].
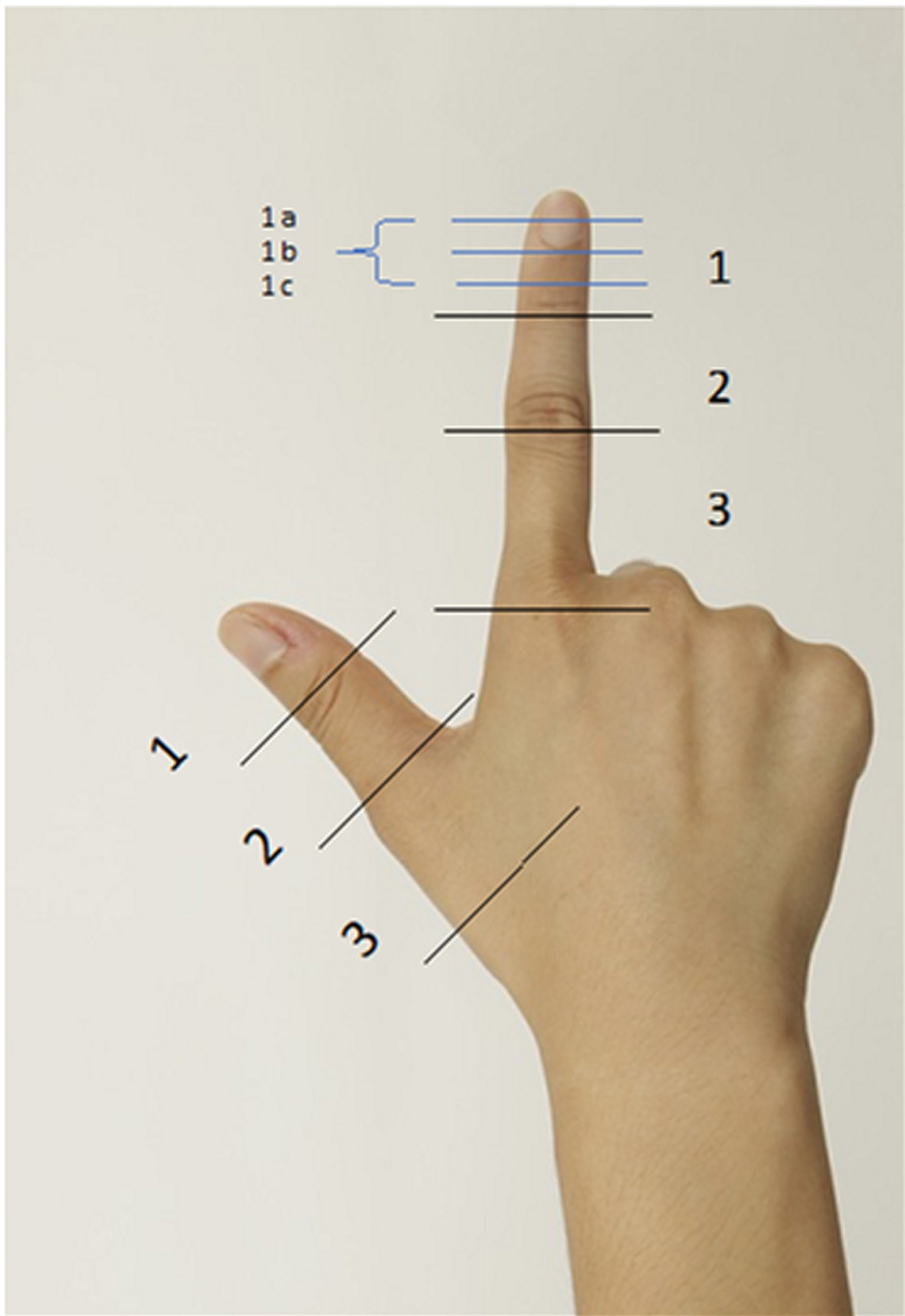
Merle’s classification of the amputation level (of the thumb and tripartite fingers). (Level 1 = amputation distal to IPJ/DIPJ (1 a = onliy pulp defect; 1 b = mid portion of distal phalanx (osteocutaneous defect); 1 c = base of distal phalanx). Level 2 = amputation distal to the PIPJ (tripartite fingers)/amputation at base of proximal phalanx or through MPJ (thumb). Level 3 = amputation distal to MPJ (tripartite fingers)/amputation at base of first metacarpal bone or through CMCJ).
This retrospective study was designed to evaluate potential benefits as well as disadvantages of free vascularized autologous (partial) toe transplants in contrast to a control group of alternative reconstructive options. End points were functional aspects as range of motion, sensation and postoperative complications. Goal was to achieve best possible outcomes. Selected benefits of partial or total toe to hand transfers at different amputation levels for all parts of the finger preserving best possible function and aesthetic outcome of the hand in comparison to common reconstructive methods are discussed.
From 2010 to 2019 all patients at the Department of Plastic, Hand, and Reconstructive Surgery receiving either free vascularized partial or total toe transfers (group I) (Table 1–3) or alternative reconstructions (group II) (Table 4-5) as local or island flaps like Foucher-, Epping-, Littler-, free venous flow- through flaps or joint arthroplasty were included into this retrospective study. This study was approved by the Institutional Review Board Committee of the University of Regensburg (no. 20-1845-104) and was designed in accordance with the Helsinki Declaration. Informed consent was obtained of all patients prior to the free flap procedure or alternative operation respectively. Patient consents included photographic material. The level of amputation was defined by the classification of Merle [10] (Fig. 1). Primary/delayed primary reconstructions were defined as operations the day of trauma to one month after. Secondary operations were defined as any reconstructions after this time period.
Survey of patients and the microsurgical reconstructive procedures of tripartite phalanxes in Regensburg (2010–2019)
Survey of patients and the microsurgical reconstructive procedures of tripartite phalanxes in Regensburg (2010–2019)
Survey of patients and the microsurgical reconstructive procedures of the thumb in Regensburg (2010–2019)
Sensory recovery (dynamic 2 PD) and range of motion (ROM) after partial or total toe to hand reconstruction at different levels after 12 months
Survey of patients in control group and the reconstructive procedures of the thumb in Regensburg (2010–2019) after > 6 Months
Survey of patients in control group and the microsurgical reconstructive procedures of
A two-point discriminator (2PD) (Cando 12-1480 Two Point Aesthesiometer; Baseline) with nonadjustable points was used for testing the sensation of each digital nerve. The exact measurable distance can be read on the instrument (range 2 mm to 20 mm). Measuring of the two-point discrimination is described as a viable tool in literature (Karjalainen et al., 2019; van Nes et al., 2008). The range of motion in tripartite fingers after joint replacement was measured with universal goniometer (standard finger and wrist goniometer; (Patterson Medical, Warrenville, IL) with full-circle body, the measured excursion was extension und flexion in all three joints of the finger. For tripartite fingers the active range of motion (TARM) was measured by summation of full extension and flexion of each joint of the finger. Especially for the reconstructed thumb Kapandji score (maximum score 10) was measured beside TARM for ip- joint (IPJ) and mcp- joint (MCPJ). The Kapandji score is used to test thumb opposition and the counter-opposition (reposition) using the hand itself as a reference [25]. This test is valid only if the first stages are possible.
Wound healing disorders, skin necrosis or haematoma being treated conservatively were classified as minor complications. Major complications were defined as loss of the graft, venous stasis or arterial occlusion needing surgical intervention. Statistical analysis was performed with SPSS (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.).
The unpaired students t-test was used to test for statistically significant differences (p < 0.05).
Results
Group I: free vascularized partial/total toe flaps (n = 14) (Table 4)
In total, 14 operations were performed as primary/delayed primary within 14 days (n = 3) or secondary reconstructions (n = 11). The point of time between injury and secondary reconstruction was 3.36±4.01 months (n = 14; range 0 to 12 months). Included procedures were pulp free flaps of the 2nd toe (n = 4), the modified wrap around toe pulp flap (n = 1) or the trimmed great toe flap of the great toe (n = 2), joint transfers (PIPJ)/(MCPJ) of the 2nd toe (n = 5) or total second toe transfer (at the base of phalanx) (n = 2). Patients comprised 13 males and 1 female with age of 35.85±17.19 years (n = 14; range 16–81 years).
As minor complications wound healing disorders (n = 4) at donor side were seen. A post-traumatic depressive disorder by one patient (no. 9) (Table 3) significantly impaired training therapy and delayed secondary tenolysis. The hospitalization time for free vascularized partial/total toe flaps were 13.14±6.19 days (n = 14; range: 8–24 days). The oldest patient was lost to follow up due to an oncological chronic disease (patient no. 14/Table 3).
Patient no. 1 lost pulp of dominant thumb by crush injury (Level 1 a- b). A primary replantation failed, secondary reconstruction was made by pulp free flap of the opposite great toe. Twelve months later, she received as a secondary procedure a split nail transplantation for improving of tweezer handle.
Patient no. 7 lost the pulp of his index finger by accident. Primary replantation failed. The neurovascular pulp of the second toe was transplanted 21 days after trauma. Wound healing was uncomplicated at donor site and index finger (Fig. 2). Sensory recovery (2PD) measured 6 mm after 5 months (Table 3).
Neurovascular free pulp flap of second toe for reconstruction of index finger pulp of pat. no. 7 after avulsion injury. (Up left: avulsions injury index finger. The skin was initially readapted but secondary necrosis up right: donor site second toe; down left: harvested free pulp flap; down right: appearance in follow- up (5 months) with pleasing functional and aesthetic result. The 2PD was measured with 6 mm.).
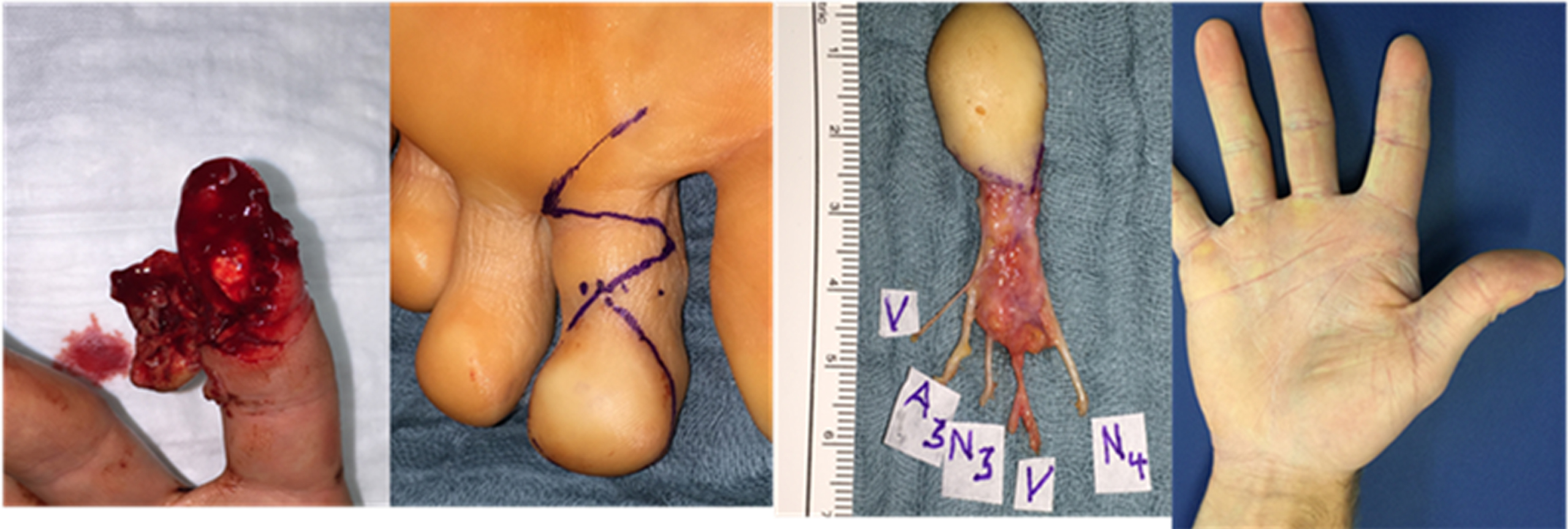
Patient no. 2 lost the 80 % of the pulp of his thumb by a crush injury without an accompanying nail injury. Secondary to a failed replantation a wrap-around flap of the great toe was transplanted to restore length by bony components and the pulp by soft tissue (Fig. 3). The missing length of the thumb measured 2 cm after unsuccessful replantation. After 12 months the length of the reconstructed thumb to uninjured thumb was measured 1 cm at follow up. The flexion of the IPJ was 30 °, Kapandji- Index was 10. The donor site healed on secondary cure after debridement and full skin transplant (Fig. 4) (Table 3).

Pat. no. 2 (Table 3) lost the pulp of the dominant thumb (level 1b) by crush injury and benefited from modified wrap around flap of great toe. (Upper left: necrosis after unsuccessful replantation of amputated pulp; upper second: flap harvesting of a partial osteocutanenous great toe flap with harvesting of metatarsal plantar artery, proper plantar digital nerve II, two concomitant veins; upper third: postoperative x- ray (4 weeks) after k- wire transfixation of osseous part of distal phalanx of great toe; upper right: IPJ flexion is 90 ° in follow up after 12 months. Down: Donor site after modified wrap around flap of the great toe (9 months). The patient did not complain of functional impairments.)

After losing the pulp of dominant thumb by crush injury, a functional defect reconstruction was achieved by a neurovascular wrap around flap taken from the great toe from the left foot (pat. no. 3/Table 3). (Upper left: intraoperative defect (2×3 cm) of thumb and recipient vessels (end to side to radial artery and concomitant veins): upper right: markings for wrap around flap of great toe (including deep peroneal nerve, fibular great toe digital nerve). Down left: follow up thumb function after 18 months with Kapandji score 10/10 and 2PD 8 mm both digital nerves down right: healed donor site after 18 months).
Patient no. 3 lost his right thumb of the dominant hand by crush injury. In emergency a foucher flap for covering of soft tissue was used but failed 72 hours later.
3 weeks later a wrap around flap transplantation from left great toe for customized coverage of the 2×3 cm pulp defect, was performed. At follow up after 12 months no limitation to work requirements in daily life remained (Fig. 4).
After initially showing adequate perfusion one free pulp transplant (Pat. no. 6) after degloving injury of distal digit of the ringfinger, a malperfusion on POD 5 with subsequent complete necrosis of the transferred tissue occurred but was maintained to heal by secondary intention. No further procedures were necessary and the result showed a comparable outcome with the rest of cases.
Patient no. 5 lost his thumb at the base of basis phalanx of the thumb by degloving injury. After frustrate replantation, primary closure was done and followed by secondary reconstruction with total second toe transfer. Both digital nerves, flexor pollicis longus and flexor tendon of the second toe were connected, as well as extensor pollicis longus tendon and extensor tendon of second toe. After one year Kapandji index was 10, everyday activities like opening a bottle or pointed handling were possible (Fig. 5).
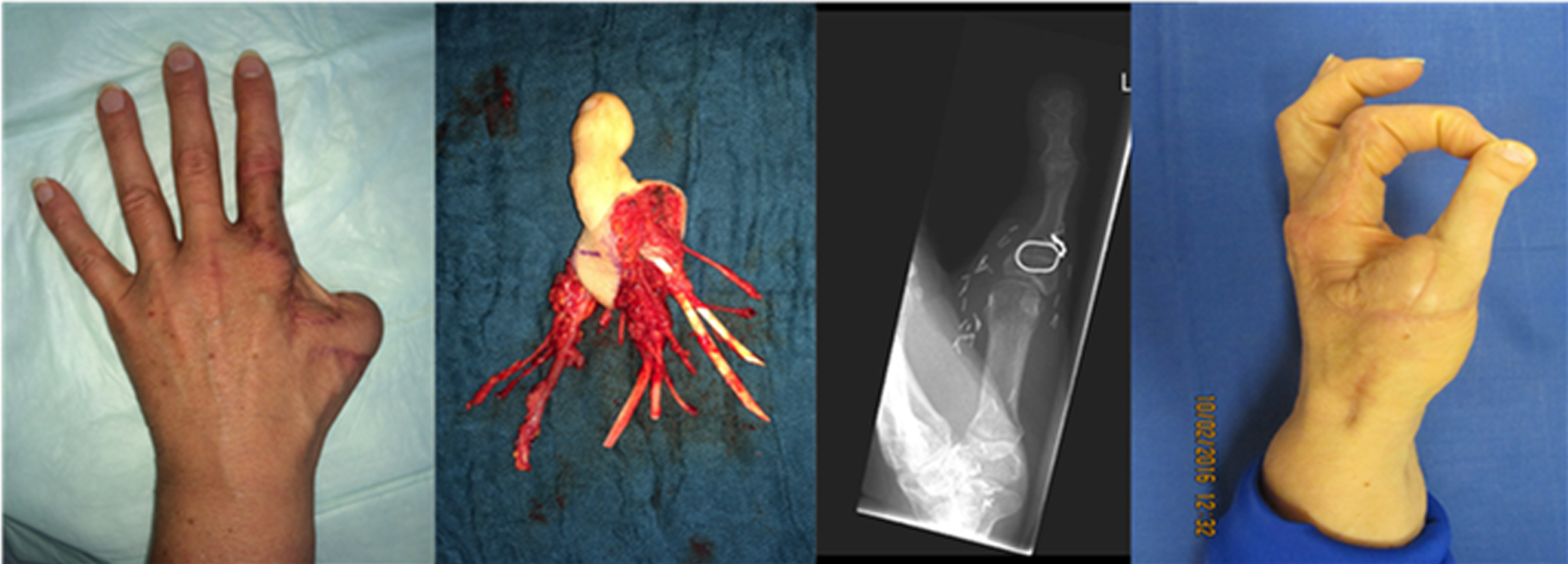
Pat. no. 5 (Table 3) was reconstructed by a total second toe transfer at base of thumb after amputation at level 2b. (Left: intial primary closure with a pedicled modified Foucher-flap; second: free neurovascular toe transplant with metatarsal plantar artery 3/4 to digital artery 1/2, proper plantar digital nerve 3/4 to digital nerve 1/2, two concomitant veins; flexor tendon for deep flexor tendon of the thumb and extensor tendon of 2. toe for long extensor tendon of thumb third: Postoperative×–ray a 4 week follow-up; right: adequate tweezer handle of indexfinger and thumb in follow up after 12 months).
Patient no. 10 suffered a mid-hand amputation injury by a circular saw (Fig. 6). In the emergency operation replantation of the middle hand was performed. Bony reconstruction of metacarpalia 2 and 3, as well as the base phalanx of the ring finger was achieved through stabilization with plate fixation. Multiple digital nerves were grafted with sural nerve segments. Destruction of the PIPJ-IV caused a secondary ulnar deviation of the 4th digit. The base phalanx VI showed non-union. Extensor tendon insufficiency was noted. The loss of osseous substance of the base phalanx precluded the use of a prosthesis. Maintaining finger ray length, axis and mobility were defined as goals for secondary reconstruction. Thus, due to limited TARM one year after primary reconstruction a vascularized toe joint transfer from the second toe including tenorrhaphy of its extensor tendon and the extensor digitorum communis 4 tendon of the ringfinger was performed. The missing bone segment in the toe was replaced with a small pelvic bone graft for toe preservation. The range of motion could be improved, the previous lag of extension was corrected. Twelve months after joint- transfer a lag of full flexion in PIPJ needed to be improved by tenolysis, a FDP-IV-tenorrhaphy and an arthrodesis of the transplanted joint were performed. The preoperative distance (5 cm) between hollow hand and the fingertips could be improved by the tertiary operation (3 cm) (Fig. 6). An improvement in keyboard typing was achieved for general use.
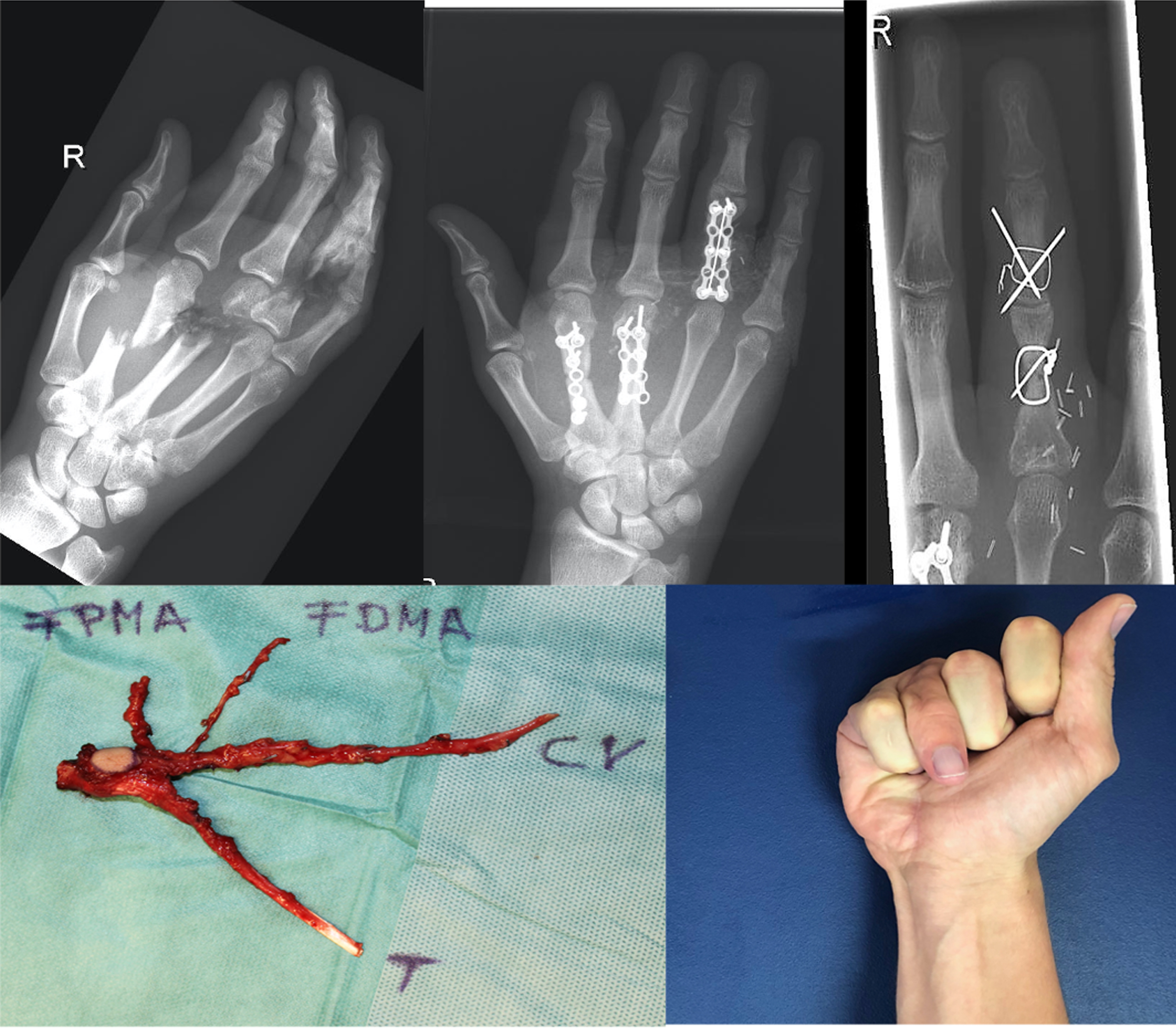
Pat. no. 10 (table 3) benefited from a PIPJ- II transfer of second toe to PIPJ- IV after subtotal mid hand amputation with primary revascularization and osteosynthesis. Upper left: subtotal mid hand amputation; upper middle: after replantation and plate fixation (PIPJ was destructed); upper right: postoperative x - ray after vascularized PIPJ- transfer of 2nd toe Down left: harvested PIPJ second toe (T= extensor tendon, CV = cephalic vein, FPMA = first plantar metatarsal artery, FDMA = first dorsal metacarpal artery. A skin island was maintained for perfusion monitoring); down right: function of ring finger after 12 month with an PIPJ flexion of 60°, maintaining flexion deficit of 3 cm from fingertip to hollow hand.
Some of the patient’ s outcomes are also available in the attached video supplement.
Thumb reconstruction showed TARM of IPJ 26 °±24.34° (n = 5, range 10 to 65°) and TARM of MCPJ 69 °±6.59° (n = 5, range 60 to 75°). The Kapandji score was measured 9.8±0.44 (n = 5, range: 9 to 10). For tripartite fingers and fingers with free joint transfer the TARM of DIPJ was 30°±34.94° (n = 8, range –20 to 80°); TARM of PIPJ 73°±28.75° (n = 8, range 20 to 100°) and TARM of MCPJ was 70°±21.45° (n = 8, range 20 to 90°).
Esthesia
The 2PD for the pulp following pulp transfer in the radial digital nerve distribution was: 7.75±1.66 mm (n = 8; range: 6–10 mm) and ulnar digital nerve 7.25±1.83 mm (n = 8, range 6 to 10 mm).
After joint reconstruction the 2PD in the radial digital nerve distribution was: 6±0.40 mm (N = 6, range 6 to 7 mm) and for ulnar digital nerve 6.1±0.40 mm (n = 6; range 6 to 7 mm). Only minor complications with local donor site wound healing disorder (n = 4) and an additional prolonged wound healing (n = 2) were seen in the whole cohort. Two patients needed revision of wound healing disorder with debridement and skin transplantation within the first 6 weeks following reconstruction.
Group II: alternative procedures (n = 12) (Table 4/5)
In this group local or free flaps were used for reconstruction of the pulp of the thumb. Procedures included for the thumb (n = 6) were: homodigital artery flaps (Epping/Moberg) (n = 2) or the venous flow- through flap (n = 1), Foucher’s first dorsal metacarpal artery flap (n = 1), Littler’s heterodigital neurovascular flap (n = 2) and a Venkataswami flap (n = 1) (Table 4/5). Follow up was 8 months, one patient was lost to follow up immediately after release from hospital (no. 4). In two cases reconstruction of tripartite fingers with soft tissue defects were performed with a venous flow through flap and a tubed groin flap. For reconstruction after open fractures of the PIPJ (n = 2) or the MCPJ (n = 1) an implantation of a silicone prothesis (Swanson finger joint implants; Fa Wright, USA) was used (n = 3). The time between injury and defect reconstruction was mostly primary (n = 10) just the implantation of finger prosthesis was performed secondarily (6–14 months). The hospitalization time for local flaps or joint reconstruction was 11.3±8.11 days (n = 12; range: 2 to 28 days). Joint replacements (n = 3) were performed with Swanson’s prosthesis (n = 3), delayed in two patients after unsuccessful primary reconstruction and twice in one patient. Implantation of prosthesis was first done for primary reconstruction and after implant failure (14 years after).
Patient no. 5 (Table 4) was an 83 years old female patient who sustained a soft tissue defect of her right thumb after saw injury. Considering her lack of compliance for a free pulp transfer and comorbidities, the decision was made to perform a venous flow through flap primary (Fig. 7). Patient no. 6 lost his distal phalanx at IPJ- level of the thumb in an accident. For coverage a neurovascular Epping- island flap was used. The sensory recovery was 2PD 4–6 mm. In comparison to his right thumb there was a loss of 3 cm in length. Kapandji score was 8 after 12 months. There was no wound healing disorder.

Pat. no. 5 (table 4) was reconstructed by an arterialized venous throughflow flap after she injured the distal phalanx of the thumb by circular saw (amputation level 1b). Upper left: Circular saw injury: upper right: arterialized venous throughflow flap (V 1-3: veins; N = N. cutaneus antebrachi medialis) Down left: follow-up at 2 weeks; down right: follow-up after 6 months.
Reconstruction of joints: Patient no. 10 (Table 5) benefited from an implacement of Swanson prosthesis after posttraumatic PIPJ-II arthrosis after subtotal amputation of PIPJ-II. Fourteen years later an increasingly painful range of motion led to replacement of the Swansons prosthesis and secondary reconstruction of the collateral ligaments. Active and passive motion was exercised before replacement by manual therapy. Intraoperatively the prosthesis showed broken. Postoperative range of motion was achieved: DIPJ-II: 20 °, PIPJ-II: 40° and MCPJ-II: 95° after 12 weeks.
Reconstruction of the thumb (n = 6) with local flaps showed a TARM for the IPJ 46°±32.09° (n = 5, range 20 to 90°) and MCPJ of 56°±13.41° (n = 5; range: 40 to 70°), Kapandji score was 8±1.41 (n = 5; range 7 to 10).
Tripartite fingers with local flaps showed following values: TARM of DIPJ 48.75°±3.53° (n = 2; range 70–75°); PIPJ: 80°±14.14° (n = 2; range 70–90°).
Reconstruction of joints (n = 3) showed TARM of DIPJ 30°±7.07° (n = 2; range 20 to 30°), PIPJ 48.33°±23.62° (n = 3; range 30 to 75°) and MCPJ 88.33°±7.63° (n = 3; range 80–95°).
Esthesia
All included patients (n = 12) after local flaps of the thumb or tripartite fingers or joints demonstrated sensory with 2PD of radial digital nerve 8.3±1.79 mm (n = 11, range 6–10 mm) and ulnar digital nerve 7.76±2.21 mm (n = 12; range 6 to 12 mm). Complications of the entire group were minor wound healing disorders at the flap (n = 2). No further operations were necessary.
Statistical analysis (Table 6)
The two groups showed no significant homogenous distribution in age and gender (p- value: 0.246). The statistical analysis was performed by means of t-test considering the following parameters: esthesia, TARM, complications and Kapandji score. There was no statistical difference in esthesia, TARM or complications (p-value > 0,05).
The Kapandji score showed a significant difference (p- value = 0.04) with a score of 9.8 in comparison to control group (Kapandji index = 8.0).
Discussion
The pulp of the finger, especially of the thumb, contributes to more than 50 % of the fingertip volume and is a specialised structure that permits fine motor activities and precise sensation. Its delicate tissue comprises neuro-vascular fibrofatty components which are stabilized by fibrous septa extending from the dermis to the periosteum of the distal phalanx.
Numerous specialised mechanoreceptors such as Meissner corpuscles provide a stunningly accurate sensation and may discriminate differences in prominences of 0.006 mm in height [26]. Finger pulp restoration may be oriented on the mechanism of injury, defect size, age, sex, expectations and occupation of the patient. Hand surgeons are frequently challenged by the unique requirements of soft tissue coverage of the hand. Whereas many smaller soft tissue defects without involvement of deep structures are amenable to healing by secondary intention or skin grafting, larger lesions and those with exposed tendon, bone, or joint often require vascularized coverage that allows rapid healing without wound contraction.
Restitutio ad integrum is challenging to impossible and constitutes one of the most common problems in severe hand injuries [27]. Even if possible conservative treatment may result in a prolonged wound healing period and lack of sensitized soft tissue substance. Consequently, difficulties to start physiotherapy and returning back to work until complete soft- tissue closure may occur. Therefore, in larger defects surgical reconstructions constitute the method of choice.
A variety of reconstructive procedures are available. Lemmon et al. developed an algorithm for soft tissue injuries of the fingertip, recommending a differentiated approach for each part of the fingertips of thumb and the tripartite fingertips [28, 29]. This work focusses on the reconstruction of special tissue of the pulp, all suggested procedures for defects larger than 1.5 cm like homo- and heterodigital flaps may not provide enough soft, fatty tissue as existent in the original pulp. The thin tissue layer of Foucher-flaps for instance may not restore total soft tissue constitution of the pulp of the thumb if its thickness is lost entirely. Local flaps are often described with adequate results but furthermore may be limited by their advancement capacity [14, 31].
Limited sensate properties using various donor nerves transferred to a different field of tactile sensation have been described [32, 33]. Cerebral plasticity which is responsible for central learning processes of tactile changes if nerves are transferred may be limited in mid-age and older age groups.
Free pulp flaps as well as partial/total transfers represent elegant but complex methods of reconstruction. Their effectiveness is constituted by their ability to tailor the particular operation to a specific injury pattern and patient type.
Due to the complexity of a free transfer, patient selection, as well as close consideration of his or her secondary conditions, is critical for accurate surgical planning.
Advanced peripheral arterial disease may be a contraindication to free toe transplantation, because the restitution of the microcirculation is of crucial importance for the oxygen supply of the graft [34, 35] whereby already the choice of anesthesia can influence the success of the procedure [36].
In our cohort of young and healthy patients, the free vascularised pulp transfer for defects larger than 1.5 cm was a safe method (only one case showed necrosis without the need of operative revision) to reconstruct like with like: The toe pulp consists of the same fibrofatty tissue like the pulp of the finger.
PIPJ and MCPJ represent fine examples of a highly-sophisticated biomechanical system in evolution. Substantial damage or loss cause severe impairments of range of motion, grip strength and digital length [37]. To this date, no artificial prosthesis has been introduced that may perfectly match as a substitute with natural freedom of motion, proprioception and strength paired with longevity. The idea of autologous joint replacement has fascinated dedicated hand and microsurgeons for decades [38, 39]. Joint transfer was modified to vascularised autologous transplants as described by Buncke et al. 1967 [40] and are useful for injuries located distal to the thumb saddle joint. A renaissance may be noted since the late 1990 s with a solidification of microsurgical operations as a safe and standard technique. A high significance of partial or total toe and larger patient series may be noted in Asia [41–43] Common techniques we used in our series are for example have been described by Ellis et al. [42]. Proximal injuries with loss of the thumb saddle joint or the first metacarpal bone benefit from pollizisation to preserve joint mobility. Patient selection should include a healthy, compliant and motivated cohort to be eligible for toe transplantation. (Relative) contraindications comprise vascular disease, major illness, lack of compliance or acute trauma to the donor foot [44]. Present comorbidities may require a straight-forward solution. Local or island flaps (Littler/Moberg/Foucher) or venous flow through flaps may render solutions even as additional features for covering defects after joint transfer [45].
Amputation proximal to the middle of the proximal phalanx of the thumb affects grasping and pinching because of the longitudinal change. Common procedures are the wrap around procedures [46] which usually utilize partial volume of the great toe, but include the entire nail and onychium [14]. In our cohort, we used modified wrap- around- technique using bony and soft tissue components while the nail was excluded. Preserving the proportions of the thumb compared to the great toe necessitated a volume reduction [47].
Reconstruction for posttraumatic destruction of the PIPJ and MCPJ poses a challenging problem. Current treatment options include amputation, arthrodesis, silicone implant arthroplasty, Pyro-Carbon implant arthroplasty, and vascularized toe joint transfer [48, 49]. A literature research by Chung et al investigated the arc of motion as the most important outcome after toe joint transfer, silicone implant arthroplasty and Pyro- Carbon arthroplasty. All three methods achieved adequate mobility, but the authors favored arthroplasty because of greater complications with toe joint transfer. The group stated in their review that complications were difficult to find in literature. Our experience in vascularized partial toe (-joint) transfer are just minor complications (n = 4). Prolonged wound healing especially at donor site was common, but no flap failure was seen. The arc of motion was greater with arthroplasty compared to toe- transfer in literature [50]. In our cohort the requirement of mobility was mostly an opposable thumb measured by Kapandji score. In our cohort the Kapandji index showed significant difference between group I (9.8) compared to alternative reconstructions (group II = 8.1). Even though toe transplantation can be offered as immediate reconstruction for amputation of digits like Woo et al. with high success [51, 52], we believe optimal functional and esthetic outcomes are achieved by optimal setting, two teams and clean recipient sides.
A conditio sine qua non for successful arthroplasty is sufficient bony substance for abutment. In case no. 10 (Table 5) insufficient bony substance precluded arthroplasty. Furthermore, arthroplasty in general may only provide a limited life span, in our cohort a replacement of pip-joint in the same patient (no. 10/table) was necessary after 14 years because of implant failure. The durability varies depending on the indication and the affected joint (PIPJ or MCPJ). The use of cement may affect the life period. In conclusion, the failure rate may increase up to 16% for PIPJ- arthroplasty over twenty-five years [53]. Implant arthroplasty of the finger joint is a costly procedure, in terms of both implant cost and secondary revision surgery [50]. Furthermore, the patient’s working capacity is interrupted after primary and revision surgery due to motion and grip limitations especially in manual workers as the main cohort of amputation injuries.
For the MCPJ- arthroplasty the Swanson prosthesis seems to be replaced by a newer generation of pyrolytic carbon protheses. However, there are still limitations like implant failure, adhesion of ligaments or fracture [54, 55]. As a common perequisite, intact stabilizers as collateral ligaments are needed for joint arthroplasty [56]. Due to minor donor site impairment and rapid recovery of normal gait the whole second ray may be amputated after harvesting of a joint graft on the second toe [37]. In our cohort the second ray was maintained with a bone graft in one patient, and only minor wound healing disorders occurred. Following amputation of the second ray all other patients recovered full mobility within 6–8 weeks.
In our cohort the reconstruction of the thumb distal to the CMCJ preserved opposition to the tripartite fingers which is the main function to be restored. The function of the CMCJ -I is paramount to optimal function. Possessing a biconcave saddle and a complex set of ligaments, this basal joint provides the greatest degree of motion, but the least stability of the articulations of the thumb ray.
Frykman et al. evaluated in the beginnings of toe transplantation, 20 toe to hand transfers in 17 patients and noted total active motion of the transplanted great toe to be 48 degrees. IPJ- motion was 27 degrees and MCPJ- motion was 27 degrees [57]. 2PD was less than or equal to 15 mm in 65% of patients. In our cohort esthesia (2PD: 7.75/7.25) and TARM of IPJ (26°) and MCPJ (69°) showed superior results, even if there was no statistically difference towards control group.
Larger studies showed comparable results like Buncke et al. group with average MCPJ- motion of 44° and IPJ- motion of 40° in 161 patients with thumb reconstruction [58].
Long-term studies were able to prove the objective and subjective satisfaction after toe transplantation in esthetic and functional parameters [59]. As a limitation to our study, no questionnaires were used to evaluate patient satisfaction. A further limitation is the missing grip strength or pinch as a predictor for complete hand function especially for craft workers.
Conclusion
Healthy patients with adequate compliance benefit from different options of partial or total toe transfer. It is a safe procedure to achieve comparable sensory recovery, maintain ray length and provide long-lasting outcomes. The loss of parts of a toe or metatarsus does not restrict the overall mobility. The effectiveness of this procedure and its high surgical success rate seem to justify toe transfer. It may be recommended due to its ability to tailor the particular operation to a specific injury pattern and patient type.
Regarding the profile of complications and variety of surgical procedures there is still a need for further investigations in long term survival of different joint transfers. So far complications seem to be still less well-documented and therefore hard to quantify in literature.
In summary, neurovascular partial or total toe flaps add a powerful option to the arsenal of the microsurgeon to sufficiently reconstruct two and tripartite digits with respect to function, sensation and aesthetic appearance.
Financial disclosure
None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Contributions
All authors stated above meet the required conditions for authorship:
1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; 2) drafting the article or revising it critically for important intellectual content; 3) final approval of the version to be published; 4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethical approval
This study was approved by the Institutional Review Board Committee of the University of Regensburg (no. 20-1845-104) and was designed in accordance with the Helsinki Declaration.
Informed consent
Informed consent was obtained of all patients prior to the free flap procedure or alternative operation.