CD133 is the molecular marker of normal stem cells and progenitor cells and also confirmed as a marker for cancer stem cells in various tumors. The aim of this study is to examine the expression of CD133 and assess its clinicopathologic significance in benign and malignant breast lesions.
METHODS:
We analyzed the distribution of CD133 positive cells in breast usual ductal hyperplasia, atypical ductal hyperplasia (ADH), breast ductal carcinoma in situ (DCIS), and invasive breast carcinomas. We then explored the relationship between the CD133 expression and clinicopathologic features using immuno-histochemical staining.
RESULTS:
We found that CD133 is not expressed in the cells of normal breast tissue, but the expression rate increased with progression of lesions from usual hyperplasia, through atypical ductal hyperplasia, ductal carcinoma in situ and invasive carcinoma. The positive expression rate of CD133 in breast invasive ductal carcinoma correlated to histological grade, cancer stage, nodal status, metastasis, recurrence, event-free survival and overall survival. There was no significant correlation between CD133 expression and factors such as age, postmenopausal status, histological type, tumor size, estrogen receptor, progesterone receptor and human epidermal growth factor receptor-2 expression.
CONCLUSION:
CD133 may play an important role in the occurrence and development of breast cancer. CD133 positive breast cancer cells are closely related to invasiveness and its expression may predict a poor prognosis.
Breast cancer is the most common malignant tumor, accounting for 23% of all cancer cases and causing 14% of all cancer deaths in women [1, 2]. Until now, the pathogenesis and malignant progression of breast cancer have not been fully elucidated, so it is difficult to establish effective preventive measures. In addition, the prognosis of breast cancer patients is still unsatisfactory. As a result, it is critical to seek new targets to study the occurrence, progression and prognosis of breast cancer.
A small subpopulation of cells in the tumor tissue, with stem cell-like characters, is called as cancer stem cells (CSCs). They have the characteristics of self-renewal, differentiation potential, high tumorigenicity, unlimited proliferation, and resistance to radiotherapy and chemotherapy. They are also considered to play a key role in the process of cancer relapse and metastasis [3]. Al-Hajj isolated firstly CD44/CD24 breast cancer stem cells from breast cancer tissues, which confirmed as surface molecular markers on breast cancer stem cells in 2003 [4]. However, a further study has indicated that, CD44/CD24 breast cancer cells are heterogeneous and can be further divided into different subgroups. Cells in some subgroup have no capacity of tumor formation, suggesting that not all cells labeled with this molecule are breast cancer stem cells [5]. Therefore, it is necessary to screen out other stem cell markers or jointly utilize multiple stem cell markers for studies on breast cancer stem cells.
CD133 is the molecular marker of normal stem cells and progenitor cells, also confirmed as a marker for CSCs in various tumors [6, 7, 8, 9, 10, 11, 12]. Some studies have also demonstrated that CD133 is one of the markers of breast cancer stem cells [13, 14]. Multiple clinical studies have confirmed that CD133 may have potential predictive effect and is an effective tool for the treatment of invasive breast cancer [15, 16, 17]. Lin’s research indicated differential CD133 expression distinguishes between benign lesions and malignant breast papillary lesions [18].
However, breast carcinogenesis is thought to undergo a transition from normal epithelium to invasive carcinoma through usual ductal hyperplasia, atypical ductal hyperplasia, and breast ductal carcinoma in situ [19]. It has been confirmed by original biopsy that 50% of untreated breast carcinoma in situ will develop into invasive breast carcinomas within 24 years [19, 20]. Therefore, we detected the CD133 expression in normal breast tissues, breast usual ductal hyperplasia, atypical ductal hyperplasia, breast carcinoma in situ and invasive breast carcinoma to gain more insight into CD133’s role in breast carcinogenesis in this study. In addition, we further researched the relationship between CD133 expression and clinicopathologic characteristics in invasive breast carcinomas to evaluate the significance of CD133 in breast cancer progression and prognosis.
Methods and materials
Tissue samples
In this study, archived paraffin section specimens (mean age 51.37 yearsaged 27 to 78) from January 2006 to December 2008 were selected from the department of pathology, kunming general hospital. All samples were confirmed independently by two pathologist examinations. The study of tissue samples was approved by the Ethics Review Committee of Kunming General Hospital. All procedures followed Institutional Review Board (IRB) approved protocol. These specimens included 41 cases of usual ductal hyperplasia, 39 cases of atypical ductal hyperplasia, 51 cases of ductal carcinomas in situ, 121 cases of invasive breast cancer (97 cases of invasive ductal carcinoma, 17 cases of invasive lobular carcinoma and 7 cases of other types) and 45 cases of normal breast tissues (tissues 5 cm away from breast cancer were collected, and confirmed as normal breast tissues by pathological examination). No radiotherapy, chemotherapy or endocrine therapy was performed before operation to any patient.
Breast cancer tissues were graded according to Elston and Ellis methods. TNM stage was judged by using TNM staging criteria modified in 1998 by Union for International Cancer Control (UICC).
Immunohistochemistry
All of tissue paraffin blocks were cut into 4 m sections. The sections were deparaffinized in xylene, rehydrated using serial dilutions of ethanol and washed three times in 0.1 M PBS for 5 min each time. Antigen retrieval was performed for 2 min at 120C in citrate buffer (10 mmol/l, pH 6.0) in a pressure cooker. After that, the sections were then washed three times in 0.1 M PBS for 5 min each time. Then the sections were incubated in 0.2% hydrogen peroxide for 20 min at room temperature to block the action of any endogenous peroxidase. The following is a further three times 5 min washes in 0.1 M PBS. Then normal goat serum was added for 20 min at 37C prior to incubation overnight at 4C with CD133 mouse anti-human monoclonal antibody (Abcam, dilution 1:200). Afterwards, the sections treated as described above were flushed with PBS for 3 times 5 min, labeled with secondary antibody by biotin at 37C and incubated for 5 min, then again flushed with PBS for 3 times 5 min, incubated at room temperature with peroxidase for 5 min, developed color with diaminobenzidine (DAB), conterstained with hematoxylin, dehydrated, hyalinized, and sealed with neutral gum. Result of immunohistochemical staining with PBS replaced by the primary antibody was adopted as negative control, and positive section with primary antibody was adopted as positive control.
Comparison of the positive rates of CD133 between benign and malignant lesions of the breast
Groups
Cases ()
CD133 expression (%)
Negtive
Positive
Breast usual ductal hyperplasia
41
28 (68.3)
13 (31.7)
0.000
Breast atypical ductal hyperplasia
39
20 (51.3)
19 (48.7)
Breast ductal carcinomas in situ
51
18 (35.3)
33 (64.7)
Invasive breast carcinomas
121
31 (25.6)
90 (74.4)
The expression of CD133 in the diffirent stage of breast carcinogenesis
Groups
Cases ()
CD133 expression (%)
Breast usual ductal hyperplasia
41
28 (68.3)
11 (26.8)
2 (4.9)
0 (0)
0.000
Breast atypical ductal hyperplasia
39
20 (51.3)
5 (12.8)
14 (35.9)
0 (0)
Breasrt ductal carcinomas in situ
51
18 (35.3)
11 (21.6)
16 (31.4)
6 (11.8)
Invasive breast carcinomas
121
31 (25.6)
23 (19.0)
26 (21.5)
41 (33.9)
Microscopic examination
Each immunohistochemistry section was observed independently by two pathologists from the Department of Pathology at Kunming General Hospital under a light microscope (Olympus DX40). CD133 positive staining was manifested as brown yellow or brown granules around the nucleus and cytoplasm. Semi quantitative grading standards were adopted for staining scoring: 0 point, positive cell 10%; 1 point, 10%–25%; 2 points, 26%–40%; 3 points, 41%–55%; 4 points, 56%–70%; 5 points, 71%–85%; 6 points, 86%–100%. Straining intensity: 0 point, negative; 1 point, weak positive; 2 points, moderate positive; 3 points, strongly positive. Comprehensive score was calculated by adding the two scores, 0 point, (); 1–3 points, (), low expression cases; 4–6 points, (), moderate expression cases; 7–9 points, (), high expression cases.
Statistical analysis
Statistical analysis was performed using SPSS 11.5 (Inc., Chicago, IL, USA). The differences were analyzed by chi-squared test and the rank sum test. The Kaplan-Meier method was used to estimate disease-free survival (DFS) and overall survival (OS). A value of 0.05 was considered statistically significant.
Results
Expressions of CD133 in breast benign and malignant lesions
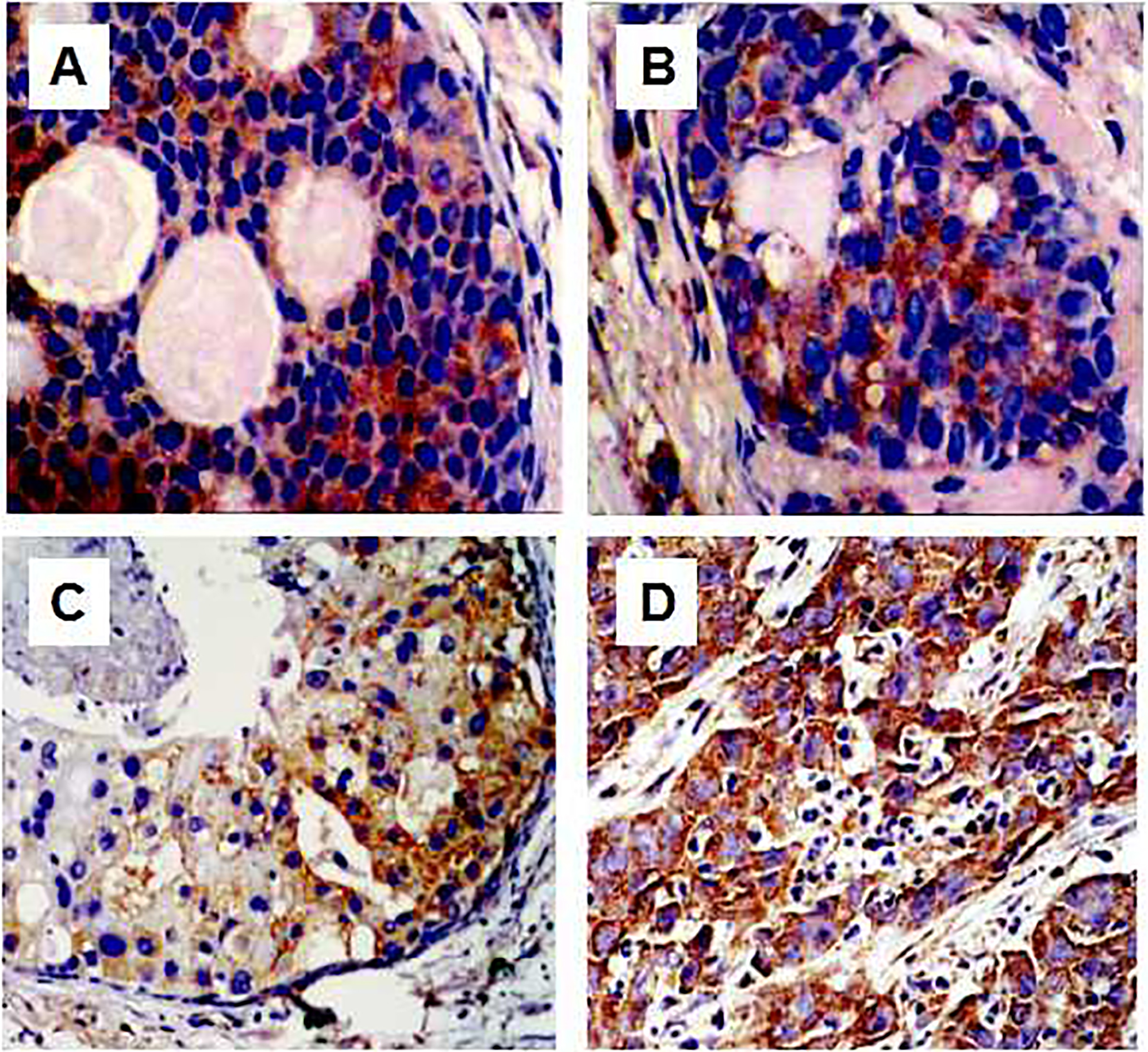
We found that CD133 was not expressed in normal breast tissues. CD133 was expressed in usual breast ductal hyperplasia, atypical breast ductal hyperplasia, breast ductal carcinomas in situ and invasive breast carcinomas tissues (Fig. 1). However, the positive expression rates of CD133 in the above different lesions were different, which were 31.7% (13/41), 48.7% (19/39), 64.7% (33/51) and 74.4% (90/121), respectively. The chi-square test results had statistical significance ( 0.000) (Table 1). To further analyze the correlation between CD133 expression and disease severity, comprehensive score was used in this study to divide CD133 expression level into 4 grades (, , , ), and then ordinal variables of multiple groups were compared by rank sum test. The results showed a significant difference in positive CD133 expression (grades) in benign and malignant diseases of breast ( 0.001) (Table 2).
CD133 expression in breast cancer of various stages. A. Usual breast hyperplasia; B. Atypical breast hyperplasia; C. Breast carcinomas in situ; D. Invasive breast carcinomas.
Correlation between CD133 expression in invasive breast carcinomas and clinicopathological characters
Positive expression rates of CD133 were respectively 63.6% (21/33), 72.2% (26/36) and 82.7% (43/52) in tissues of histological grade I, II and III breast cancer ( 0.05). Positive expression rate of CD133 in tissues of stage IV breast cancer was 94.3% (33/35), obviously higher than 57.1% (12/21) of stage I breast cancer, 69.4% (34/49) of stage II breast cancer and 68.7% (11/16) of stage III breast cancer ( 0.001). Positive expression rate of CD133 was 82.0% (41/50) in breast cancer with lymphatic metastasis. In breast cancer without lymphatic metastasis positive expression rate of CD133 was 69.0% (49/71) ( 0.05). Positive expression rate of CD133 was 94.3% (33/35) in breast cancer with remote metastasis, obviously higher than 66.3% (57/86) in breast cancer without remote metastasis, and the difference was significant ( 0.001). Positive expression rate of CD133 was 82.8% (53/64) in patients with relapsed breast carcinomas. In patients without relapse positive expression rate of CD133 was 64.9% (37/57) ( 0.05). Positive expression rate of CD133 was not significantly correlated with patient age, menstrual state, histological type of tumor, tumor size, or expressions of estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor-2 (Her-2) ( 0.05) (Table 3).
Relationship between the expression of CD133 in invasive breast carcinoma and clinicopathological features
Parameter
Cases
CD133 expression (%)
Age
50
65
14
(21.5)
10
(15.4)
19
(29.2)
22
(33.8)
0.122
50
56
17
(30.4)
13
(23.2)
7
(12.5)
19
(33.9)
Menstrual status
Premenopausal
69
14
(20.3)
12
(17.4)
17
(24.6)
26
(37.7)
0.089
Postmenopausal
52
17
(32.7)
11
(21.2)
9
(17.3)
15
(28.8)
Histological type
Invasive ductal carcinoma
97
27
(27.8)
17
(17.5)
16
(16.5)
37
(38.1)
0.741
Invasive lobular carcinoma
17
3
(17.6)
5
(29.4)
6
(35.3)
3
(17.6)
Other types
7
2
(28.6)
2
(28.6)
2
(28.6)
1
(14.3)
Histological grade
Grade I
33
12
(36.4)
8
(24.2)
6
(18.2)
7
(21.2)
0.013
Grade II
36
10
(27.8)
7
(19.4)
6
(16.7)
13
(36.1)
Grade III
52
9
(17.3)
8
(15.4)
14
(26.9)
21
(40.4)
Stage
Stage I
21
9
(42.9)
6
(28.6)
4
(19.0)
2
(9.5)
0.000
Stage II
49
15
(30.6)
13
(26.5)
6
(12.2)
15
(30.6)
Stage III
16
5
(31.3)
2
(12.5)
4
(25.0)
5
(31.3)
Stage IV
35
2
(5.7)
2
(5.7)
12
(34.3)
19
(54.3)
Tumor size
2 cm
33
11
(33.3)
6
(18.2)
8
(24.2)
8
(24.2)
0.155
2–5 cm
73
17
(23.3)
15
(20.5)
14
(19.2)
27
(37.0)
5 cm
15
3
(20.0)
2
(13.3)
4
(26.7)
6
(40.0)
Node metastasis
Negative
71
22
(31.0)
17
(23.9)
11
(15.5)
21
(29.6)
0.029
Positive
50
9
(18.0)
6
(12.0)
15
(30.0)
20
(40.0)
Blood metastasis
M0
86
29
(33.7)
21
(24.4)
15
(17.4)
21
(24.4)
0.000
M1
35
2
(5.7)
2
(5.7)
11
(31.4)
20
(57.1)
Recurrence
No
57
20
(35.1)
13
(22.8)
8
(14.0)
16
(28.1)
0.013
Yes
64
11
(17.2)
10
(15.6)
18
(28.1)
25
(39.1)
ER
Negtive
54
11
(20.4)
11
(20.4)
9
(16.7)
23
(42.6)
0.141
Positive
67
20
(29.9)
12
(17.9)
17
(25.4)
18
(26.9)
PR
Negtive
60
16
(26.7)
12
(20.0)
9
(15.0)
23
(38.3)
0.901
Positive
61
15
(24.6)
11
(18.0)
17
(27.9)
18
(29.5)
Her-2
Negtive
45
9
(20.0)
13
(28.9)
11
(24.4)
12
(26.7)
0.679
Positive
76
22
(28.9)
10
(13.2)
15
(19.7)
29
(38.2)
Kaplan-Meier survival analysis of CD133 expression with disease-free survival (DFS) and overall survival (OS). Patients with high CD133 expression had a short DFS ( 0.0145) and OS ( 0.0219).
Association between CD133 expression and survival
We analyzed the disease-free survival (DFS) and overall survival (OS) in 121 invasive breast cancers (78 cases with complete survival follow-up data and 43 lost visit) by Kaplan-meier curves. There was a statistically significant difference base on CD133 expression ( 0.0145, 0.0219, respectively) (Fig. 2).
Discussion
In this study, we found the positive expression rate of CD133 gradually increased in usual breast hyperplasia, atypical breast hyperplasia, breast carcinomas in situ, and invasive breast carcinomas, with progression of lesions. It was similar to expression pattern of CD44/CD24 in above mentioned tissues, which suggested : 1) Two types of positive cells labeled as stem cells are similarly distributed among benign and malignant breast lesions, accordant with distribution characters of stem cells in tissues [21]. 2) CD133 can mark stem cells in usual breast hyperplasia, atypical breast hyperplasia, and can also mark CSCs in invasive breast carcinomas tissues. Stem cells in normal breast and breast cancer stem cells have similar cell surface markers. Normal breast stem cells may be transformed into breast cancer stem cells via genetic mutation under carcinogenic factors [22]. 3) Expression rates of CD133 stem cells are increasing gradually in usual breast hyperplasia, atypical breast hyperplasia, breast carcinoma in situ and invasive breast carcinoma. Because stem cells have self-regenerating capacity, tissue proliferation and regeneration in the above diseases are enhanced in order, accordant with biological characters and clinical pathological characters of different lesions.
CD133 expression rate increased gradually in breast cancer tissues with histological grades and cancer stages. In addition, breast cancer with lymphatic metastasis or remote metastasis has higher CD133 rate compared to those without metastasis, suggesting that breast cancer stem cells with CD133 are closely related with infiltration and metastasis of breast cancer. Compared to differentiated cancer cells, breast cancer stem cells have more powerful capacity of movement and infiltration. The mechanism is as follows. Breast cancer stem cells can obtain characters of interstitial cells via epithelial mesenchymal transition (EMT), resulting in disintegration of epithelial cell connection, formation of cell matrix adhesion, and promoting metastasis [23]. It is indicated in a study that, breast cancer stem cells, considered as the initial cells from remote metastatic lesions, are present in circulating blood and marrow in patients with early breast cancer [24]. The role and mechanism of CD133 breast cancer stem cells in breast cancer infiltration and metastasis remain to be further studied.
Tumor relapse is an important reason for therapeutic failure of breast cancer. This study indicates that, CD133 expression rate was higher in patients with relapsed tumor cancer than in patients without relapsed tumors, suggesting that CD133 cell is related with breast cancer relapse. A study has demonstrated that, after chemotherapy, the proportion of breast cancer stem cells increases [25], indicating that breast cancer stem cells are resistant to chemotherapy. This phenomenon is due to certain transport protein highly expressed on the tumor stem cell surface has “drug pump” effects, which means this type of transport protein can excrete chemotherapy drugs out of cell [26]. In addition, tumor cells highly express survivin, lowly express apoptosis promoting genes, and inhibit the killing effects of chemotherapy drugs [27]. CSCs have stronger DNA repairing capacity, which can resist DNA damage resulted by radiotherapy and chemotherapy [28]. Breast cancer stem cells can escape from the killing effects of radiotherapy and chemotherapy via the above mentioned mechanisms, then become the root of tumor relapse. To a certain extent, the positive rate of CD133 cells in breast cancer tissues represents the amount of breast cancer stem cells in tissues and the possibility of relapse after therapy. Beyond thatthe prognosis of breast cancer can be predicted by detecting the positive rate of CD133 cells in breast cancer tissues. For the study of the resistance mechanism of breast cancer stem cells to radiotherapy and chemotherapy, it is very critical to find effective therapeutic targets for breast cancer.
In our study, we found that there was no significant correlation between CD133 expression and factors such as age and menopausal status of the patients, histological type. However, Lin detected that CD133 expression was lower in papillary carcinomas of breast than that in other type breast carcinomas [18]. In our study, we focus on the invasive ductal carcinoma instead of other types. There were few other types of breast carcinomas specimen. Moreover, CD133 positive expression rate was not significantly correlated with tumor size, ER, PR, Her-2 status in this research. However, Kim et al. found CD133 expression in invasive breast carcinomas was associated with the above mentioned parameters [15]. Ieni et al.’s studies indicated that there were no significant relationships between CD133 positive expression and hormone receptor expression, whereas a significant correlation between CD133 and Her-2 status [16, 17]. The difference may be resulted from the different scoring systems and different regions and populations. It needs more studies to confirm it.
Available study results have indicated that stem cells obtained by culture and separation only account for an extremely small portion of total cells, about 1%–5%. In our study, in some invasive breast cancers, CD133 labeled cells account for a higher percentage, far higher than the distribution ratio of stem cells in tissues. While similar phenomena are observed in other stem cells markers in different tumor tissues, suggesting that cells with positive stem cells markers are not necessarily tumor stem cells [29, 30]. It still needs further studies on specificity of stem cell markers and identification of tumor stem cells.
In summary, CD133 breast cells are distributed in benign and malignant lesions of the breast, whose expression rate is gradually increasing with the malignancy of the diseases. In benign hyperplasia in breast, CD133 cells may be normal stem cells of the breast. But under effects of oncogenic factors, these cells may be transformed into CD133 breast cancer stem cells. The number of CD133 breast cancer cells is closely related with infiltration and metastasis of breast cancer, so adopted as a parameter to predict malignancy and prognosis of breast cancer. CD133 breast cancer cells are resistant to radiotherapy and chemotherapy, which may be an important reason for relapse of breast cancer. In studies on breast cancer, it is critical to further investigate the mechanism of CD133 breast cancer stem cells in infiltration and metastasis and the mechanism of resistance CD133 breast cancer stem cells of to radiotherapy and chemotherapy.
Footnotes
Conflict of interest
All authors declare that they have no conflict of interests.
References
1.
JemalA.BrayF.CenterM.M.FerlayJ.WardE. and FormanD., Global cancer statistics, CA Cancer J Clin61(2) (2011), 69–90.
2.
WangL.ZhangY.LiR.ChenY.PanX.LiG. et al., 5-aza-2’-deoxycytidine enhances the radio-sensitivity of breast cancer cells, Cancer Biother Radiopharm28(1) (2013), 34–44.
3.
SleemanJ.P. and CremersN., New concepts in breast cancer metastasis: Tumor initiating cells and the microenvironment, Clin Exp Metastasis24(8) (2007), 707–715.
4.
Al-HajjM.WichaM.S.Benito-HernandezA.MorrisonS.J. and ClarkeM.F., Prospective identification of tumorigenic breast cancer cells, Proc Natl Acad Sci U S A100(7) (2003), 3983–3988.
5.
GinestierC.HurM.H.Charafe-JauffretE.MonvilleF.DutcherJ. and BrownM., ALDH1 is a marker of normal and malignant human mammary stem cells and a predictor of poor clinical outcome, Cell Stem Cell1(5) (2007), 555–567.
6.
SinghS.K.ClarkeI.D.TerasakiM.BonnV.E.HawkinsC.SquireJ. et al., Identification of a cancer stem cell in human brain tumors, Cancer Res63(18) (2003), 5821–5828.
7.
SuetsuguA.NagakiM.AokiH.MotohashiT.KunisadaT. and MoriwakiH., Characterization of CD133+ hepatocellular carcinoma cells as cancer stem/progenitor cells, Biochem Biophys Res Commun351(4) (2006), 820–824.
8.
BrunoS.BussolatiB.GrangeC.CollinoF.GrazianoM.E.FerrandoU. et al., CD133+ renal progenitor cells contribute to tumor angiogenesis, Am J Pathol169(6) (2006), 2223–2235.
9.
MiyataT.OyamaT.YoshimatsuT.HigaH.KawanoD.SekimuraA. et al., The clinical significance of cancer stem cell markers ALDH1A1 and CD133 in lung adenocarcinoma, Anticancer Res37(5) (2017), 2541–2547.
10.
LiC.WangC.XingY.ZhenJ. and AiZ., CD133 promotes gallbladder carcinoma cell migration through activating Akt phosphorylation, Oncotarget7(14) (2016), 17751–17759.
11.
ZhouJ.Y.ChenM.MaL.WangX.ChenY.G. and LiuS.L., Role of CD44 (high)/CD133 (high) HCT-116 cells in the tumorigenesis of colon cancer, Oncotarget7(7) (2016), 7657–7666.
12.
SaricanbazI.KarahaciogluE.EkinciO.BoraH.KilicD. and AkmansuM., Prognostic significance of expression of CD133 and Ki-67 in gastric cancer, Asian Pac J Cancer Prev15(19) (2014), 8215–8219.
13.
WrightM.H.CalcagnoA.M.SalcidoC.D.CarlsonM.D.AmbudkarS.V. and VarticovskiL., Brca1 breast tumors contain distinct CD44+/CD24- and CD133+ cells with cancer stem cell characteristics, Breast Cancer Res10(1) (2008), R10.
14.
StorciG.SansoneP.TrereD.TavolariS.TaffurelliM.CeccarelliC. et al., The basal-like breast carcinoma phenotype is regulated by SLUG gene expression, J Pathol214(1) (2008), 25–37.
15.
KimS.J.KimY.K.JangE.D.SeoK.Y. and KimU.S., Prognostic impact and clinicopatho logical correlation of CD133 and ALDH1 expression in invasive breast cancer, J Breast Cancer18(4) (2015), 347–355.
16.
IeniA.GiufferG.AdamoV. and TuccariG., Prognostic impact of CD133 immuno-expression in node-negative invasive breast carcinomas, Anticancer Res31(4) (2011), 1315–1320.
17.
GiuffrèG.AdamoV.IeniA.ColoneseF.BarresiV.CaristiN. et al., Hematopoietic progenitor cells (HPCs) in node-negative invasive breast carcinomas: Immunohistochemical analysis and clinicopathological correlations, Pathol Res Pract207(8) (2011), 487–491.
18.
LinC.H.LiuC.H.WenC.H.KoP.L. and ChaiC.Y., Differential CD133 expression distinguishes malignant from benign papillary lesions of the breast, Virchows Arch466 (2015), 177–184.
19.
WangY.Y.WangL.ChenY.LiL.YangX.T. and LiB.L., ER81 expression in breast cancers and hyperplasia, Patholog Res Int2011 (2011), 980513.
20.
ErnsterV.L.BarclayJ.KerlikowskeK.WilkieH. and Ballard-BarbashR., Mortality among women with ductal carcinoma in situ of the breast in the population-based on surveillance, epidemiology and end results program, Archives of Internal Medicine160(7) (2000), 953–958.
21.
ReyaT.MorrisonS.J.ClarkeM.F. and WeissmanI.L., Stem cells, cancer, and cancer stem cells, Nature414(6859) (2001), 105–111.
22.
MolyneuxG.ReganJ. and SmalleyM.J., Mammary stem cells and breast cancer, Cell Mol Life Sci64(24) (2007), 3248–3260.
23.
ManiS.A.GuoW.LiaoM.J.EatonE.N.AyyananA.ZhouA.Y. et al., The epithelial-mesenchymal transition generates cells with properties of stem cells, Cell133(4) (2008), 704–715.
24.
BalicM.LinH.YoungL.HawesD.GiulianoA.McNamaraG. et al., Most ear1y disseminated cancer cells detected in bone marrow of breast cancer patients have a putagive breast cancer stem cell phenotype, Clin Cancer Res12(19) (2006), 5615–5621.
25.
PhillipsT.M.McBrideW.H. and PajonkF., The response of CD24 (-/low)/CD44+ breast cancer-initiating cells to radiation, J Natl Cancer Inst98(24) (2006), 1777–1785.
26.
GottesmanM.M.FojoT. and BatesS.E., Multidrug resistance in cancer: Role of ATP-dependent transporters, Nat Rev Cancer2(1) (2002), 48–58.
27.
EiseleL.Klein-HitpassL.ChatzimanolisN.OpalkaB.BoesT.SeeberS. et al., Differential expression of drug-resistance related genes between sensitive and resistant blasts in acute myeloid leukemia, Acta Haematol117(1) (2007), 8–10.
28.
BaoS.WuQ.McLendonR.E.HaoY.ShiQ.HjelmelandA.B. et al., Glioma stem cells promote radio-resistance by proferential activation of the DNA damage response, Nature444(7120) (2006), 756–760.
29.
PatrawalaL.CalhounT.Schneider-BroussardR.ZhouJ.ClaypoolK. and TangD.G., Side population is enriched in tumorigenic, stem-like cancer cells, whereas ABCG2+ and ABCG2- cancer cells are similarly tumorigenic, Cancer Res65(14) (2005), 6207–6219.
30.
ShmelkovS.V.ButlerJ.M.HooperA.T.HormigoA.KushnerJ.MildeT. et al., CD133 expression is not restricted to stem cells, and both CD133+ and CD133- metastatic colon cancer cells initiate tumors, J Clin Invest118(6) (2008), 2111–2120.