
Abstract
BACKGROUND:
The response of Renal Cell Cancer (RCC) to tyrosine kinase inhibitors (TKI) has been well established. Although these stratifications have been established for TKI response and prognosis, these parameters have recently been used to predict immunotherapy response in RCC. We aimed to use a combination of clinical parameters of International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) risk groups and metastatic sites at the time of diagnosis to predict the effectiveness of immune checkpoint inhibitors in malignant melanoma (MM).
METHOD:
In this cross-sectional study, we retrospectively analyzed the demographic information, metastatic sites, and IMDC risk group data. The blood parameters were included in the first cycle of nivolumab treatment.
RESULTS:
The OS was statistically different between the RCC and MM groups in terms of the IMDC. In univariate analysis of stage at diagnosis, CRP levels and bone and bone marrow metastases were confirmed to be prognostic factors in the MM population in terms of OS. Brain metastasis was a prognostic factor for RCC, whereas sex, line of treatment, LDH, bone, and splenic metastasis remained significant in patients with MM in terms of OS. Brain metastasis was prognostic in both cancer types in multivariate analysis in terms of PFS. In addition to brain metastasis, LDH levels and lung, liver, and splenic metastases also affect PFS in patients with MM undergoing nivolumab treatment.
CONCLUSION:
In our study, the IMDC was confirmed to be a prognostic factor for MM. The IMDC groups were similar, except for the favorable RCC and MM groups. Different metastatic sites were prognostic, similar to the IMDC risk group in the MM group.
Introduction
Immune system and tumor-driven inflammation are important hallmarks of cancer [1]. Genetic instability, angiogenesis, and cell growth have been suggested to be the main sources of chemokines and cytokines related to chronic inflammation. Cytotoxic T and B cells, which are influenced by these mediators, play a major role in the detection of tumors and elimination of cancer cells [2, 3, 4, 5].
Risk stratification due to the clinical characteristics of patients is used for prognostic evaluation of renal cell cancer (RCC). The response to tyrosine kinase inhibitors (TKI) in RCC has been well established over a long period [6, 7]. Although these stratifications have been established for TKI response and prognosis, these parameters have recently been used to predict immunotherapy response in RCC. In a recent trial, the combination of nivolumab and ipilimumab showed a superior response to sunitinib in intermediate- and poor-risk RCC groups [8]. Although two more trials have used these risk stratifications for immunotherapy and tyrosine kinase inhibitor combinations, the possible imbalance in TKIs may decrease the value of clinical factors [9, 10]. International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) risk groups may have expanded their use to different cancer types receiving immunotherapy and TKI.
The immune system is another aspect of the immune response of malignant cells [11, 12]. As well as tumor-infiltrating lymphocytes, peripheral immune cells are important for predicting immunotherapy response. Ferrucci et al. reported that baseline increased absolute neutrophil counts correlated with decreased overall survival (OS) and progression-free survival (PFS) in metastatic malignant melanoma treated with ipilimumab [13].
C-reactive protein (CRP) that is induced by IL-6 may show an immunotherapeutic response. In metastatic RCC patients whose CRP levels remain high after nephrectomy, poorer outcomes have been reported with INF-
The Royal Marsden Hospital (RMH) scoring system, combining albumin, LDH levels, and the number of metastatic sites, showed a predictive effect on survival in multiple cancer types in phase 1 trials [18, 19]. This scoring system has not yet been tested as an immunotherapeutic agent. Previous studies have shown decreased survival in patients with breast, bladder, and colorectal cancers with liver metastasis [20, 21, 22].
With these developments and further understanding, the cancer-immune system relationship may force us to use dynamic nomograms to select patients who will benefit from immune checkpoint inhibitors. In this study, we aimed to use a combination of the clinical parameters of IMDC risk groups and metastatic sites at the time of diagnosis to predict both the effectiveness and detrimental effects of immune checkpoint inhibitors in patients receiving nivolumab for malignant melanoma (MM) and RCC.
Material method
The flowchart of the study: Study population selection and the parameters evaluated were shown.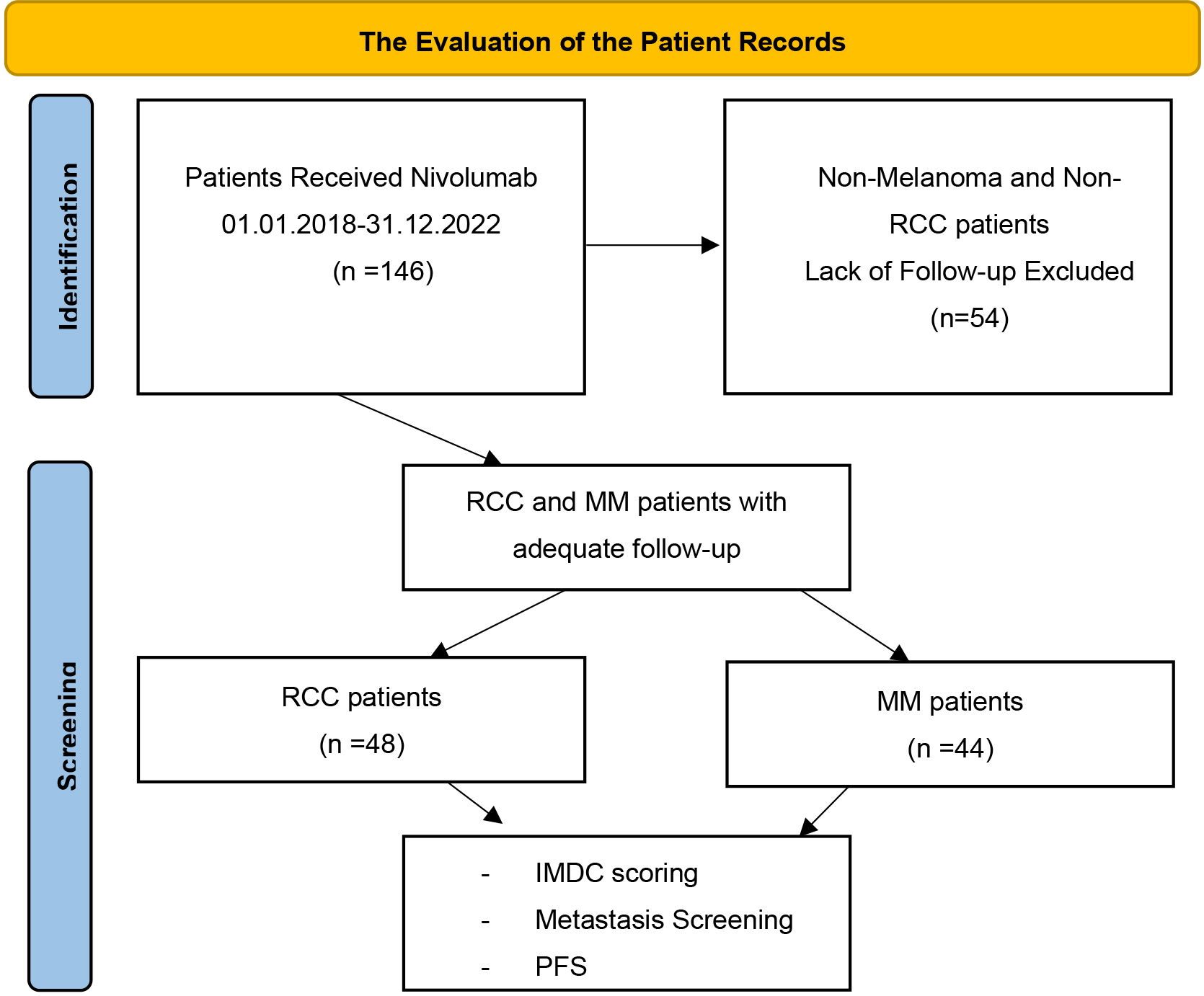
This cross-sectional study retrospectively analyzed the archives of the Antalya Education and Research Hospital Medical Oncology clinic between 2016–2022. Of 146 patients, 92 who received nivolumab between 2018–2022 were included in the study. Patients who received nivolumab and had adequate follow-up, clinical information, and laboratory parameters with appropriate imaging for the evaluation of treatment response were included in the study. Patients who lacked clinical parameters in the IMDC risk and follow-up groups were also excluded [6]. Karnofsky score component was converted from the patients’ data of the Eastern Cooperative Oncology Group (ECOG) Performance Score (PS), which is more utilized in current practice [23, 24]. Demographic information, metastatic sites, IMDC risk group data, CRP levels, diagnosis, treatment initiation and progression, and the last control times were recorded. In addition, the total number of treatment lines and the nivolumab line of treatment (LOT) were recorded. The blood parameters were included in the first cycle of nivolumab treatment (Fig. 1).
Statistical analysis
Statistical analyses were performed using SPSS software (Statistical Package for the Social Sciences, version 22.0. SPSS Inc, Chicago, IL, USA). The Kolmogorov-Smirnov test was used to determine whether the data conformed to a normal distribution. Descriptive data are presented as either means or medians for continuous variables, and frequencies and percentages are reported for categorical variables. Kaplan-Meier curves were used to determine the differences in survival. Chemotherapy responses were defined based on radiological reports. Differences between groups were tested using the chi-square test. Cox regression analysis was performed to evaluate prognostic factors. These factors cannot converge or be outfitted from the analysis. The cutoff values of prognostic factors determined both the IMDC categorization and ROC analysis.
Ethics
This study was approved by the local ethics committee of Antalya Education and Research Hospital, and the trial was conducted in accordance with the principles of the Declaration of Helsinki.
Results
The comparative characteristics of the study population according to diagnosis. There were statistical difference in four categories: Stage at diagnosis, line of treatment, total lines of treatment received and IMDC groups
The comparative characteristics of the study population according to diagnosis. There were statistical difference in four categories: Stage at diagnosis, line of treatment, total lines of treatment received and IMDC groups
One-hundred forty-six patients who received nivo-lumab were retrospectively analyzed, and 92 patients were enrolled. There were 48 patients with RCC and 44 with MM. The median ages of the patients with RCC and MM were 65 and 61.5 years respectively. Male dominance was observed in both groups with no statistical differences. There was no difference in the ECOG performance scores between the groups (
The Kaplan-Meier curves of RCC patients according to IMDC groups for OS. A statistically significant difference was observed between three groups. The median OS was not reached in intermediate IMDC group.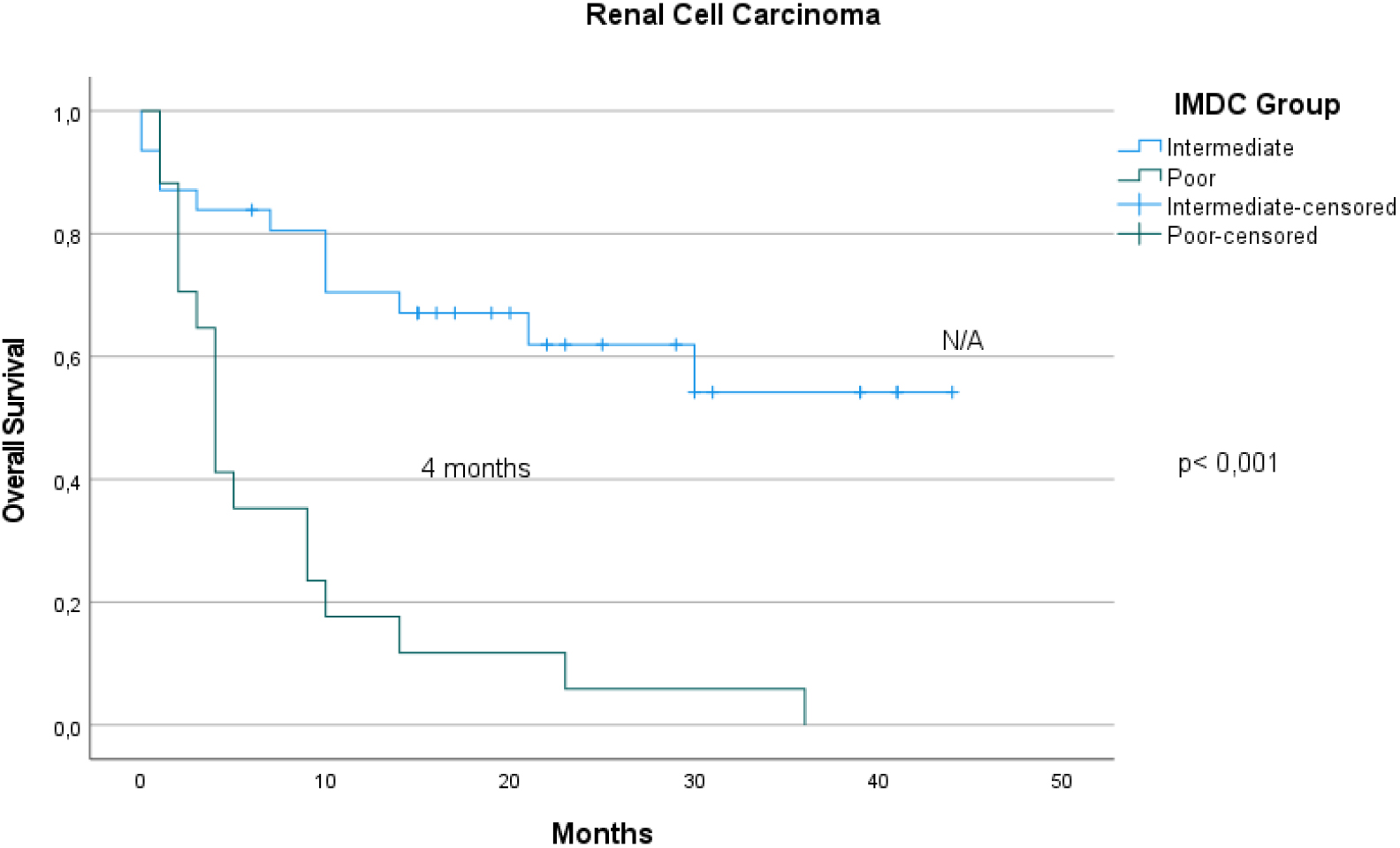
The Kaplan-Meier curves of MM patients according to IMDC groups for OS. A statistically significant difference was observed between three groups. The median OS was not reached in good IMDC group.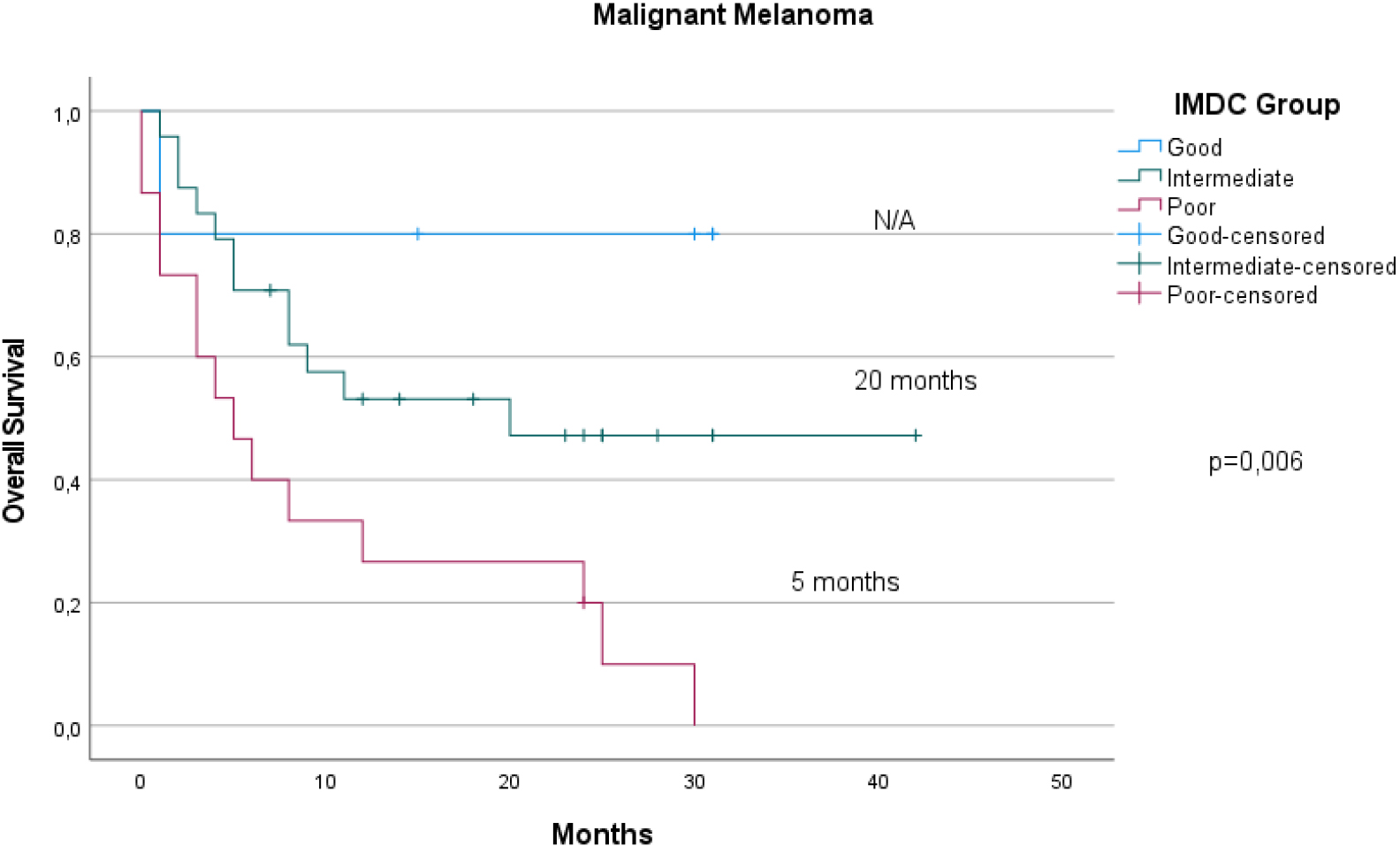
The univariate analysis of the study population according in terms of PFS according to diagnosis. Gender, IMDC group in RCC and bone marrow metastasis in MM were statistically significant
Met: Metastasis; CRP: C Reactive Protein; LOT: Line of Treatment;
The univariate analysis of the study population according in terms of OS according to diagnosis. IMDC groups, CRP category, lung and spleen metastasis in RCC and IMDC groups, stage at the diagnosis, CRP category, bone and bone marrow metastasis were statistically significant
Met: Metastasis; CRP: C Reactive Protein; LOT: Line of Treatment;
The OS was statistically different between the RCC and MM groups in terms of the IMDC (Figs 2, 3) (
The Kaplan-Meier curves of RCC patients according to IMDC groups for PFS. Border-line statistical significance was observed between groups.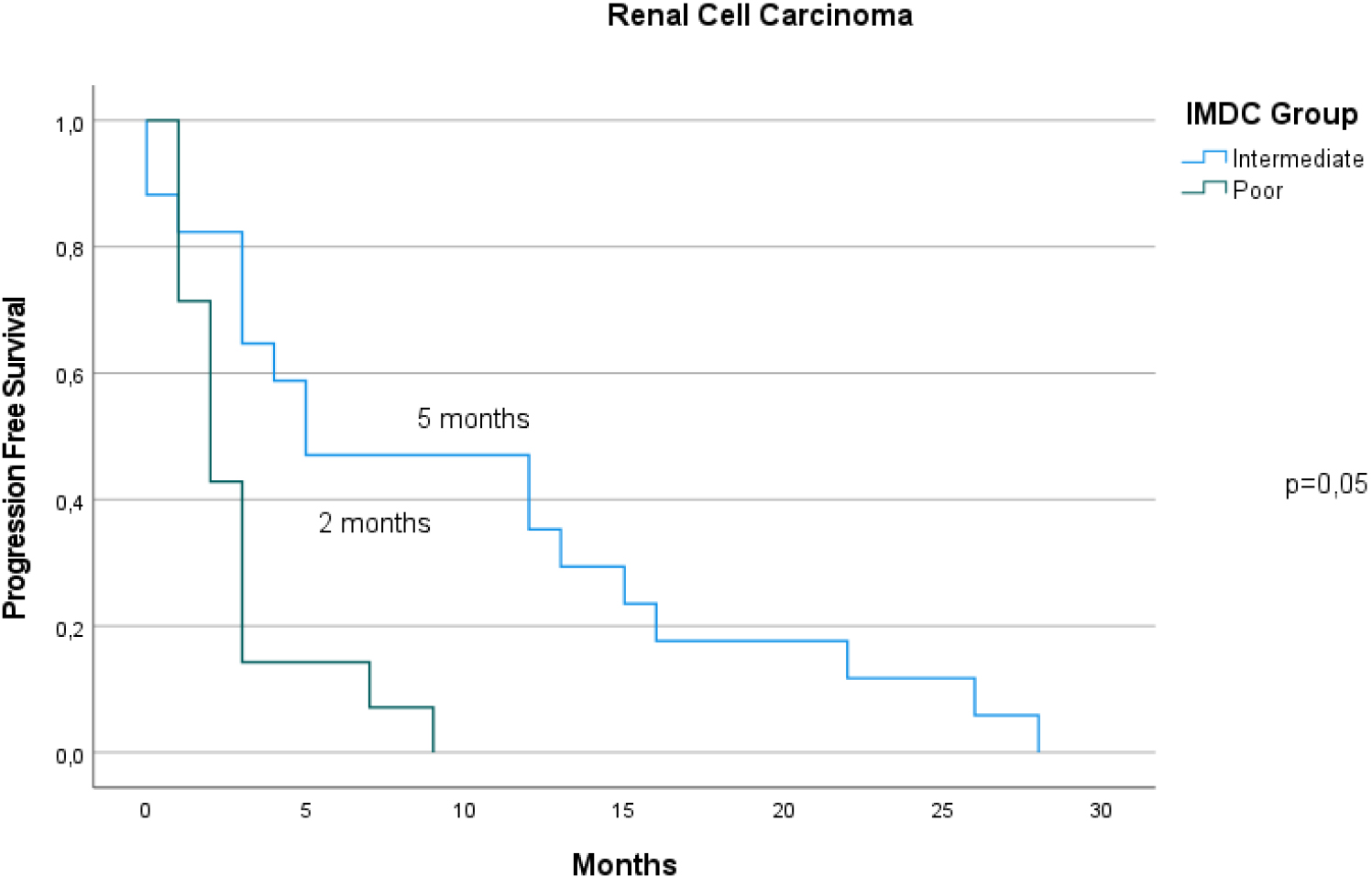
The Kaplan-Meier curves of MM patients according to IMDC groups for PFS. No statistical difference was observed.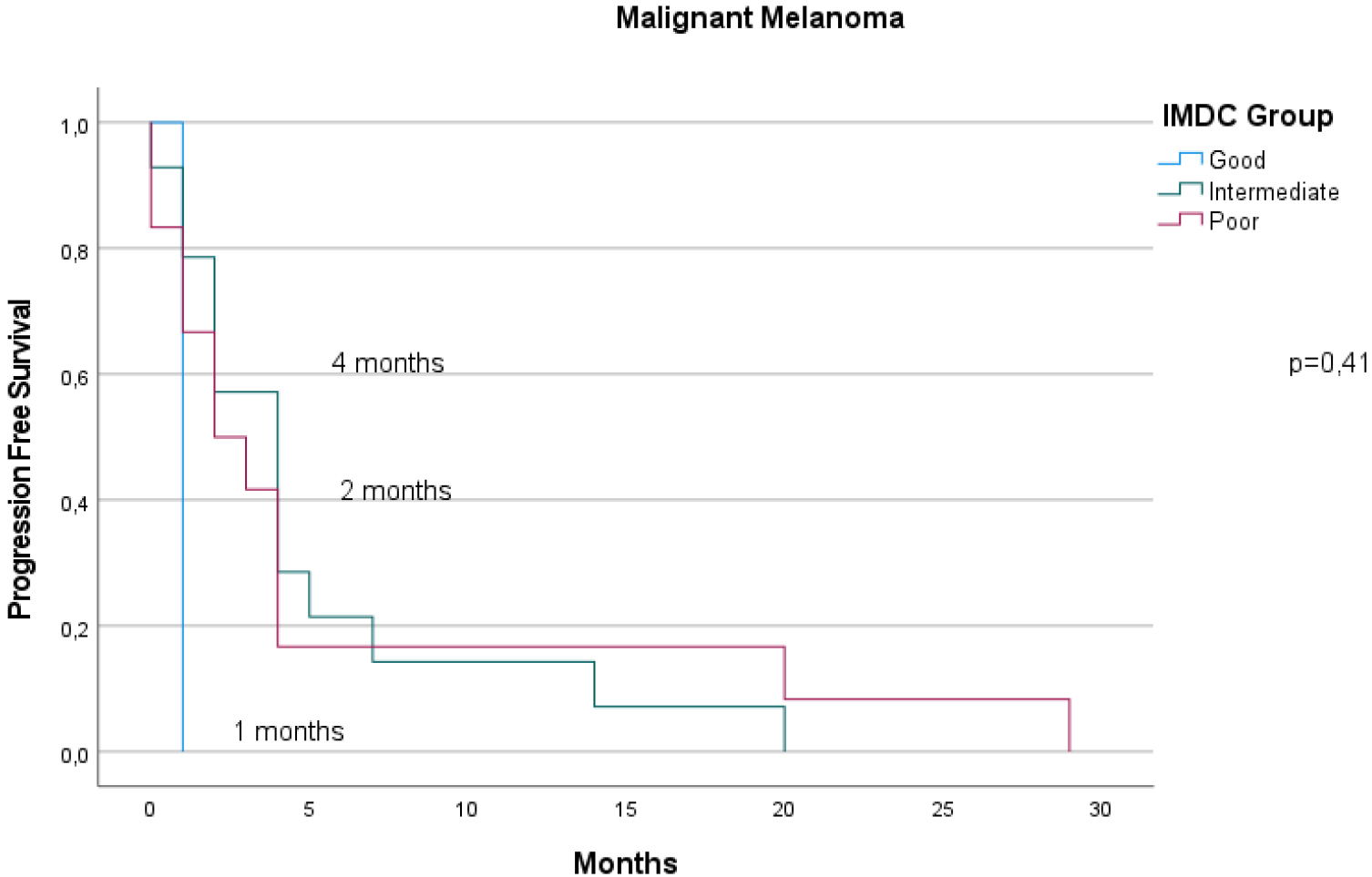
In terms of PFS, sex and IMDC were predictive factors in the RCC group, whereas only bone marrow metastasis was statistically significant in the MM group. The median PFS times for the intermediate and poor prognostic groups were 5 and 2 months, respectively (
The multivariate analysis of the study population according in terms of OS according to diagnosis. Brain metastasis in RCC and gender, bone metastasis, LDH levels and total lines of treatment in MM were statistically significant
Met: Metastasis; CRP: C Reactive Protein; LDH: Lactate Dehydrogenase; LOT: Line of Treatment.
The multivariate analysis of the study population according in terms of PFS according to diagnosis. Brain metastasis in RCC and LDH levels, lung, liver, brain, and spleen metastasis in MM were statistically significant
Met: Metastasis; CRP: C Reactive Protein; LDH: Lactate Dehydrogenase; LOT: Line of Treatment.
Multivariate analysis of the study population according to OS and PFS according to diagnosis is shown in Tables 4 and 5, respectively. In terms of OS, brain metastasis was a prognostic factor for RCC, whereas sex, LOT, LDH, bone, and splenic metastasis remained significant in MM patients.
Brain metastasis was predictive of both cancer types in the multivariate analysis in terms of PFS. In addition to brain metastasis, LDH levels and lung, liver, and splenic metastases also affect PFS in patients with MM undergoing nivolumab treatment. These parameters were confirmed to be independent predictive factors for nivolumab treatment in patients with MM.
To our knowledge, this is the first study to evaluate IMDC risk score in combination with metastatic sites in patients with different cancer types receiving immunotherapy. In our study, although the components of the IMDC groups were similar between patients with RCC and MM, there was a difference in the IMDC scores and groups between diagnoses. In contrast, the IMDC group was associated with better prognosis in terms of OS in both RCC and MM.
There has been increased effort to understand the relationship between tumors and the immune system. Some studies have attempted to establish immunograms for patients receiving immunotherapies [25]. Baseline peripheral blood parameters were evaluated in patients with lung cancer who received nivolumab. Immunotherapy response may be more related to the immune response than tumor type [26]. For patients receiving nivolumab compared to non-small cell lung cancer and RCC, increased neutrophil-to-lymphocyte ratio at the 6
Likewise, peripheral blood parameters and metastatic organs are important in determining patient prognosis. Although this is a highly investigated area, there is still a lack of literature on patients receiving immunotherapy. In a study in which phase 1 study of patients, liver metastasis was reported to have a significantly shorter OS and a trend toward shorter PFS. Although one-third of the study population included patients with MM, a subgroup analysis reported outcomes [36]. Different to this study, we found that metastatic sites had more prognostic effects, especially in patients with MM receiving nivolumab. In addition, the RMH score, which included the number of metastatic sites, was used in this study [36]. We did not determine the number of metastatic sites in this study.
Limitations
The study was retrospectively designed to limit data quality. Additionally, the study population was too small to identify certain factors. Bone marrow metastasis was excluded from the proper analysis using Cox regression. Although the number of treatments and the line of nivolumab were added to the statistics, the difference in the treatment of these diseases was underestimated. A comparison was made between the study groups; however, there was an imbalance in some factors were imbalanced. The PDL-1 status was not available for the study population.
Conclusion
In our study, the IMDC was confirmed to be a prognostic factor for MM. The IMDC groups were similar except for the favorable RCC and MM groups. Different metastatic sites were prognostic, similar to the IMDC risk group in the MM group. A combination of immune subsets with metabolic and clinical factors may be less prone to failure and have the potential to provide new or currently used predictive scores. The validity of combined scores should be tested in larger studies with clearly defined patient groups.
Footnotes
Acknowledgments
This study did not receive any funding from commercial or non-commercial organizations. The study database is available on demand.
Conflict of interest
The authors declare no conflict of interest.
Author contributions
Conception: IB.
Interpretation or analysis of data: AHO, YS, and IB.
Preparation of the manuscript: IB.
Revision for important intellectual content: AHO, YS, and IB.
Supervision: IB.