
Abstract
BACKGROUND AND AIM:
We aimed to quantify monocyte subsets in newly diagnosed pediatric patients with solid tumors at South Egypt Cancer Institute (SECI) and Assiut University Hospital (AUH), and investigate their roles in the treatment outcomes.
PATIENTS AND METHODS:
This is a prospective case-controlled study included 100 patients with de novo solid tumors and forty age and sex matched healthy children to provide blood samples as control subjects to determine normal count of monocyte subsets, blood samples were collected from cancer patients before the first cycle of chemotherapy, these blood samples were subjected to routine laboratory tests and assessment of monocyte subsets using flow cytometry.
RESULTS:
Significant accumulations of intermediate monocytes and non classical monocytes (
CONCLUSION:
Solid conclusion regarding the impact of monocyte classes in pediatric tumors is premature, although, in this study, non-classical and intermediate monocytes were associated with better response to treatment in pediatric solid tumors and non-classical monocytes were correlated with higher overall survival; further studies are needed for better understanding and specification of monocyte functions in different pediatric tumors.
Introduction
Pediatric solid tumors have an overall better prognosis compared with adult cancers [1]. However, it remains poor for patients with metastatic or relapsed solid malignancies in spite of aggressive therapeutic multimodalities utilizing surgery, radiation, and intensive chemotherapy.
Pediatric solid tumors incorporate carcinomas derived from epithelial cells and sarcomas derived from mesenchymal cells. Solid tumors can develop from any of the three germ cell layers: mesoderm, endoderm or ectoderm [2].
Monocytes are essential components of the innate immune system that are responsible for phagocytosis of pathogens, dead cells, and anti-tumor activities [3]. The conception that the immune system by its components including monocytes has a protective role in tumor development is well established [4], a recent study suggests a converse role in promoting tumor initiation, neo-angiogenesis and progression [5]. This conflicting role of monocytes in normal and tumor development may result in the polarized expression of either pro- or anti-tumor functions.
Recognition of different monocyte subsets helps in explaining this paradoxical action [6]. Circulating human monocytes are broadly classified on the basis of their expression patterns of CD16 (Fc
Classical monocytes (CD14
Circulating monocytes expressing Tie-2 receptor [Tek tyrosine kinase receptor] named TEM or Tie-2 expressing monocytes, comprised within NCM, are recruited to the tumor where they have a proangiogenic activity through binding with angiopoietin-2 released by activated endothelial cells and angiogenic vessels [9]. Local tumor environment change affects the behavior of monocyte functions, either pro or antitumor ability [10].
The proportion of non-classical monocytes is small in myeloma patients with normal to low bone marrow levels of plasma cells and this proportion increases with increasing bone marrow myeloma load [11].
It has been widely accepted that tumor progression is an inherently proinflammatory process that includes the activation of the innate and adaptive immune system. During tumorigenesis, monocytes give anti-tumor response of the host and are considered as cytotoxic effector cells, also act to present tumor-associated antigens to tumor-infiltrating lymphocytes.
Recruitment of monocytes especially TEM into the tumors is influenced by several factors like MCP1 (chemoattractant protein 1), placental growth factor (PGF), TGF-
Human monocyte subsets may represent a novel prognostic marker in clinical medicine, and thorough investigations of their characteristics in bone marrow and peripheral blood for better understanding of their development, maturation, specialized functions and their impact in different diseases including cancers are required.
At present, a paucity of data regarding the impact of different circulatory monocyte subsets in cancers especially pediatric solid cancers is known and whether this paradoxical change is obvious or not; we aimed to quantify monocyte subsets in newly diagnosed pediatric patients with solid tumors at South Egypt Cancer Institute and Assiut University Hospital and investigate their roles in treatment outcomes.
Materials and methods
This study has been approved by the ethical committee of South Egypt Cancer Institute (SECI), with approval ID 98 date 17/2/2013. Written informed consents from all patients’ relatives and their controls were taken.
This is a prospective cohort study included 100 patients with de novo solid tumors presented to Pediatric Oncology Department, SECI, and Clinical Oncology Department, Assiut University, during the period from January 2014 to May 2016.
Patients were eligible for participation if they had histologically confirmed newly diagnosed malignant solid tumor (either localized or metastatic), 12 months to 18 years of age, and had not yet received anticancer therapy. All patients with previous chemotherapy or surgery (other than tumor biopsy) within 4 weeks were excluded.
Flow cytometric detection of monocytes subsets. A: Forward (FSC) and side scatter (SSC) histogram was used to detect monocyte (R1). B: CD14-FITC and CD16-PE positive cells were then identified among monocytes. CL-Mo (Classical monocytes, CD14++CD16-), In-Mo (intermediate monocytes CD14+CD16+), and Non Cl-Mo (non-classical monocytes CD14+CD16++) were then detected.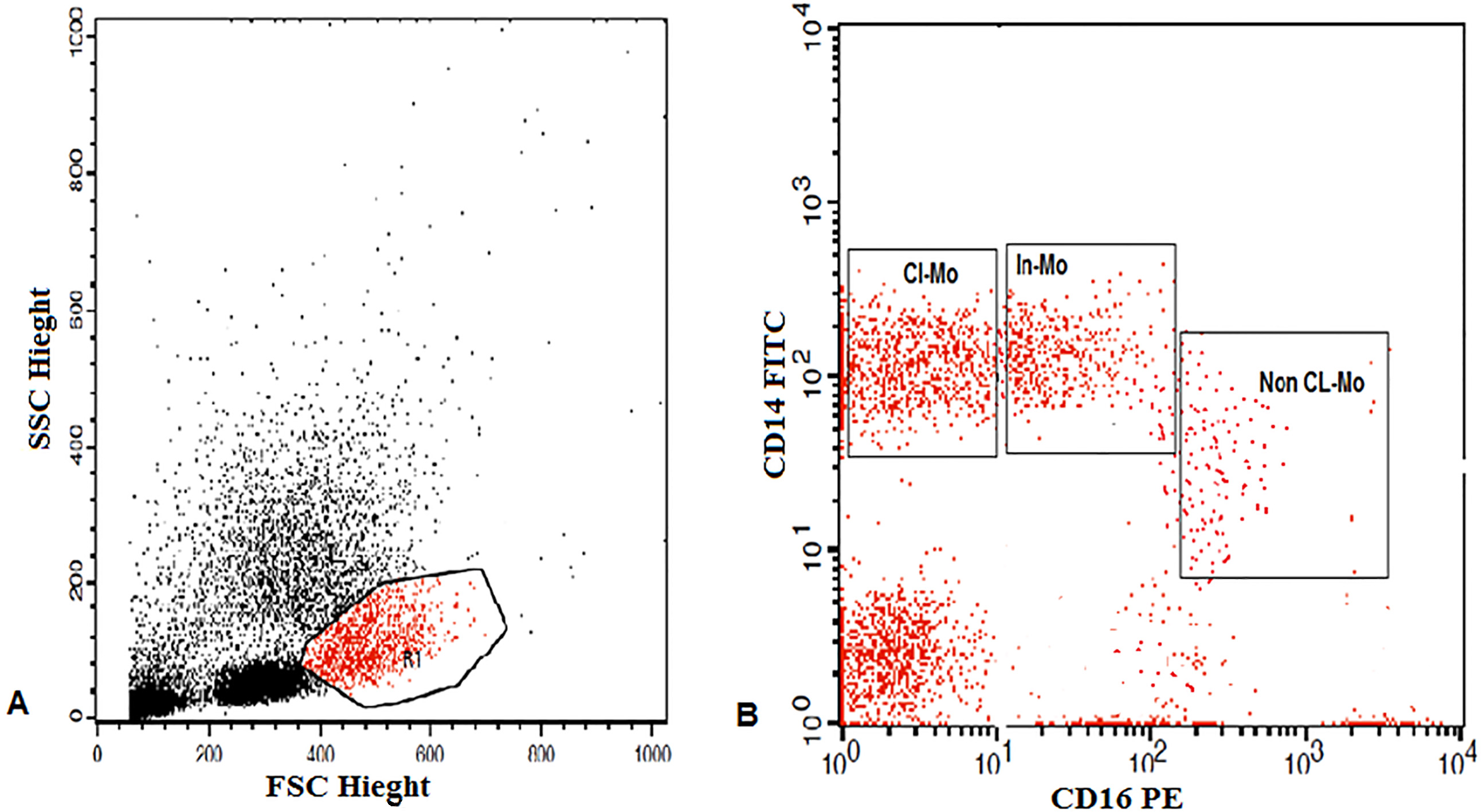
Patients’ groups: The type of cancer was diagnosed according to standard histopathologic, immunohistochemical, radio-imaging and tumor markers relevant to each type. Patients were categorized according to diagnosis into three groups: embryonal tumors [Neuroblastoma (NB), Wilms’ tumor (WT), Retinoblastoma (RB) and Hepatoblastoma (HB)], sarcomas [Rhabdomyosarcoma (RMS), Osteosarcoma (OS) and Ewing sarcoma (ES)] and other rare tumors.
Control group: Forty age and sex matched healthy children were provided blood samples as control subjects to determine the normal count of monocyte subsets. They were recruited from siblings of patients attending Pediatric Oncology Outpatient Clinic, SECI, Assiut University.
Surgical interventions: prior surgery was specified according to different tumor types with the aim to achieve complete tumor resection with good safety margins as in soft tissue sarcomas or limb sparing or amputation surgeries as in bone sarcomas, nephrectomies, and debulkings. With the advance of laparoscopic instruments and techniques, a variety of pediatric solid tumors can be resected safely by the minimally invasive technique but its role still uncertain due to the small number in the current series, prior surgery more than four weeks before enrollment in this study was allowed. Incisional or excisional biopsy were done in some cases for better histopathologic and immunohistochemistry diagnosis.
Blood samples were prospectively collected from cancer patients before the first cycle of chemotherapy.
The most common chemotherapy regimens used were backboned with platinum drugs including PE regimen (cisplatin or carboplatin plus vepside) in brain tumors, SIOPEL 3/3HR protocols (cisplatin alone for standard risk hepatoblastoma patients, cisplatin
All patients were subjected to:
Thorough history taking and clinical examination, with careful assessment of clinical signs. Routine laboratory tests: e.g. complete blood picture (CBC) by Ruby Cell Dyn (American, Serial number: 36026BG), liver function test, and renal chemistry by Cobasintegra 400 plus (Swiss, Serial number: 500558). Blood samples from the patients and the controls were subjected to assessment of monocyte subsets using flow cytometry.
Flow cytometric detection of monocytes subsets
For detection of monocytes subsets, 50
Response evaluation was carried out after the end of chemotherapy and was defined into categories of progressive disease (PD), stable disease (SD), and partial remission (PR) according to Response Evaluation Criteria in Solid Tumors (RECIST).
Follow-up of the patients was ended on May 2018. Overall survival (OS) of patients is defined as the time from the start of chemotherapy to date of patients’ death or last follow up. Progression free survival (PFS) of patients is defined as the time that patients remain free from progression including local and distant progressions or death.
Statistical analysis
This study was designed to test the null hypothesis that the treatment outcomes for all pediatric solid tumors weren’t affected by the pretreatment levels of monocyte classes.
Data analysis was performed with the Statistical Package for Social Sciences (SPSS version 21). Statistical comparisons were performed using the Independent Sample
Results
We enrolled 100 pediatric patients over a period of two years, their median age was 7.01
Characteristics of patients with pediatric solid malignancies enrolled in the study (
100)
Characteristics of patients with pediatric solid malignancies enrolled in the study (
Upon analysis of the type of circulating monocytes in 100 pediatric patients compared to 40 normal controls; we found significant accumulations of intermediate monocytes and non classical monocytes (
Circulating monocyte types in pediatric patients with solid tumors and the control group
Data presented as mean percentage
Relations between types of monocytes and different Clinicopathologic characteristics
Correlations between survival and different monocytes subsets
Having a younger age, means significantly higher percentage of intermediate monocytes as there was significant negative correlation between age and intermediate monocytes (
The median OS for our patients was 27 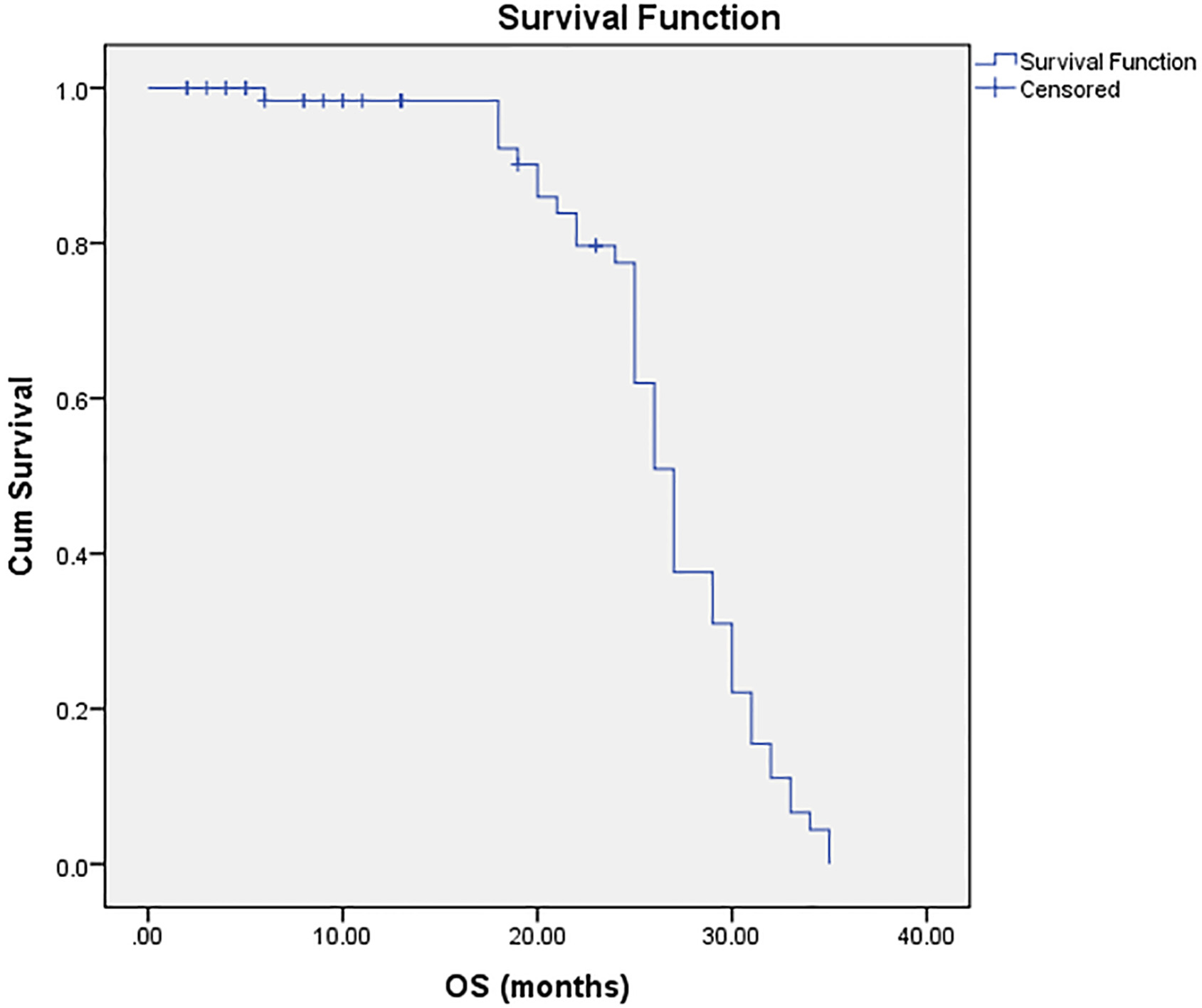
The median PFS of our study patients was 26 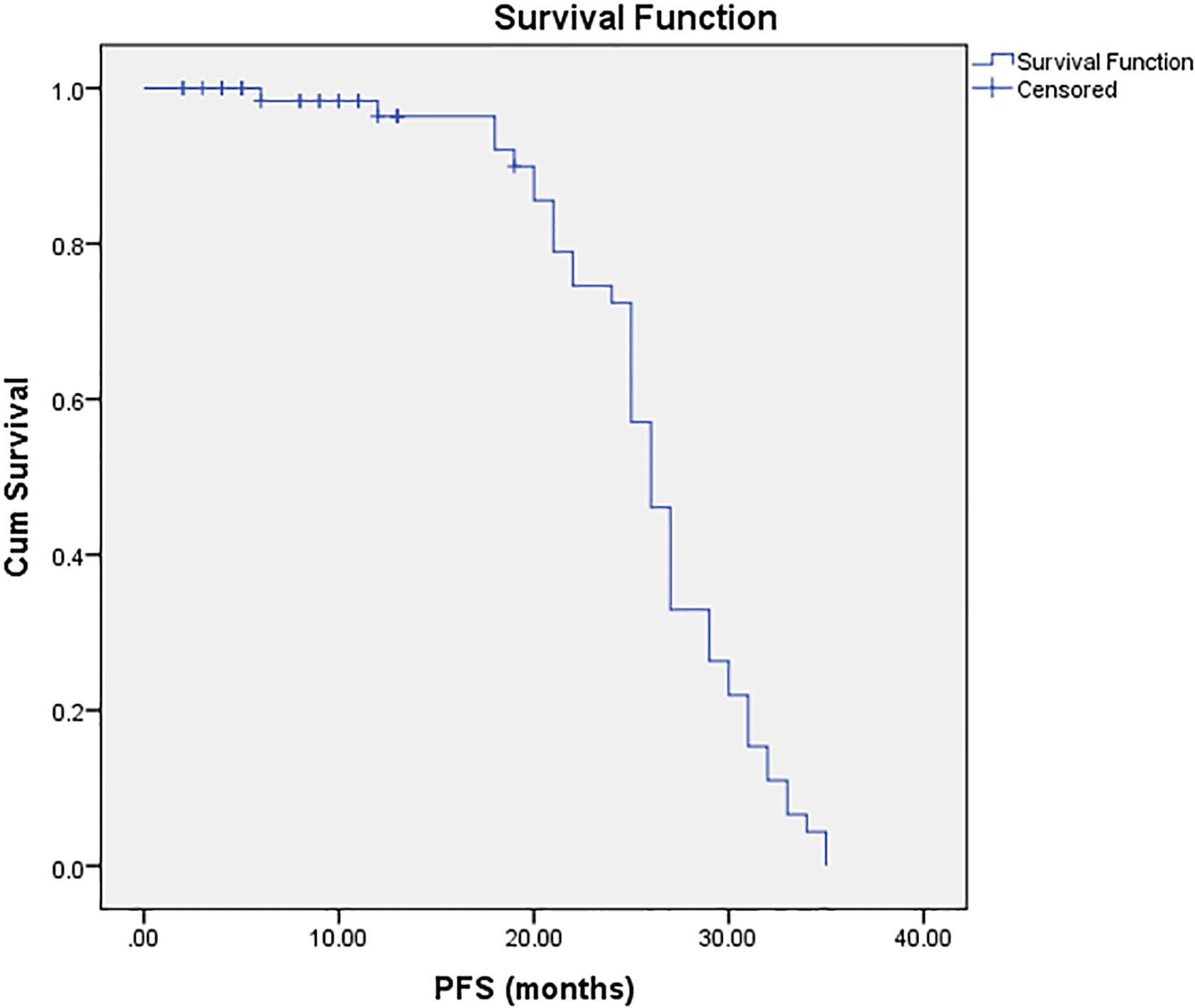
Simple scatter/dot graph of correlation with fit-line between OS and NCM with 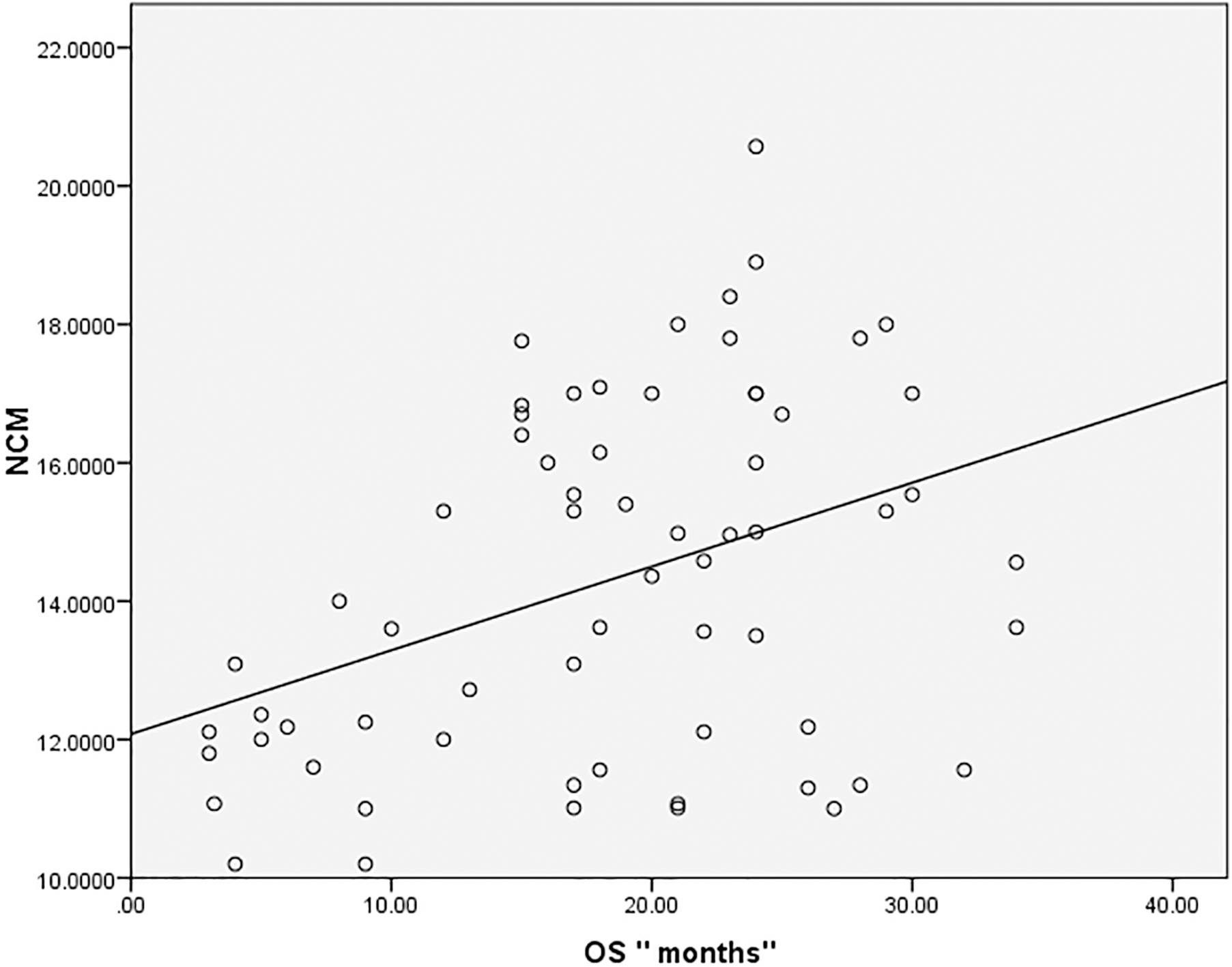
The median OS for 100 patients with pediatric solid tumors involved in our study was 27
Correlations were done between different monocyte subsets and survival and we found that there was a significant positive correlation between non-classical monocytes and OS denoting longer overall survival was achieved in those patients with higher mean percentage of non-classical monocytes (
Discussion
Over decades, the role of monocytes in inflammation was actively studied while recently the researchers started gaining insights regarding their role in cancers.
It was in the late 1980s until Passlik et al. recognized different monocyte types based on their expression of specific surface antigen CD16 [12]. Classical monocytes are important components of innate immunity, they lack CD16 antigen expression (CD14
The expansion of non-classical (CD16
There is growing evidence suggesting a role for non classical monocytes in prevention of hematogenous spread of malignancies [21] where it was detected that these cells concentrated in the vasculature near intravenously injected cancer cells, furthermore, extravasated at tumor sites to engulf tumor materials.
Jung et al. found that NCM promoted resistance to anti-VEGF therapy in colorectal cancers. Bevacizumab resulted in an upregulation of CX3CL1 in human colon cancer specimens. Enhanced CX3CL1 expression facilitated mobilization of NCM to the vascular bed of the tumor, where they enhanced recruitment of neutrophils. Both NCM and neutrophils inhibited anti-tumor
The previous studies supported in part our results that demonstrated significant accumulation of NCM, and IM in cases rather than controls.
Recent studies have demonstrated conflicting roles for monocytes in tumorigenesis and tumor treatment. Monocytes can mediate anti-tumor responses by presenting tumor-associated antigens to tumor infiltrating cytotoxic
It is known that tumor-derived factors attract circulating monocytes into the tumor site where they become differentiated into macrophages (TAM), TAM are heterogeneous group of myeloid precursors whose functions and phenotypes differ according to the type, location, and stage of the tumor [24].
TAM infiltration was correlated with poor prognosis in many cancers like breast, cervical, bladder, rectal cancers, but conflicting role was evidenced in other cancers like prostate, lung, brain cancers.
In a study done in stage II/III colorectal cancer patients; the level of peripheral blood monocytes was associated with the density of tumor associated macrophages (TAM) in cancer microenvironment, in addition, PFS and OS were significantly worse in patients with high level of TAMs and concluded that the level of peripheral blood monocytes was a useful negative prognostic marker [25], our results were contradictory to these results as NCM was correlated positively with OS.
It is hypothesized that TAM in the pre-tumor and early tumor stages contribute to neoplastic transformation, tumor growth, angiogenesis, and immunosuppression, while they can influence every stage of tumor development and progression through phagocytosis of metastatic cells and participation in cancer immune-editing [26].
CD16
All of the above studies supported directly and indirectly our results, however, Studies in gene expression profiles in monocyte subpopulations as part of tumor biology remain scarce and future studies will be needed to understand their accurate roles as well as define future approaches to modulate them to promote antitumor activity, and to explore whether this paradoxical change of monocytes from the antitumor effect to immunosuppressive effect was evident and explained in different pediatric malignancies or not, and if it was correlated with more aggressive types of pediatric tumors than others especially those with high metastatic rates, also our study might imply indirectly that the antitumor effect of monocyte especially NCM could be present in localized and locoregional tumors before these tumors became metastatic. This study may be a unique one in dealing with the role of different monocyte subpopulations specifically in pediatric solid tumors and need to be supported by future studies.
The hypothesis that NCM functions in the tumor vasculature by orchestrating the killing and clearance of metastasizing tumor cells and supporting CAR
Taken together, these results suggest that monocyte subsets may play ramified roles in the different phases of tumor behavior and highlight the importance of understanding the mechanisms by which NCM contribute to anti-tumor immunity before they can be targeted for therapy.
Conclusion
Solid conclusion regarding the impact of monocyte classes in pediatric tumors is premature, although, in this study, non-classical and intermediate monocytes were associated with better response to treatment in pediatric solid tumors and non-classical monocytes were correlated with higher overall survival; further studies are needed for better understanding and specification of monocyte functions in different pediatric tumors.