
Abstract
BACKGROUND:
Platelets play a key role in tumor progression and metastasis. C-type lectin-like receptor 2 (CLEC-2) is the receptor expressed on platelets and the marker of platelet activation.
OBJECTIVE:
This study aims to determine whether soluble CLEC-2 levels differ between patients with benign colorectal polyps and those with colorectal cancer (CRC).
METHODS:
We measured plasma soluble CLEC-2 by enzyme-linked immunosorbent assay in 150 patients with colorectal polyps, 150 CRC patients without metastasis, 150 CRC liver metastasis, and 150 control subjects.
RESULTS:
The CRC patients had higher soluble CLEC-2 levels than patients with colorectal polyps (
CONCLUSIONS:
CRC patients have higher CLEC-2 levels than patients with colorectal polyps and healthy controls. Moreover, there is a significant difference in CLEC-2 levels among polyp subtypes. Further research is warranted.
Introduction
Colorectal cancer (CRC) is the third most common malignant cancer with and the second highest mortality rate [1]. Despite much progress has been made in treatment, the long-term survival of CRC patients remains poor, especially for advanced and metastatic CRC patients [2]. Furthermore, more than 20% of CRC patients are diagnosed with distant metastasis at initial diagnosis [3]. Therefore, it is extremely important to early detect of precancerous colorectal lesions. Although colonoscopy is the gold-standard screening test, it is an invasive test and there is a risk of perforation [4]. Thus, identifying new potential targets is needed.
Platelets has an essential role in cancer progression and metastasis [5]. Platelets-tumor cell interactions and stimulated signaling pathways have been identified as fundamental determinants of cancer metastasis [6, 7]. There is plenty of evidence to suggest that increased platelets are associated with a poor prognosis in various types of cancer, such as pancreatic cancer, gastric cancer, colorectal cancer, endometrial cancer, and ovarian cancer [8, 9, 10, 11, 12].
C-type lectin-like receptor 2 (CLEC-2) is a type II transmembrane protein mainly expressed on platelets, which functions as a platelet-activating receptor for snake venom toxin rhodocytin and endogenous ligand podoplanin [13]. CLEC-2 activates platelets through hemi-ITAM within CLEC-2 [14]. Clustering of CLEC-2 induces tyrosine phosphorylation of hemi-ITAM by the Src family kinases [15]. The podoplanin/CLEC-2 axis promotes an immunosuppressed microenvironment and facilitates tumor cell invasion [16].
However, there are few studies to evaluate soluble CLEC-2 levels in patients with colorectal polyps. Therefore, the purpose of the present study was to investigate soluble CLEC-2 levels in colorectal polyps and CRC.
Methods
Study population
We studied 150 patients with colorectal polyps, 150 CRC patients without metastases, 150 CRC patients with liver metastases, and 150 control subjects at the Harbin Medical University Cancer Hospital between January 2018 and December 2018. None of CRC patients received preoperative chemotherapy or radiotherapy. The exclusion criteria included hematological disorders, hypertension, diabetes mellitus, and medical treatment with statins and acetylic salicylic acid. The control subjects were recruited and they were matched for age, gender, body mass index (BMI), and smoking status. All participants underwent endoscopy procedures. The patients with colorectal polyps or CRC were confirmed by histology. Tissue pathology of colorectal polyps was classified as hyperplastic polyp, sessile serrated adenoma, traditional serrated adenoma, tubular adenoma, and tubulovillous adenoma.
This study was approved by the Institutional Review Board of Harbin Medical University Cancer Hospital. Written informed consent was obtained from all study patients.
Clinical examination and biochemical measurements
Clinical data including smoking status, medical history and medication use were recorded for each subject. Venous blood samples after a 10-hour overnight fasting were collected in all participants. All blood samples were collected before colonoscopy. White blood cell (WBC), haemoglobin, and platelet indices were measured by an autoanalyzer (Sysmex XE-2100, Kobe, Japan). The whole blood samples were collected in EDTA-containing tubes, and were processed within 30 minutes after blood collection. The inter- and intra-assays coefficients of variation (CVs) of all these assays were below 5%.
Blood sampling
A venous blood sample was drawn into tube containing sodium citrate from each participant under fasting conditions prior to any treatment. After centrifugation at 2,500 rpm for 10 minutes, the plasma was stored at
ELISA measurements
CLEC-2 levels were measured in duplicate using commercially available sandwich ELISA kit (Xinle, Shanghai, China, respectively) in accordance with the manufacturer’s instruction. The intra- and inter assay variation were below 8% and 10%, respectively.
Statistical analysis
The descriptive statistics were presented as means
Clinical and laboratory characteristics of the participants
Clinical and laboratory characteristics of the participants
Data are presented as means (SD) or percentage. BMI, body mass index; WBC, white blood cells; CLEC-2, c-type lectin-like receptor 2. One-way ANOVA was used for continuous variables and Chi-square test was used for categorical variables. Categorical variables included gender, smoker, and drinker.
CLEC-2 levels in CRC patients, polyps patients, and control subjects.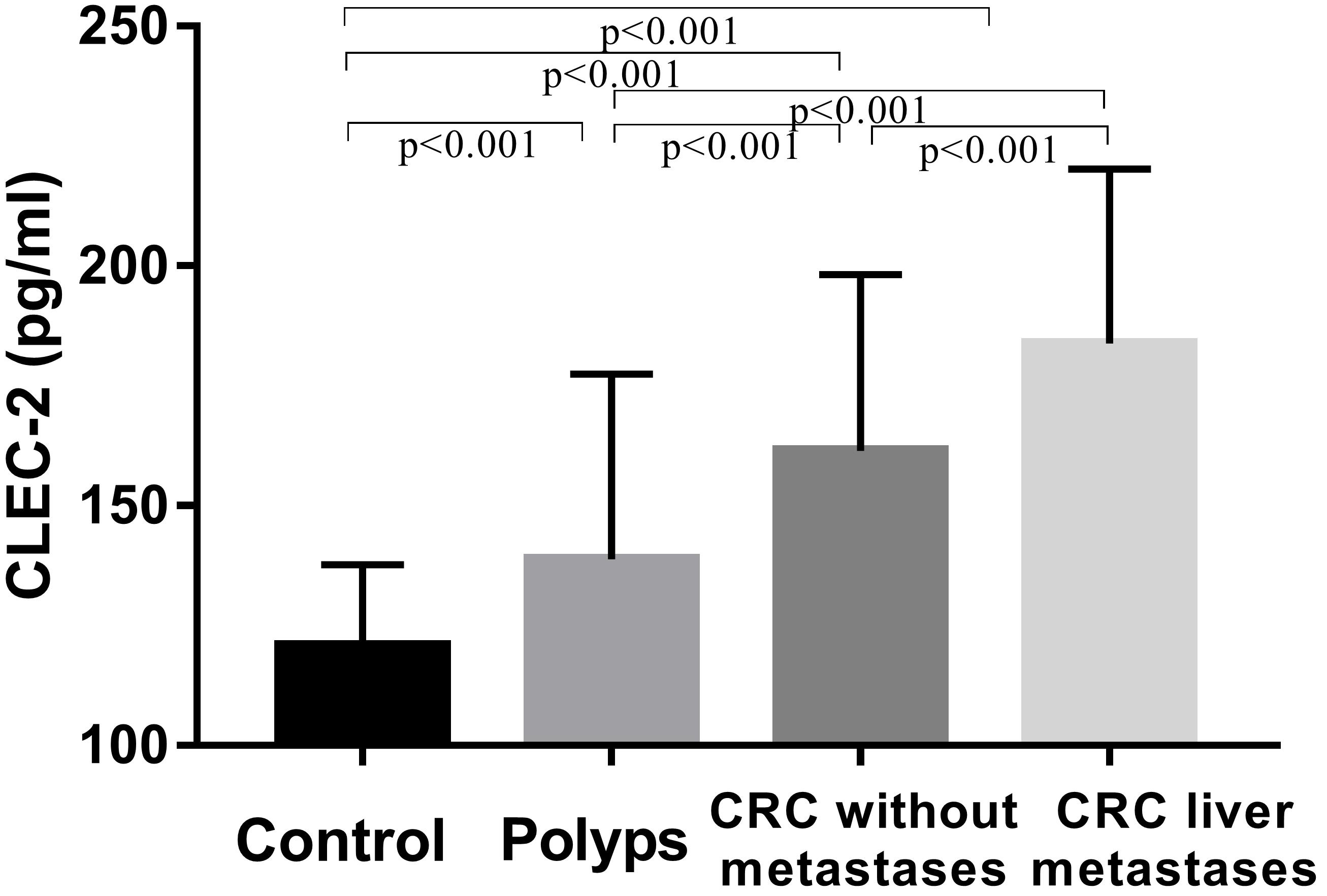
The study included 150 control subjects, 150 patients with benign polyps, 150 CRC patients without metastases, and 150 CRC patients with liver metastases between January 2018 and December 2018. Of the 600 participants entered, 339 (56.5%) were men and 261 (43.5%) were women. The mean ages were 59.8
The characteristics of participants are listed in Table 1. Platelet count, haemoglobin, white blood cells, and CLEC-2 levels were significantly different among four groups. Platelet count, white blood cells, and CLEC-2 levels were markedly increased, and haemoglobin levels were reduced in CRC patients compared with those in patients with benign polyps or in control subjects. However, there was no difference in age, gender, body mass index, smoking status, and drinking status in two groups. Post hoc analyses using two-tailed LSD were conducted for multiple comparisons. The CLEC-2 levels were increased in CRC patients compared to CRC patients with benign polyps or control subjects (Fig. 1). Moreover, CLEC-2 levels were increased in CRC patients with liver metastases compared to CRC patients without metastases.
CLEC-2 levels in benign polyps according to clinicopathological features are presented in Table 2. CLEC-2 levels were not markedly different according to histological grade and tumor size. However, CLEC-2 levels in different types of serrated polyps and conventional adenomas showed significant difference. The CLEC-2 levels were increased both in sessile serrated adenoma and in traditional serrated adenoma, as compared to hyperplastic polyp. Additionally, when compared to hyperplastic polyp, a significant increase in CLEC-2 levels was detected in tubular adenoma and tubulo villous adenoma (Fig. 2).
Correlations between clinicopathological features and CLEC-2 in patients with benign polyps
Correlations between clinicopathological features and CLEC-2 in patients with benign polyps
Values are shown as mean (standard deviation). CLEC-2, c-type lectin-like receptor 2. HGIEN, high-grade intraepithelial neoplasia; LGIEN, low-grade intraepithelial neoplasia; HP, hyperplastic polyp; TSA, traditional serrated adenoma; SSA, sessile serrated adenoma; TA, tubular adenoma; TVA, tubulo villous adenoma.
CLEC-2 levels in different polyps subtypes. CLEC-2: c-type lectin-like receptor 2.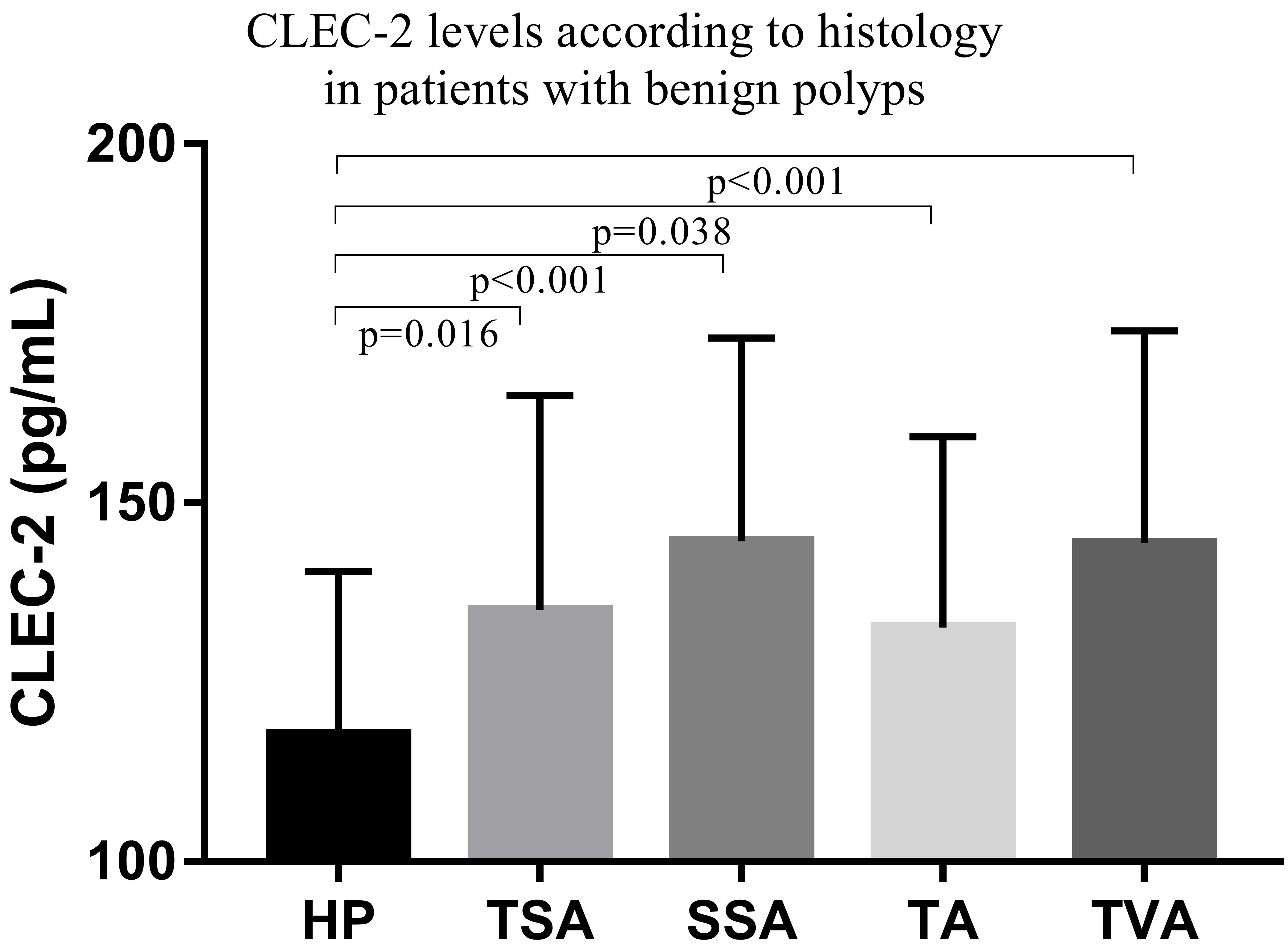
CLEC-2 levels in patients with CRC according to clinicopathological features are summarized in Table 3. However, there was no significant difference in CLEC-2 levels for some clinical and pathological parameters, including tumor size, histological type, histological grade, tumor location, and T classification. CLEC-2 levels were significantly increased in patient with lymph node metastasis and advanced tumor stage, compared with the patients without lymph node metastasis and low stage.
Correlations between clinicopathological features and CLEC-2 in patients with CRC
Values are shown as mean (standard deviation). CLEC-2, c-type lectin-like receptor 2.
Receiver operating characteristic curve analyses
PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve; CLEC-2, c-type lectin-like receptor 2. (A) Analysis of CLEC-2 ROC curve as screening biomarker of colorectal cancer. (B) Analysis of CLEC-2 ROC curve as differentiating biomarker between colorectal cancer and benign polyps.
ROC curve for CLEC-2 as a screening biomarker of CRC.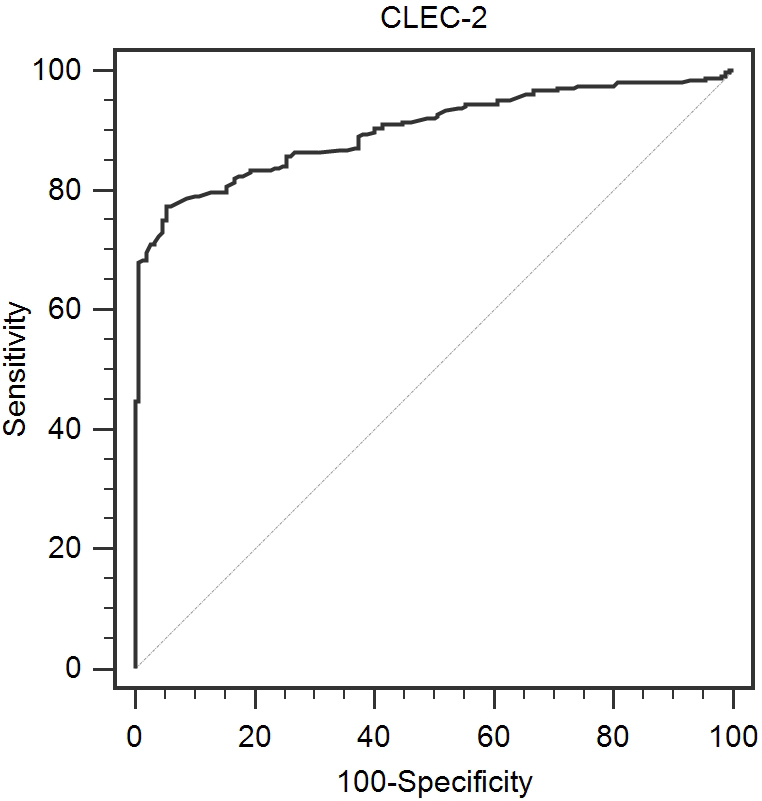
ROC curve for CLEC-2 as a differentiating biomarker between CRC and benign polyps.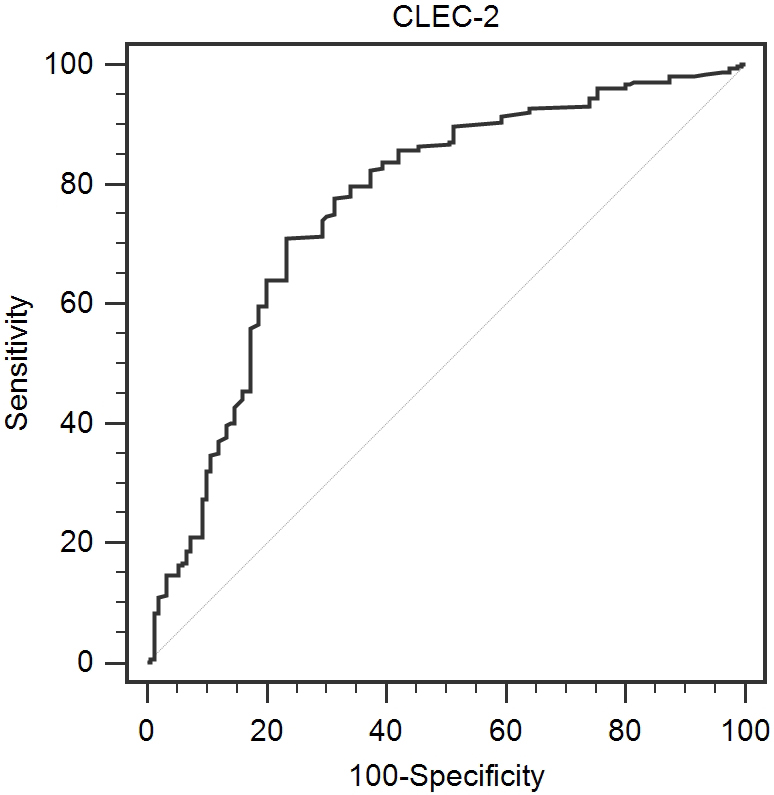
To evaluate whether CLEC-2 can be used as screening biomarker or differentiating biomarker, ROC curve analysis is performed (Table 4). For the screening biomarker of CRC, CLEC-2 yielded an AUC of 0.900 (95% CI: 0.872–0.928) with 77.3% sensitivity and 94.6% specificity (Fig. 3). For the discrimination between patients with CRC and benign polyps, CLEC-2 yielded an AUC of 0.765 (95% CI: 0.716–0.814) with 71.0% sensitivity and 76.7% specificity.
It has been shown that CRC patients had higher soluble CLEC-2 levels than patients with colorectal polyps. Moreover, CRC patients with liver metastases displayed higher CLEC-2 levels than those in CRC patients without metastases. In CRC patients, CLEC-2 levels were correlated with lymph node metastasis and advanced tumor stage. In patients with polyps, there was a significant difference in CLEC-2 levels among different polyp subtypes.
Platelets in tumor microenvironment play a vital role in tumor development, angiogenesis, and metastasis [17]. A growing body of evidence supported the association between platelets activation and CRC [18]. Platelet-derived growth factor-D promotes CRC cell migration, invasion and proliferation [19]. Moreover, higher serum platelet-derived growth factor-AA predicts CRC liver metastasis [20]. In addition, platelet-derived endothelial cell growth factor inhibitor augments radiotherapeutic efficacy for CRC [21]. A previous report confirmed that extract of caulis spatholobi, a platelet inhibitor, efficiently suppresses the invasion and metastasis of CRC by targeting tumor cell-induced platelet aggregation [22]. Furthermore, long-term use of aspirin had a chemo-preventive effect against CRC [23, 24].
The intrinsic mechanisms of CLEC-2 in malignant transformation are not clear. The podoplanin/CLEC-2 axis facilitates tumor cell invasion [16]. Upregulated expression of podoplanin was observed in a number of human tumours, including colorectal adenocarcinoma, lung squamous cell carcinomas, cervical cancer, and oral cancer [25]. Podoplanin interacts with neighbouring cells, extracellular matrix components and stromal factors to promote platelet activation and tumour cell migration [26]. The activated platelets also secrete a variety of bioactive factors that assist in extravasation to new metastatic sites [17]. Clustering of CLEC-2 induces tyrosine phosphorylation of hemi-ITAM by the Src family kinases [15]. Src family kinases are one of the most important signal transmitters in platelets [27]. Recent studies has revealed that transformation by the oncogene Src induces podoplanin expression and promotes tumour cell migration and invasion [28]. Moreover, Src/Syk-dependent signalling stabilises platelet adhesion to podoplanin under flow [29].
In this study, increased CLEC-2 levels were found both in advanced polyp and in metastatic CRC group, indicating that podoplanin signaling is involved in malignant transformation and tumor metastasis. In addition, our results were consistent with previous findings that platelet activation played a key role in malignant transformation of advanced polyp and the aspirin usage was associated with a significant reduction in colorectal adenoma recurrence [30, 31, 32]. Therefore, CLEC-2 could be used as a useful screening indicator in patients with colorectal polyps and as a potential therapeutic target to prevent malignant transformation from colorectal polyps to CRC.
The interpretation of this study had some limitations. Firstly, the study was the lack of a mechanistic explanation. Secondly, the study was carried out in a single center. Fianlly, this findings cannot be generalized because only Chinese patients were included in the present study.
In conclusion, CRC patients have higher CLEC-2 levels than patients with colorectal polyps and healthy controls. Moreover, there is a significant difference in CLEC-2 levels among polyp subtypes. Further research is warranted.
Author contributions
Conception: ML Z, WJ H, RT W, and R X
Interpretation or analysis of data: ML Z, WJ H, CX Y, MM L, N L, RT W, and R X
Preparation of the manuscript: ML Z and WJ H
Revision for important intellectual content: CX Y, MM L, N L, R X, and RT W
Supervision: R X and RT W
Funding
This work was supported by the Fundamental Research Funds for the Provincial Universities (No. 2018-KYYWF-0526).
Footnotes
Conflict of interest
None declared.