
Abstract
BACKGROUND:
The use of dyes like Indocyanine green (ICG) and Patent blue facilitates the identification of lymphatic vessels during lymphaticovenous anastomosis (LVA) surgery. However, some patients experience “staining failure”. In these cases, no stained lymphatic vessels can be detected, making supermicrosurgical LVA even more complex.
OBJECTIVE:
This study aims to investigate patient-related factors that may interfere with lymphatic vessel staining during LVA.
METHODS:
A retrospective study was conducted on 30 patient charts, focusing on patient characteristics and the staining quality of ICG and Patent blue dye. Statistical analyses were performed to identify correlations between variables.
RESULTS:
Significant correlations were found between higher age and secondary lymphedema, longer duration of lymphedema in male patients until surgery and reoccurring cellulitis and Patent blue staining. Notably, recurrent infections to the lymphatic system resulted in inferior staining ability during LVA surgery.
CONCLUSIONS:
Due to staining failure the detection of functional lymphatic vessels remains challenging in LVA surgery. A more extensive preoperative workup is recommended for patients with recurrent cellulitis to optimize surgical feasibility and procedure quality in LVA treatment for lymphedema.
Keywords
Introduction
Lymphaticovenous anastomosis (LVA) has gained significant popularity as a microsurgical technique for the management of lymphedema in recent years. This supermicrosurgical procedure involves creating bypasses between lymphatic vessels and epifascial veins, enabling the direct drainage of excess lymphatic fluid into the venous system and subsequently reducing the appearance of lymphedema in the affected area of the body [1].
Currently, many surgeons employ the use of Indocyanine green (ICG) and (Patent-)blue dyes to aid with the identification of small-caliber lymphatic vessels during the procedure. These lymphophilic dyes stain lymphatic vessels filled with clear lymphatic fluid, facilitating their detection intraoperatively [2–6]. Furthermore, ICG lymphography findings serve as an indicator of lymphedema severity and lymphatic dysfunction [3, 7].
In our clinical observations, however, we have encountered a subset of patients that experiences what is referred to as “staining failure.” In these cases, no stained lymphatic vessels can be identified during the intraoperative phase, making the application of LVA considerably more challenging. Consequently, patients exhibiting staining failure may benefit from more extensive preoperative diagnostic techniques, such as MR lymphography, to enhance the visualization of lymphatic vessels [8]. Foremost, in patients expected to experience staining failure, a comprehensive evaluation of the potential risks associated with dye injection, including allergic reactions, is imperative [9]. It is crucial to carefully consider and balance these risks against the potential benefits of the procedure.
The objective of this retrospective study was to investigate patient-related factors that may interfere with the staining ability of lymphatic vessels during LVA. By identifying these factors, we aim to enhance our understanding of the challenges associated with the surgical application of lymphaticovenous bypasses. Ultimately, this knowledge may contribute to refining patient selection criteria and optimizing surgical outcomes for individuals with lymphedema.
Material and methods
Patients
This retrospective trial was conducted based on ethical approval and in accordance with the Declaration of Helsinki. It was registered in a public German trial registry (DRKS 00031962) and approved by the institutional ethics committee (23-3369-104). Informed consent was obtained from the patient whose intraoperative findings are shown.
A total of 30 patient charts were reviewed and included into our investigation.
Charts containing insufficient documentation according to our in-house standard were excluded. The review was focused on patient characteristics and the operation protocol regarding the staining quality of ICG and Patent blue dye.
Dye administration
0.2 ml of ICG (5 mg/ml) were administered 24 hours preoperatively in the first web space at the dorsum of the foot or hand intradermally and once again together with 0.2 ml (25 mg/ml) of Patent blue dye when the patient was already in the operating theatre under vital parameter monitoring. The second dye application was injected five centimetres below the surgical incision.
Statistics
For correlation analysis of two nominally scaled variables, Phi-coefficient was calculated when both variables had only two values (e.g., “yes” and “no”). When one variable was scaled nominally and the other ordinally, the Chi-Square test was used. For two ordinally scaled variables, as well as one ordinally and one metrically scaled variable, Spearman Rho was calculated. Pearson coefficient was determined for two metric scaled variables. When one variable was nominally scaled and another was metric, the eta coefficient was employed. In the rare case of a correlation between a metric and a dichotomous variable, the point biserial correlation was used. A p-value of < 0.05 was set to indicate statistical significance. Analysis was performed using IBM SPSS Statistics for Mac, version 29.0.0.0.
Results
Characteristics
The mean patient age was 53 (SD 13) years and 13.2 (SD 10) years passed since the lymphedema occurred first. There were 24 lymphedemas stage two and six lymphedemas stage three according to Yamamoto [7]. LVA surgeries were performed between January and June 2023. Dermal backflow pattern showed a splash in seven, star dust in 19 and diffuse distribution in four patients, respectively. Further patient characteristics are shown in Table 1 and intraoperative findings in Table 2.
Patient characteristics
Patient characteristics
Intraoperative findings
To identify coherences between the parameters a correlation coefficient was calculated. Only three significant pairs were found that are displayed in Table 3.
Patient and surgical parameters indicating statistically significant correlations
Patient and surgical parameters indicating statistically significant correlations
A positive correlation was found for age and secondary lymphedema indicating that advanced age was associated with secondary causes more frequently. Sex and duration negatively correlated, showing that a long latency until surgery tended towards male sex. Reoccurring cellulitis (>1) also negatively correlated with Patent blue staining, pointing towards less staining ability with multiple preceding infections (Fig. 1).
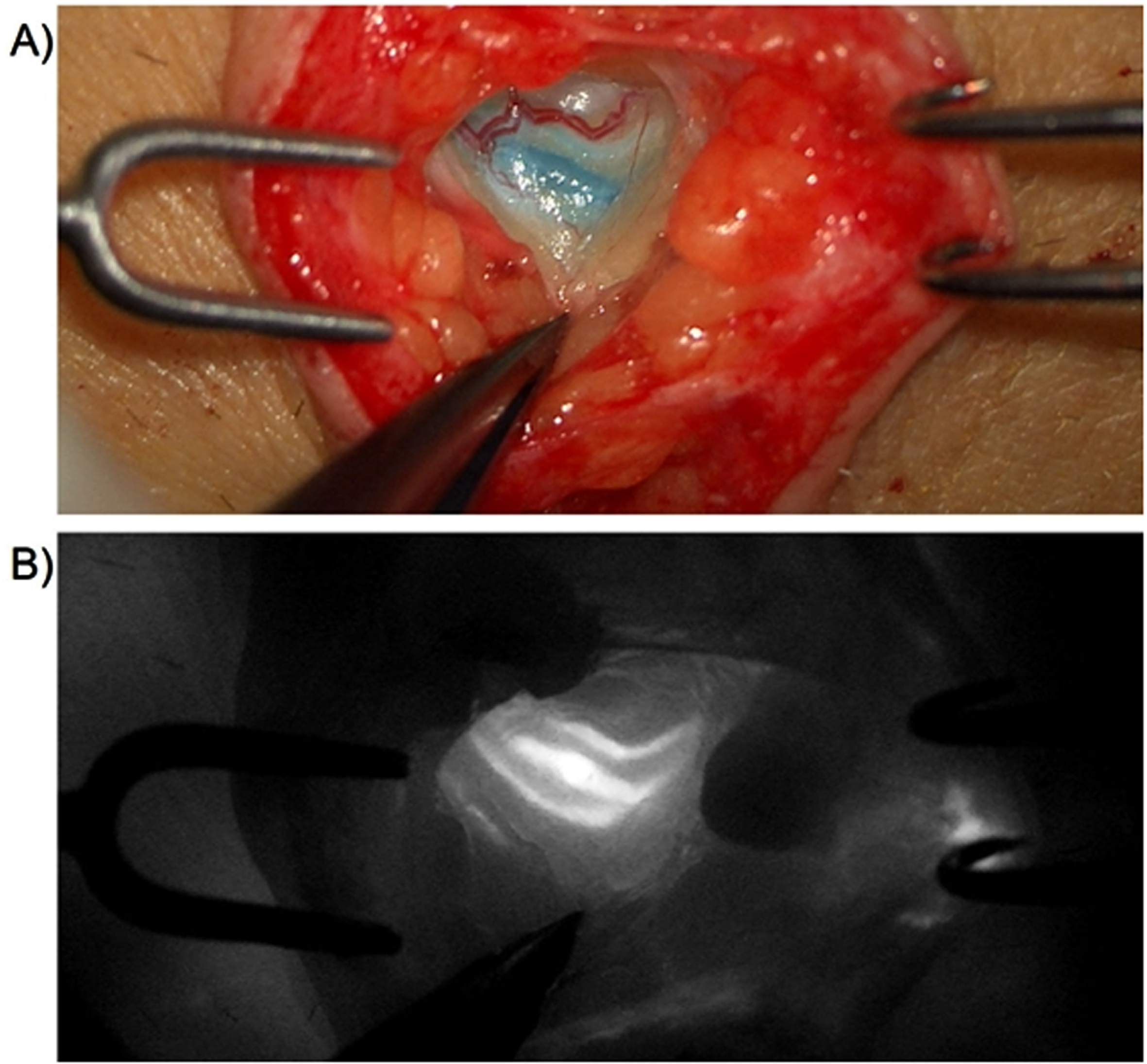
Intraoperative images. A) Surgical situs displaying a bicolour-stained lymphatic vessel after preoperative Patent blue dye and ICG application according to the trial center’s standard. B) ICG lymphography showing a bright fluorescence signal of the lymphatic vessel.
The lymphaticovenular bypass is an increasingly used surgical procedure in the treatment of chronic lymphedema. Despite technical advances in fluorescence intensifying microscopes the pure detection of functional lymphatic vessels often remains a surgical challenge.
In an attempt to further contribute to the understanding of intraoperative lymphatic staining, we tried to identify patient characteristics which may aid the surgical decision making preoperatively. We found that reoccurring cellulitis negatively affects the lymphatic staining ability with Patent blue dye.
The use of dye to aid the detection of functional lymphatic vessels and lymph nodes during surgery is a well-established tool. ICG and Patent blue dye are commonly used substances in the preoperative evaluation as well as intraoperative patency testing of lymphovenous shunts [4–7, 10]. Not all patients show similar staining qualities resulting in heterogeneous surgical feasibilities of the LVA [11]. Park et al. found lower completion rates of an LVA surgery, when fewer functional lymphatics with high flow on ICG fluorescence were detected [11]. Our results tend towards these findings, as only 63% of our patients demonstrated ICG, and 33% Patent blue staining in the intraoperative setting, respectively. Indeed, if non-dye responders have inferior clinical outcomes, may not be shown by our results as at least one LVA was performed in every case.
A similar study including the clinical results after lymphatic surgery was conducted by Hara et al. who investigated lymphatic staining with ICG during LVA surgery and compared single to multiple-injection groups [2]. In the multi-injection group, ICG was applied in a way that numerous lymphosomes may be stained. They found superior surgical results in terms of identification of more functional ectasis type lymphatic vessels and a significant larger circumference reduction in the multi-injection group [2].
In terms of surgical feasibility, it seems conclusive that larger vessels may easier and more reliably be used in an anastomosis. Preoperative characteristics of patients with these favoring conditions are not officially defined yet. However, secondary reasons for lymphedema are well described and cellulitis simultaneously remains as a common cause and sequelae. When bacteria enter the skin barrier, the infection spreads within the subcutaneous tissue and adjacent lymphatics, leading to the pathognomonic clinical presentation. This may lead to lymphatic dilatation and edematous changes within the vessel wall. In case of irreversible damage, sclerosis and lymphedema may occur [12, 13]. We found significantly less lymphatic staining with Patent blue dye after more than one reported episode of cellulitis. This seems coherent respecting the underlying pathophysiology. A thorough preoperative selection process therefore is warranted. Rodriguez et al. described a systematic and stepwise method to identify their patients preoperatively [14]. They reported a 100 % lymphatic detection rate in 677 anastomoses demonstrating that intraoperative staining alone is not the only key factor for successful surgery [14].
Previous reports have documented allergic reactions to Isosulfan blue dye, a specific Patent blue dye derivate, with reported incidences ranging from 0.6% to 2.5% [9]. In patients with suspected staining failure, it is imperative to meticulously assess the potential risks associated with dye injection and carefully balance them against the potential benefits. This is particularly relevant in case of subcutaneous injection of ICG which is an off-label use in lymphography [15, 16].
Our study has several strengths and limitations. The retrospective nature of our investigation depicts uncertainties of the intraoperative situation. However, the standardized in-house protocol of a certified lymphatic center guarantees a high quality pre- and intraoperative assessment and therapy in each patient.
Conclusion
The identification of patient-related factors influencing the staining ability of lymphatic vessels is a novel field of investigation. This study aims to explore these factors, with the goal of improving patient selection and optimizing the application of LVA in the treatment of lymphedema. In conclusion, our results demonstrate that recurrent infections to the lymphatic system result in inferior staining ability during lymphaticovenous bypass surgery. Consequently, the identification of functional lymphatics with larger diameters becomes less likely, resulting in a more challenging surgical procedure. According to the results of this study a more extensive preoperative workup is recommended when performing LVA in patients who suffered from recurrent cellulitis to increase surgical feasibility and optimize the overall quality of the procedure.