
Abstract
BACKGROUND:
Stratification and risk-evaluation of bladder cancer (BCa) patients are far-reached issues, especially for those with non muscle invasive disease. Thus, setting-up biomarkers, especially after resection of the primary tumor, is crucial. Specifically, Neutrophil to lymphocyte ratio NLR and let-7 deregulation which have been preliminarily but not consistently described to be associated to unfavorable prognosis.
OBJECTIVE:
To explore the clinical value of pre-treatment Neutrophil to Lymphocyte Ratio (NLR), let-7c and let-7g’s deregulation.
METHODS:
Data were extracted from ninety BCa samples. Pre-treatment NLR was estimated as the absolute neutrophil count divided by the absolute lymphocyte count. Expression patterns of let-7c and let-7g were assessed by qRT-PCR. Correlation with clinical characteristics was performed by descriptive statistics.
RESULTS:
Both let-7 miRs were upregulated. Interestingly, let-7g was associated to pathological stage (
CONCLUSIONS:
Our data demonstrated the potential clinical value of all markers, especially pretreatment NLR and let-7g. Further studies are recommended to confirm their utility in improving the clinical decision-making regarding treatment and follow-up scheduling.
Introduction
Bladder cancer (BCa) is the ninth most common cancer worldwide with an incidence of approximately 430 000 cases per year, and it ranks 13th in terms of annual mortality from cancer. It is the seventh most common cancer worldwide in men with marked male predominance [1]. The most common histological subtype is Urothelial BCa. Approximately, 75% of patients present with non-muscle-invasive disease (NMIBC), confined to the bladder mucosa/submucosa. This stage is usually managed with local treatment and regular follow-up, and has a particularly high prevalence due to the non aggressive natural history of this disease. The remaining 25% have muscle-invasive disease (MIBC) and often undergo cystectomy, multimodal treatment (transurethral resection, chemotherapy, and radiation therapy), or palliative care [2].
According to the current theories, the systemic inflammatory response triggered by cancer leads to a relative neutrophilia and lymphocytopenia, creating a pro-oncogenic inflammatory condition [3]. An elevated NLR (Neutrophil to lymphocyte ratio) display a high number of neutrophils and a low number of lymphocytes, implying that cell-mediated immunity is impaired and systemic inflammation is increased in inflammatory processes [4]. Among patients with BCa, an elevated NLR (Neutrophil to lymphocyte ratio) was described in literature to be associated with advanced pathologic stage [5], invasiveness and bad prognosis [5, 6]. However, the most reported studies included a heterogeneous group of patients with MIBC and high-risk NMIBC treated with radical cystectomy. Moreover, there are still gaps concerning retrospective data on the association between NLR and disease prognosis in patients with NMIBC, initially treated with transurethral resection of BCa (TURBT).
Several mechanisms were suggested to be involved in the regulation of the inflammatory response. Recently, miRNAs have emerged as key regulators of inflammation. They regulate onset and completion signaling of inflammation. Depending upon their targets mRNAs, miRNAs may either enhance or repress inflammation [7]. Among them was cited the role of let7 family of miRNA as a key modulator of inflammatory response [8]. They can act as anti-inflammatory factors by targeting some pro-inflammatory factors such as IL-13 [9] or IL-6 [10] except for development and tumor suppression or they can have pro-inflammatory direct or indirect effect by targeting some anti-inflammatory factors including respectively IL-10 [11] or NF-
Having undergone several duplications in evolution, the let-7 family is comprised of multiple paralogous genes expressed on different chromosomes forming the largest miRNA family in mammals. There are 12 different let-7 family members (let-7a-1, 7a-2,7a-3, 7b, 7c, 7d, 7e, 7f-1, 7f-2, 7g, 7i, and mir-98) expressed in human [14]. Being members of the same family, it suggests that they have at least some targets and functions in common as they were described to be most involved in multiple biological processes including cell proliferation, differentiation, progression, cell death, migration, chemoresistance and metabolism [15]. The role of let-7 in BCa is still not fully understood and it is was evident that the let-7 family members displayed distinct expression patterns [16]. Among let-7 miR family members, we were interested in the analysis of let-7c and let-7g expression profiles in Tunisian BCa specimens, since they both target inflammatory factors such as IL-10 and IL-6 as validated in several databases such as Target Scan and miRanda.org. In addition, it has been reported that let-7c is a potential biomarker to predict incidence, progression of MIBC and response to neoadjuvant chemotherapy [17]. Moreover the deregulation of let-7g expression has been found to be positively associated with cancer prognosis [18, 19].
In the present, we tried to investigate the conceivable interaction between NLR, as a well described regulator of inflammatory response, and let-7c and let-7g expression, as inflammation-associated candidate miRNAs. Moreover the clinical utility of all markers was formerly highlighted.
Material and methods
Study setting and design
Data were obtained from a retrospective cohort of formalin-fixed paraffin-embedded (FFPE) specimens that were collected from the Pathology and Urology Departments of Charles Nicolle hospital (Tunis, Tunisia) from patients who underwent transurethral resection of the bladder or radical cystectomy in the period between November 2015 and January 2017. A written informed consent form was obtained from each patient and all protocols were approved by the Tunisian Ethics committees of Charles Nicolle’s Hospital.
Patients and samples
All patients were initially treated with a TURBT, with the aim of a complete resection of the bladder tumor. Before the surgery, patients were screened for urinary tract infection and treated with appropriate antibiotics when necessary. All surgical specimens were reviewed by a pathologist and the diagnosis of urothelial carcinoma of the bladder was confirmed.
We analyzed BCa specimens from 90 patients: 44 specimens of HG NMIBC, 23 specimens of LG NMIBC, and 23 specimens of MIBC. Control samples consisted of ten specimens obtained from the non-tumoral area of cystectomy specimens and were confirmed to be non tumoral by the same pathologist. Clinico-pathological features and epidemiological parameters of the studied population including the classical presentation of BCa and the clinical course are detailed in Table 1. The patients in each group of NMIBC were also classified into risk groups according to the European Organization for Research and Treatment of Cancer (EORTC) (Table 2). For each specimen, we measured NLR, let-7c and let-7g expression and correlated them with the clinical and epidemiological characteristics of the patients.
Clinicopathological and epidemiological characteristics of bladder cancer patients
Clinicopathological and epidemiological characteristics of bladder cancer patients
PY: Packet per year; LG NMIBC: Low grade non muscle-invasive bladder cancer; HG NMIBC: High grade non muscle-invasive bladder cancer; MIBC: Muscle-invasive bladder Cancer; Tis: Tumor in situ.
EORTC stratification for progression and recurrence in NMIBC
EORTC: Europeen organisation of research and treatement of cancer; NMIBC: Non muscle-invasive bladder cancer.
The Neutrophil to lymphocyte ratio NLR was calculated based on the neutrophil and lymphocyte count as measured in a complete CBC (Complete Blood Account) taken before treatment (TURBT). It was defined as the absolute neutrophil count divided by the absolute lymphocyte count. Based on the ROC curve, we used a cut-off of 3.279 for the NLR with the most accurate balance between sensitivity (50%) and specificity (76%) (Area under the curve 0.60; 95% confidence interval [CI] 0.51-0.69;
RNA extraction and qRT-PCR
Total RNA derived from FFPE tissues was extracted using the Pure Link™ FFPE Total RNA Isolation Kit (Invitrogen, Waltham, MA, USA) following the manufacturer’s instructions. The quantity and quality of the total isolated RNAs were measured and assessed with a NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific, Wilmington, DE, USA).
To study the expression levels of let-7c and let-7g (hsa-let-7c-5p; hsa-let-7g-5p), a reverse transcription and qRT-PCR amplification were accomplished in two steps. In the reverse transcription step, 25 ng of RNA were used in reactions with specific RT probes for let-7c and let-7g and RNU6 as endogenous control primer using TaqMan™ Reverse Transcription Kit (ThermoFisher, TaqMan™ Reverse Transcription Kit). In the second step, cDNA samples were amplified in Real-Time PCR instrument 7900 (Applied Biosystems, TaqMan™ Reverse Transcription Kit) using TaqMan
Statistical analysis
The data was analyzed by descriptive statistics. A
A Receiver Operating Characteristic (ROC) Curve is an evaluation metrics for checking a classification model’s performance. It is a graphical plot of the true positive rate against the false positive rate that illustrates the diagnostic ability of a binary classifier system as its discrimination threshold is varied. It simultaniously shows the relationship between sensitivity and specificity, the test accuracy (the closer the graph is to the top and left-hand borders, the more accurate the test. Likewise, the closer the graph to the diagonal, the less accurate the test. A perfect test would go straight from zero up the the top-left corner and then straight across the horizontal) and the likelihood ratio which is given by the derivative at any particular “cutpoint”. In this study, receiver operating characteristic (ROC) curves, area under the curve (AUC) of the ROC, sensitivity, specificity, as well as likelihood ratios were calculated to determine levels of miRNAs and NLR that best differentiate bladder cancer groups and subgroups according to TNM stage and histological grade.
AUC-ROC (Area under the ROC curve) represents a degree or a measure of separability. It tells how much a model is capable of distinguishing between classes. Higher the AUC, better the model is at predicting 0 s as 0 s and 1 s as 1 s. By analogy, higher the AUC, better the model is at distinguishing between patients with disease and no disease.
AUC was used for identifying probable classification problems at various thresholds settings and to evaluate the degree of miR deregulation in distinguishing between tumor groups. An excellent model for a good separation was considered when AUC is near to 1. All analyses were performed using SPSS software (SPSS, version 23.0, USA).
Results
Neutrophil to lymphocyte ratio’s (NLR) significance among BCa patients
NLR was compared between BCa subgroups (LG NMIBC, HG NMIBC, MIBC). The distribution of this ratio among the tumor groups was significantly heterogeneous (
NLR, let-7c and let-7g’s value in terms of association to BCa subgroups, TNM stage and histological grade
NLR, let-7c and let-7g’s value in terms of association to BCa subgroups, TNM stage and histological grade
NLR: neutrophil to lymphocyte ratio; BCa: Bladder Cancer; TNM: tumor, node, and metastases; NMIBC: non muscle invasive bladder cancer; LG NMIBC: Low grade non muscle invasive bladder cancer; HG NMIBC: High grade non muscle invasive bladder cancer; MIBC: muscle invasive bladder cancer; *
Neutrophil to lymphocyte ratio and correlation to tumor subgroups NLR vs Tumor subgroups (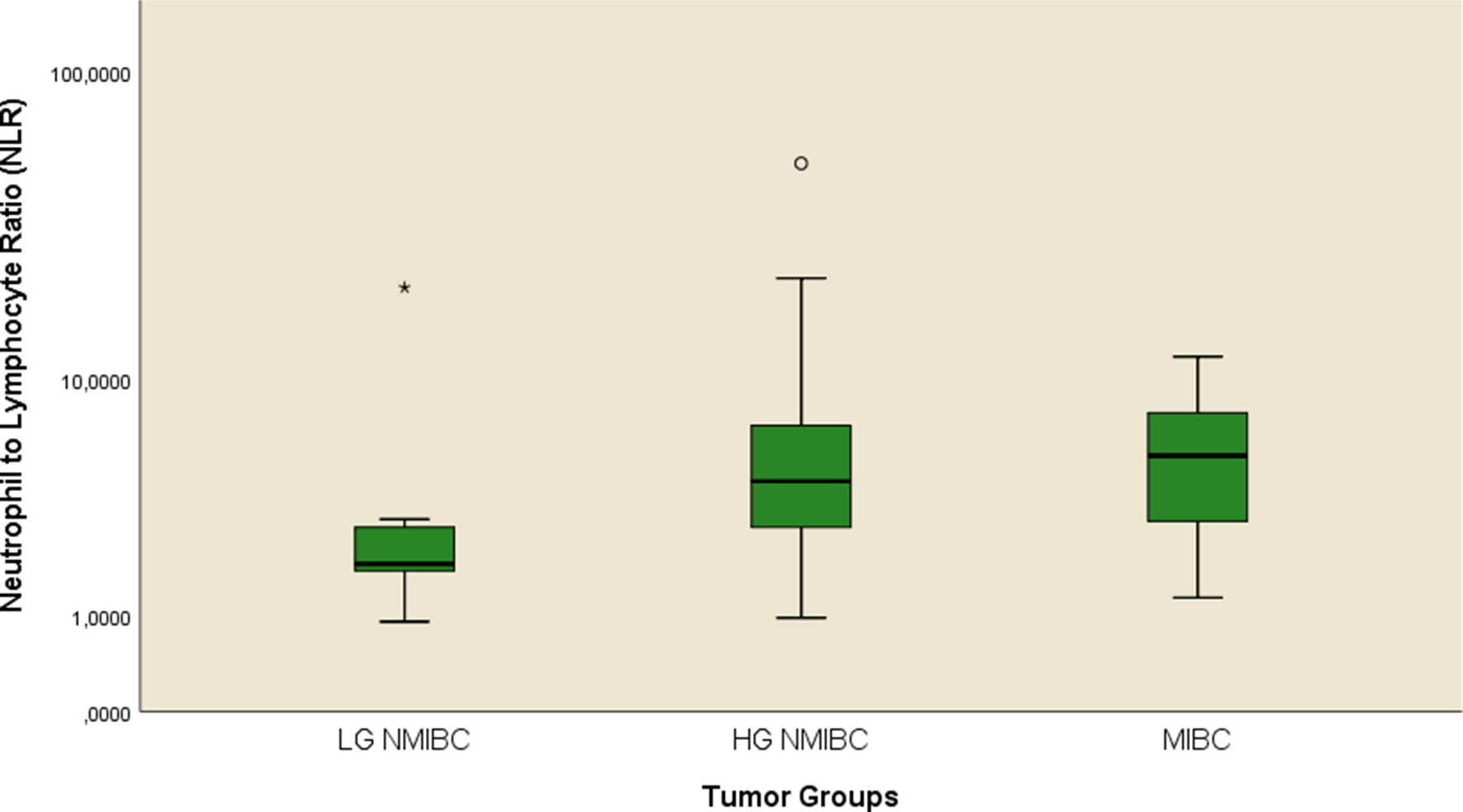
Clinical and pathological characteristics of patients with NMIBC were stratified by the NLR cut off point and are reported in Table 4. When NLR was analyzed as a continuous variable, we found that both groups exhibited significant differences in term of pathological grade (
Patients with NMIBC and tumor characteristics stratified by neutrophil-to-lymphocyte ratio (NLR)
NLR: neutrophil to lymphocyte ratio; BCa: Bladder cancer; NMIBC: non muscle invasive bladder cancer; LG NMIBC: Low grade non muscle invasive bladder cancer; HG NMIBC: High grade non muscle invasive bladder cancer; MIBC: muscle invasive bladder cancer; PY:package per year; EORTC: Europeen Organisation of Research and Treatement of Cancer; *
Expression distribution of hsa-let-7c and hsa-let-7g according to clinical parameters
EORTC: Europeen organisation of research and treatement of cancer; *
ROC analysis for NLR expression in NMIBC. ROC: Receiver operating characteristic; NLR: Neutrophil to Lymphocyte ratio; NMIBC: Non Muscle-Invasive Bladder Cancer; The 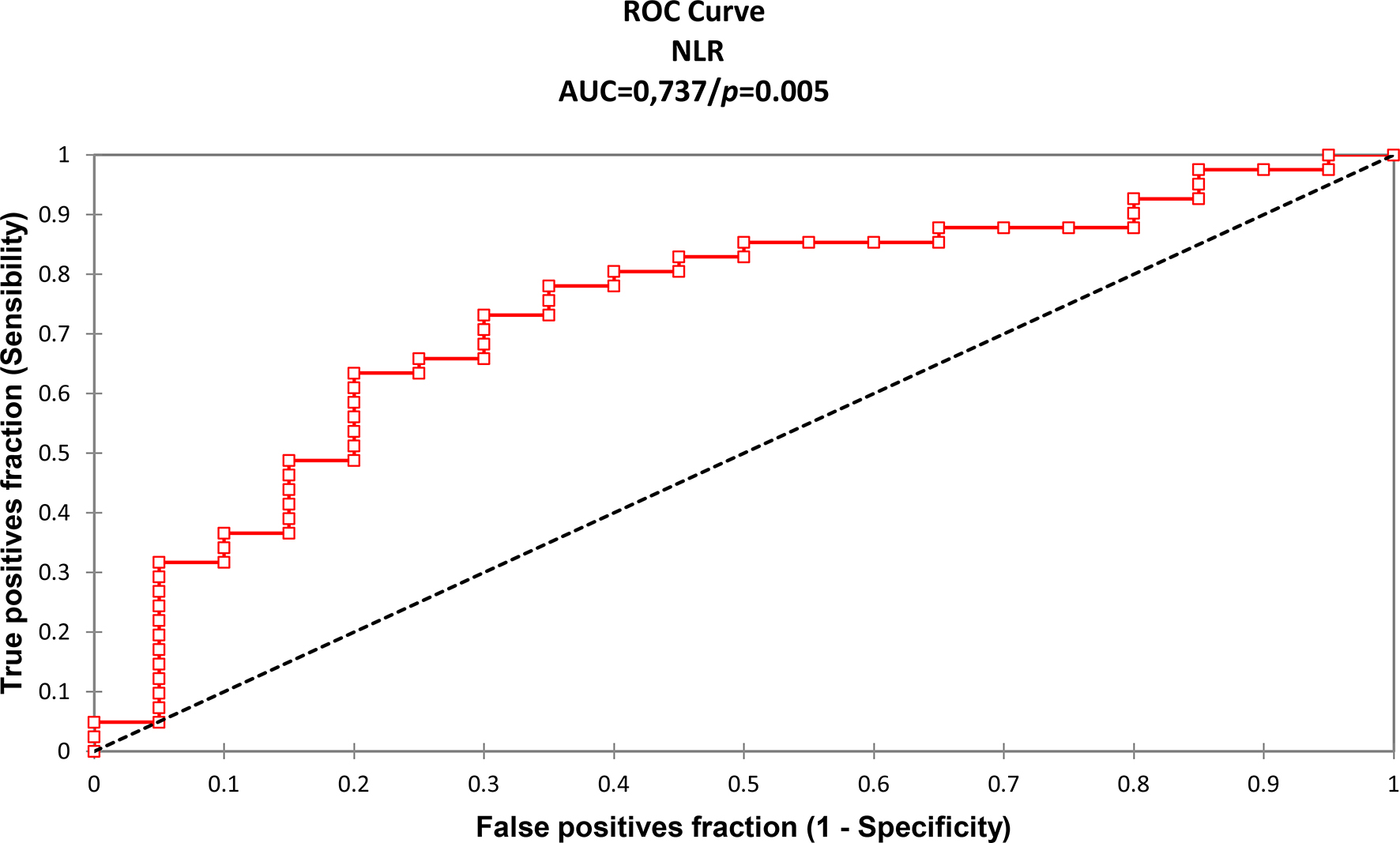
Compared with non tumoral samples, let-7c and let-7g were significantly upregulated in BCa samples with a mean fold change (FC) estimated respectively at 9.92 (sd
Expression patterns of let-7c and let-7g. *Expression patterns of let-7c and let-7g among BCa patients and non tumoral controls *a: Let-7c in tumor subgroups versus controls (mean FC 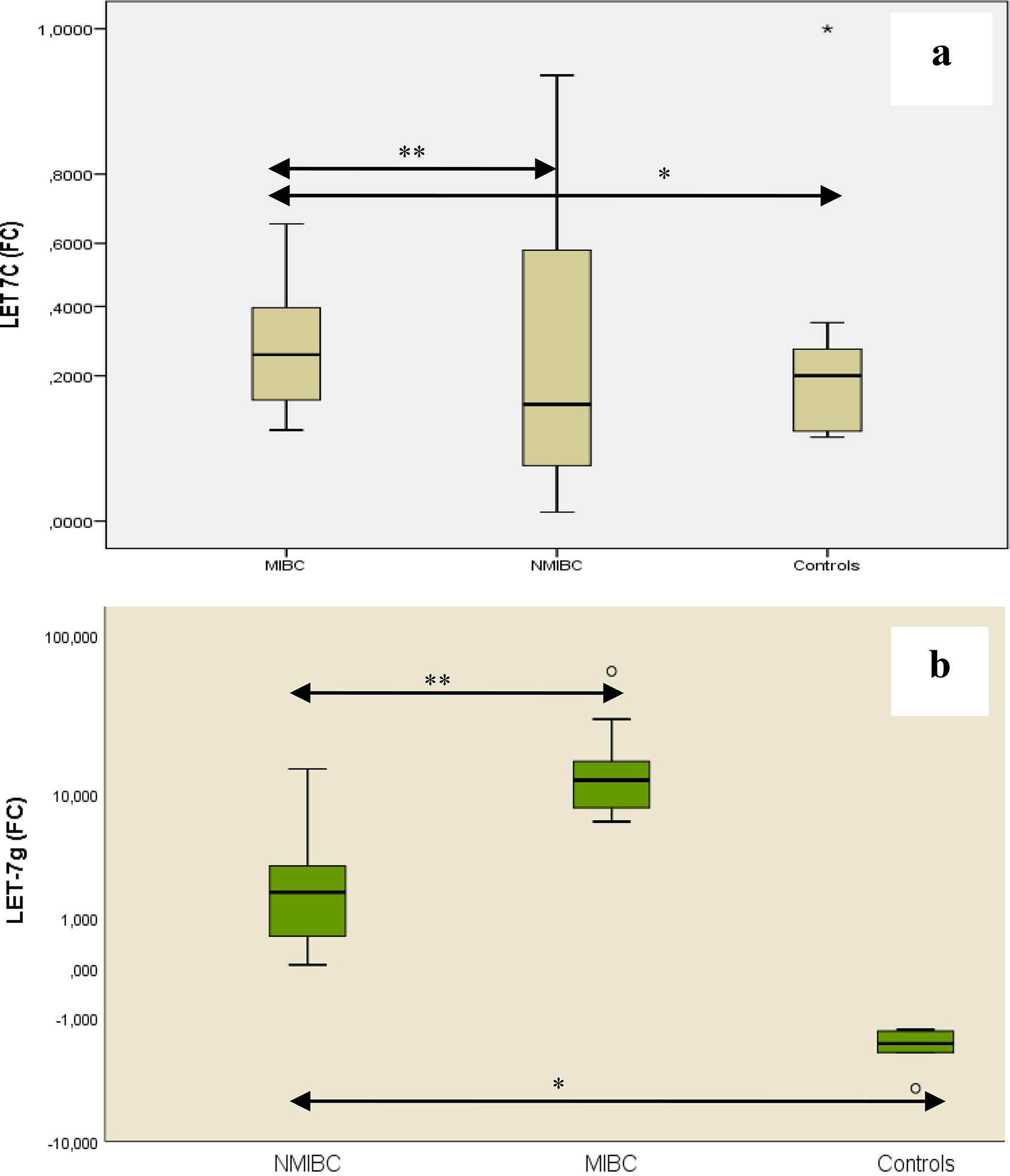
Expression patterns of let-7c and let-7g and correlation to tumor subgroups. a: Let-7c vs Tumor subgroups (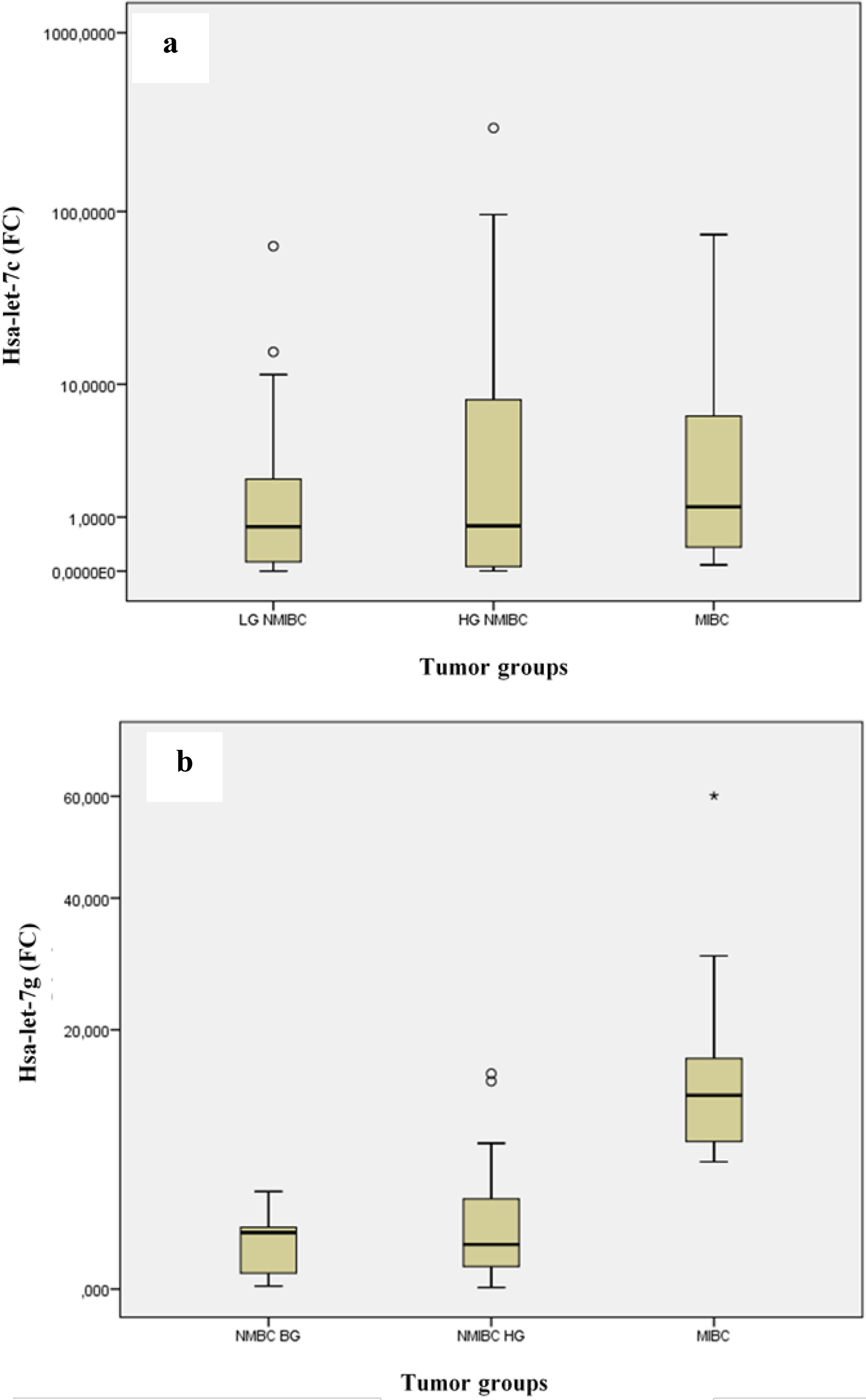
Formerly, the alliance between the deregulation of let-7c and let-7g and clinicopathological parameters revealed that the increased expression of let-7g was significantly associated to the number of tumor foci and that it was higher in tumor groups with a number of sites greater or equal to 2 (Table 5). However no association was noted between let-7c and clinical prognosticators. On the other hand, the distribution of the expression patterns of let-7c or let-7g between the risk groups of progression or recurrence in patients with NMIBC was homogenous (
The correlation between both miRNAs expression levels and the corresponding pre TURBT NLR was performed by the mean of a bivariate correlation (Table 6) and a regression logistic analysis (Table 7). Unfortunately, no significant correlation was observed (
Correlation matrix between NLR, let-7c and let-7g in the NMIBC patients
Correlation matrix between NLR, let-7c and let-7g in the NMIBC patients
NLR: neutrophil to lymphocyte ratio; NMIBC: non muscle invasive bladder cancer; FC: Fold Change; *
Logistic regression model combining NLR, let-7c and let-7g
ROC analysis for let-7g expression in MIBC (reference group NMIBC). (ROC: Receiver operating characteristic; NMIBC: Non muscle-invasive bladder cancer; MIBC: Muscle-invasive bladder cancer; The 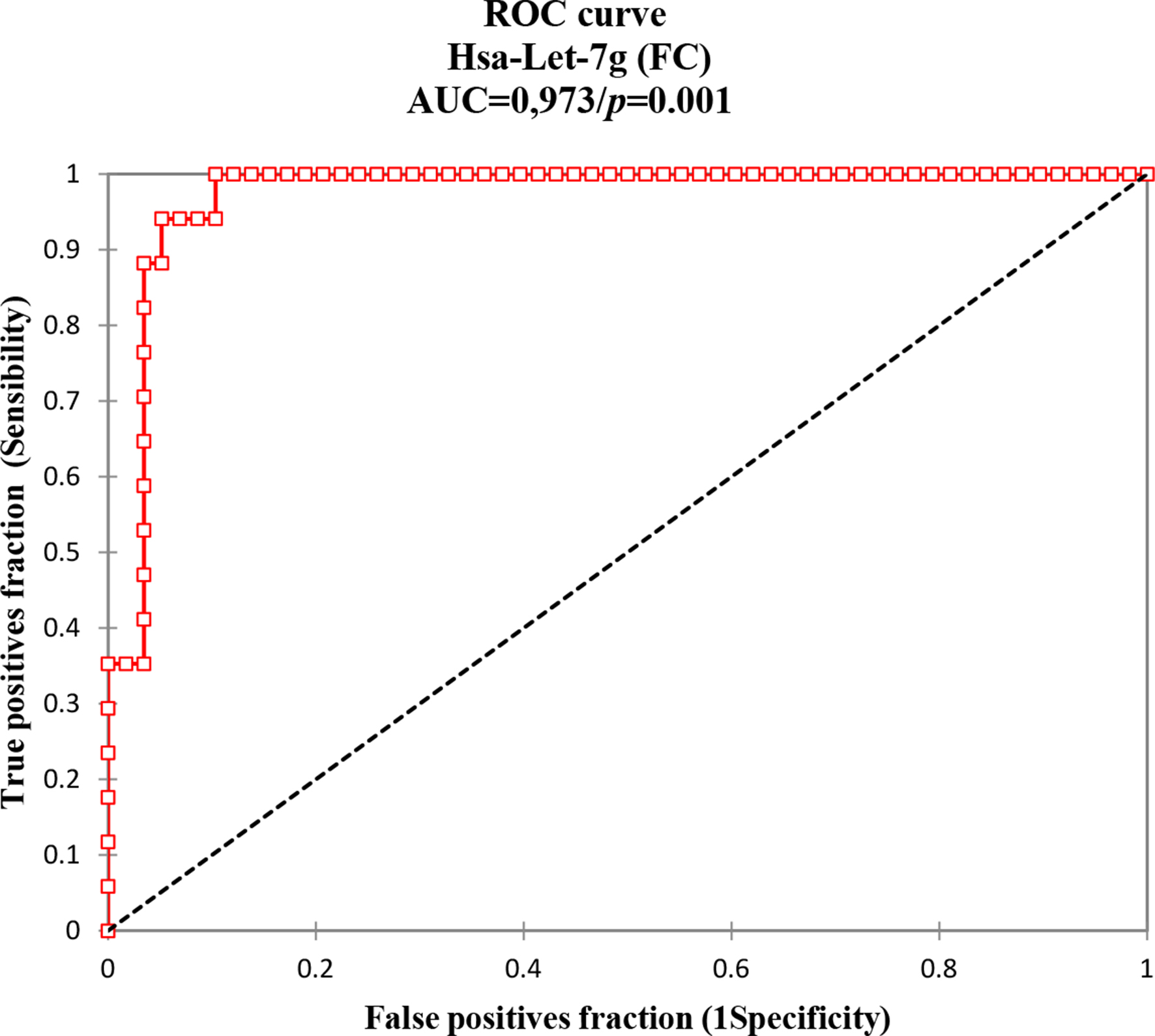
Non-muscle invasive bladder cancer (NMIBC) represents a heterogeneous group of tumors with different rates of recurrence and progression. The individualization of adjuvant therapy’s for each risk group especially in doubtful cases (intermediate or high risk for recurrence or progression) is critical and needs the development of independent pretreatment predictors of outcome.
Multiple research works reported that a systemic inflammation is conjoined to the development and progression of several neoplasms [20, 21]. Among prognostic inflammation markers, the pretreatment neutrophil-to-lymphocyte ratio (NLR), a simply-measured and reproducible biomarker, is the most widely studied one. Baseline NLR in healthy subjects demonstrated in recent studies was between 1.50 and 1.65 [22, 23] which is lower than baseline NLR in the NMIBC patients witnessing the eventual occurrence of an inflammatory tumoral microenvironment. Thus, when investigating its clinical value among patients undergoing TURBT for NMIBC, a significant discrimination between HG NMIBC and LG NMIBC tumors was highlighted. The most increased values were among the high grade tumors. The discriminative value of this biomarker was further confirmed by Roc curves.
This result was in concordance with other data from other populations [24, 25] underlying the importance of relying on this marker especially concerning its efficiency in extricating high grade tumors from low grade ones which could be valuable for the anatomopathologists especially due to the heterogeneity of the HGNMIBC. The association of the NLR to pathological characteristics in NMIBC such as sex, age, tumor category, size and multiplicity, was not conclusive. Although others data have reported a significant association to tumor size [26, 27].
Divergence may result from many other factors, such as age distribution, gender, or lifestyle and so on. Further, as fewly described to be associated to recurrence and progression in NMIBC tumors [25, 27] but rarely correlated to EORTC progression and relapse scores, our explorative data concerning the correlation to EORTC scores showed that there wasn’t a significant association. We conclude that this result could be due to the fact that NLR alterations may depend of tumor inflammatory microenvironment [28], thus, despite the fact that the p value was very close to significance, we couldn’t conclude to a significant result. We believe that given a larger cohort per sub-group, a statistical significance is probable. In literature, conflicting results were reported [29, 28] and our results displayed a contradictory result given by [24].
Besides, we have demonstrated that the pre TURBT NLR was associated to pathological stage in BCa patients (Table 3) where the highest levels of this ratio were observed among MIBC suggesting a potential role in invasiveness.
In addition to NLR, miRNAs are currently emerging as key regulator of inflammation. There are evidences showing that the biogenesis of miRNAs is regulated as part of the inflammatory response by altering the transcription processing or stabilization of mature or precursor mRNA transcripts [30, 31]. Here in, we have shown that altered miRNA expression occurs commonly in Bca, in a phenotype-specific manner. It is noteworthy that we have focused on two members of the let-7 miRNA family which are abundantly expressed in BCa and tried to elucidate their expression profile and prognosis significance in Tunisian patients with urinary BCa.
At the first level, we have performed the investigation of the expression profile of let-7c and let-7g among patients with BCa in order to evaluate postliminary their usefulness for diagnosis and prognosis. Both of our tumor-associated miRNAs were downregulated in the normal urothelium in comparison with patients with the disease. These results underline their potential usefulness as a diagnosis tool.
Publications bias exists concerning the up regulation of these markers. Indeed, the over-expression of let-7c in our cohort is in agreement along with recent reports indicating that this miR is up regulated in high grade T1–T4 BCa Tumors [32]. However, contradictory results where let-7c was up regulated in non tumoral samples have been reported [33, 34]. This result may be explained by the complex nature of the regulating mechanisms of this miRNA family and that different let-7 miRs are regulated by different factors in a specific manner and under different mechanisms of control [8]. On its side, the deregulation of let-7g in BCa has not been yet well elucidated. Its up-regulation in FFPE BCa tissues is in agreement with a previous study performed on NMIBC patients [35]. To our knowledge, this is the second study to investigate the expression of let-7g in BCa in literature. This fact accentuates the need to enlarge the studies on this marker in other cohorts. Besides, other data concerning its deregulation in other neoplasms have been reported [36, 37].
Secondly, in order to better understand the clinical involvement of increased let-7c and let-7g expression in BCa, both miRNA’s were correlated to clinical stage and pathological grade. Intersetingly, let-7g was proven to be associated to TNM stage. Its expression patterns displayed the highest levels among the most aggressive group of BCa indicating a possible role in aggressiveness or invasiveness. This hypothesis needs to be confirmed by functional analysis on a larger MIBC cohort. When correlated to other clinicopathological features, the high levels of let-7g were associated to highest numbers of tumor foci indicating that these increased patterns lean towards a bad prognosis which is in agreement with previous speculating in other neoplasms [38, 39]. Nevertheless, the association to progression and recurrence EORTC scores was insignificant. This result could be explained by the retrospective nature of the study and the relatively limited sample size.
To date, no data in literature were available in this context and our study is the first one to evoke these associations to pathological stage, histological grade and clinical prognosticators in BCa samples.
No association was found between the over expression of let-7c and clinicopathological prognosticators. This result could be explained by the retrospective nature of the study, the limited sample size as said previously, or by the fact that this miRNA interfere most in BCa tumorgenesis enrollment rather than prognosis.
Considering the important role of the let-7 family members in the inflammatory response as ranked among miRNA regulators of the key inflammatory pathways [8], we tried in a descriptive manner to explore the probable role of let-7c and let-7g as inflammation-associated miRNAs by correlating both expression patterns to the pretreatment NLR. Unfortunately, no association was found between the let-7 miRNAs and NLR not only in NMIBC but also in our entire cohort.
Hypothetically, this could be explained by the nature of the retrospective cohort or to the fact that let-7 may act in some conditions as an anti-inflammatory mediator by targeting IL-6 and suppressing NF-
Conclusion
Our data revealed the clinical relevance of NLR, let-7c and let-7g as potential pronosticators. Detecting these miRs in biofluids, in addition to blood NLR, could be of a major importance in tumor diagnosis and cancer estimating prognosis since they are easy obtained, cost-effective and non invasive reliable tools. Besides, due to the raising concern about the usefulness of let-7 miRs as therapeutic targets motivates this interest. Nevertheless, these data should be confirmed by advanced functional analyzes on larger cohorts.
Footnotes
Acknowledgments
This work is dedicated to the pure soul of our friend, clinician and scientist, Dr ATI Nidhal, Urology department, Charles Nicolle hospital, Tunis. RIP. I would like to thank S.O for supervising the research; G.P for allowing me to perform experiments in her honorable laboratory; S.O and G.P for the conception, design of the study and the revision of the paper, A.G and I.M for providing essential experimental knowledge; N.T, R.S and S.O for assisting the analyze and interpretation of data, S.O for the setting of the statistical analysis; H.A and O.K for revising the paper and helping with the clinical part; H.A,M.K, O.K, A.S, M.A.E, A.B, S.R.R and M.C for providing clinical samples, allowing access to clinical files of the patients and confirming the histopathological characteristics of the studied specimens. Respect and gratefulness to my family’s sacrifices and devotion.
Conflict of interest
The authors declare there are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.