
Abstract
BACKGROUND AND OBJECTIVE:
Renal cell carcinoma (RCC) is the urological malignancy with the highest mortality rate and is increasing in incidence. The prognostic and predictive biomarkers are highly desired. This study aims to investigate the significance of superoxide dismutase 2 (SOD2) as a clinical biomarker in patients with renal cell carcinomas.
METHODS:
A cohort of 97 patients with RCC was analyzed retrospectively using various clinical parameters and SOD2 expression by immunohistochemistry.
RESULTS:
Cases with stronger SOD2 positivity of the tumor in comparison to the adjacent normal renal tubule by immunohistochemistry were categorized as high SOD2 and were associated with worse overall survivals (
CONCLUSIONS:
High SOD2 expression can be predictive of a poor clinical outcome and be clinically useful in the follow-up of metastatic RCC. Therapeutics for metastatic RCCs require further improvement, such as supplementary administration of agents targeting mitochondrial SOD2.
Introduction
Renal cell carcinoma (RCC) is the urological malignancy with the highest mortality rate and is increasing in incidence [1]. The increased use of abdominal imaging, such as computed tomography and ultrasonography, has led to detection of incidental renal masses and consequently, patients with localized RCCs are in surge. Although radical nephrectomy remains a successful curative treatment for localized RCC, more than 30% of newly diagnosed cases are regionally advanced or eventually develop distant metastases [1]. Currently, advanced RCC cases with metastasis or recurrence are often treated with several molecular targeting drugs, which inhibit tyrosine kinase, vascular endothelial cell growth factor receptor (VEGFR), mammalian target of rapamycin (mTOR) kinase, etc. [2]. However, their therapeutic efficacy is poor. The common mechanism of action of these molecular targeting agents is based on nutrient starvation. The previous study investigated a novel target causing therapeutic resistance in “starvation-resistant” RCC cells, the study found that starvation-resistant cells possess high mitochondrial performance with sustained expression of superoxide dismutase 2 and mitochondrial function supported by stored carbon sources. In such RCCs, the current molecular targeting treatments based on nutrient starvation are not a rational therapeutic approach, however inhibition of the mitochondria can offer an effective therapeutic option for advanced RCC cases [3, 4, 5].
SOD2 is an enzyme that scavenges reactive oxygen species in the mitochondrial matrix. High SOD2 expression can inhibit cancer cell proliferation [6], but promote epithelial to mesenchymal transition and/or cancer cell migration [7]. At advanced stages, high SOD2 levels can positively contribute to metastatic tumor progression [8].
Here, we investigated the relationship betweenSOD2 expression by immunohistochemistry and various clinical parameters in a cohort of RCC patients. High SOD2 expression could predict a worse clinical outcome of RCCs cases.
Materials and methods
Patients
Previously, it was reported that higher SOD2 mRNA levels were significantly associated with poor survivals in metastatic RCCs [4]. In the present study, SOD2 expression was analyzed by immunohistochemistry in an independent cohort of patients with RCCs.
Ninety-seven patients who underwent radical or partial nephrectomy for the treatment of RCCs at the Shiga University of Medical Science Hospital from 1999 to 2015 were analyzed in this study. The median age of the patients was 62 years (34–82 years). There were 77 (79%) men and 20 (21%) females. The median follow-up period was 30 months (12–32 months) and the endpoint of the observation period was defined as death or the last visit to the hospital. Pathological types of RCC were 76 clear cell, 12 papillary, 8 chromophobe carcinomas, and 1 unclassified. T stages included 68 pT1, 4 pT2, 19 pT3, and 6 pT4. Vascular invasion and higher grading (G3) were identified in 67 and 18 cases, respectively. The pathological diagnosis and histological grading were made according to the WHO Histological Classification system [9], while the clinical stage was determined by the UICC TNM classification [10]. Radical and partial nephrectomies were performed in 51 (53%) and 46 (47%) patients, respectively. Surgery was performed in 70 (72%) patients as a curative measure whereas 27 (28%) patients underwent nephrectomy to reduce tumor size. A total of 27 (28%) patients had distant metastasis at the time of RCC diagnosis. A total of 25 (26%) patients were treated with molecular targeting drugs including sorafenib (
Immunohistochemistry
Surgical specimens were transferred to 10% buffered formalin and fixed overnight. Fixed samples were embedded in paraffin and serially sliced into 5
Representative micrographs showing SOD2 expression by immunohistochemistry. (A–C) “High SOD2 expression” case. (A) SOD2 staining of renal cell carcinoma cells. (B) is stronger than the staining of adjacently normal proximal renal tubules. (C) in the same specimen. (D–F) “Low SOD2 expression” case. (D) the positivity of renal cell carcinoma cells. (E) is less or similar than normal renal tubules. (F) The multiple punctate stainings of SOD2 observed in the cytoplasmic regions could strongly suggest its mitochondrial expression in both tumorous and normal tubular cells. The scale bars correspond to 100 
SOD2 expression of each RCC was determined by immunohistochemistry by relative comparison to SOD2 expression of adjacently normal proximal renal tubule as an internal control on the same slide. The multiple punctate stainings of SOD2 observed in the cytoplasmic regions could strongly suggest its mitochondrial expression in both tumorous and normal tubular cells. We could define two qualitative grades for specimens according to the intensity of SOD2 expression including: i) in “high SOD2” samples the staining intensity of the tumor was apparently stronger than that of normal proximal renal tubule; and ii) in “low SOD2” the intensity of the tumor was less or similar than the proximal tubules. These semi-quantitatively immunohistochemical comparison could offer us a non-ambiguous evaluation for tumorous SOD2 expression (Fig. 1).
Grading by immunohistochemistry was performed by two independent researchers (R.K., T.C.) who had no information of the clinical parameters.
Statistical analysis
The disease-specific overall survival interval was defined as the period from the point of diagnosis to the point of death as the result of RCC. All statistical analyses were performed using SPSS 22.0 (IBM Inc., Chicago, IL, USA). All tests for statistical significance were two-sided. A
Correlation between SOD2 expression and clinicopathological characteristics in 97 renal cell carcinomas
Correlation between SOD2 expression and clinicopathological characteristics in 97 renal cell carcinomas
Correlation between SOD2 expression and clinicopathological characteristics of renal cell carcinomas
Representative cases of high and low expressions of SOD2 are shown in Fig. 1A–C and D–F, respectively. SOD2 reactivity of normal renal tubules was used as an internal control of each histological section. The samples of cases with stronger SOD2 positivity of the tumor compared to the adjacent normal renal tubules were categorized as high SOD2 cases. A total of 26 (27%) and 71 (73%) cases were categorized as high and low SOD2, respectively. The correlation between SOD2 expression and clinicopathological characteristics is shown in Table 1. Although the pathological type (
Kaplan-Meier plot displaying overall survival of RCC patients with high and low SOD2 expression. Cases with high SOD2 expression had significantly shorter survival periods than cases with low expression (log-rank test, 
Prognostic evaluation of clinicopathological parameters for overall survival in 97 renal cell carcinomas by univariate and multivariate analyses
Prognostic evaluation of clinicopathological parameters for overall survival in 27 metastatic renal cell carcinomas by univariate and multivariate analyses
The 5-year OS of high and low SOD2 groups were 55.8% and 85.0%, respectively. The high SOD2 group had a worse survival curve than that of the low SOD2 group (log-rank test
SOD2 posses an especially predictive value in metastatic renal cell carcinomas
Among the 27 patients who had distant metastasis at diagnosis, high and low SOD2 expression RCC cases were 8 and 19, respectively. Regarding OS, the high SOD2 group showed a significantly lower survival rate than the low group (log-rank test
Kaplan-Meier plot displaying overall survival of 27 metastatic RCC patients with high and low SOD2 expression. Cases with high SOD2 expression had significantly shorter survival times than cases with low expression (log-rank test, 
In addition, 18 metastatic and 7 recurrent RCCs were analyzed in order to evaluate the efficacy of currently molecular targeting therapies in advanced RCC patients. The treatment resulted in partial responses in 10 cases, but no remission. Therefore, implementation of current molecular targeting therapies did not improve OS intervals in cases displaying high SOD2 RCCs expression (log-rank test
It has been previously reported the presence of enhanced mitochondrial function accompanied with high SOD2 levels in dormant-like starvation-resistant RCC cells, which complicates the therapeutic of RCC. Moreover, higher SOD2 mRNA levels in metastatic RCC were associated with significantly shorter survival intervals [4]. Apart from the cohort of previous study [4], here, SOD2 protein expression was assessed by immunohistochemistry in another independent cohort of patients with RCCs. We found that high SOD2 expression in RCC was significantly associated with worse prognosis, especially in patients with metastatic RCCs, where SOD2 expression was the maximum critical risk factor. The follow-up of RCC case with abundant SOD expression should be under the medical control more frequently and longer than those of RCC cases including subtle SOD2.
Kaplan-Meier plot displaying overall survival of 25 advanced RCC patients treated with molecular targeting therapies with high and low SOD2 expression. In this series, OS interval was defined as the period from the point of initial treatment to the point of RCC specific death. Cases with high SOD2 expression had significantly shorter survival periods than cases with low expression (log-rank test, 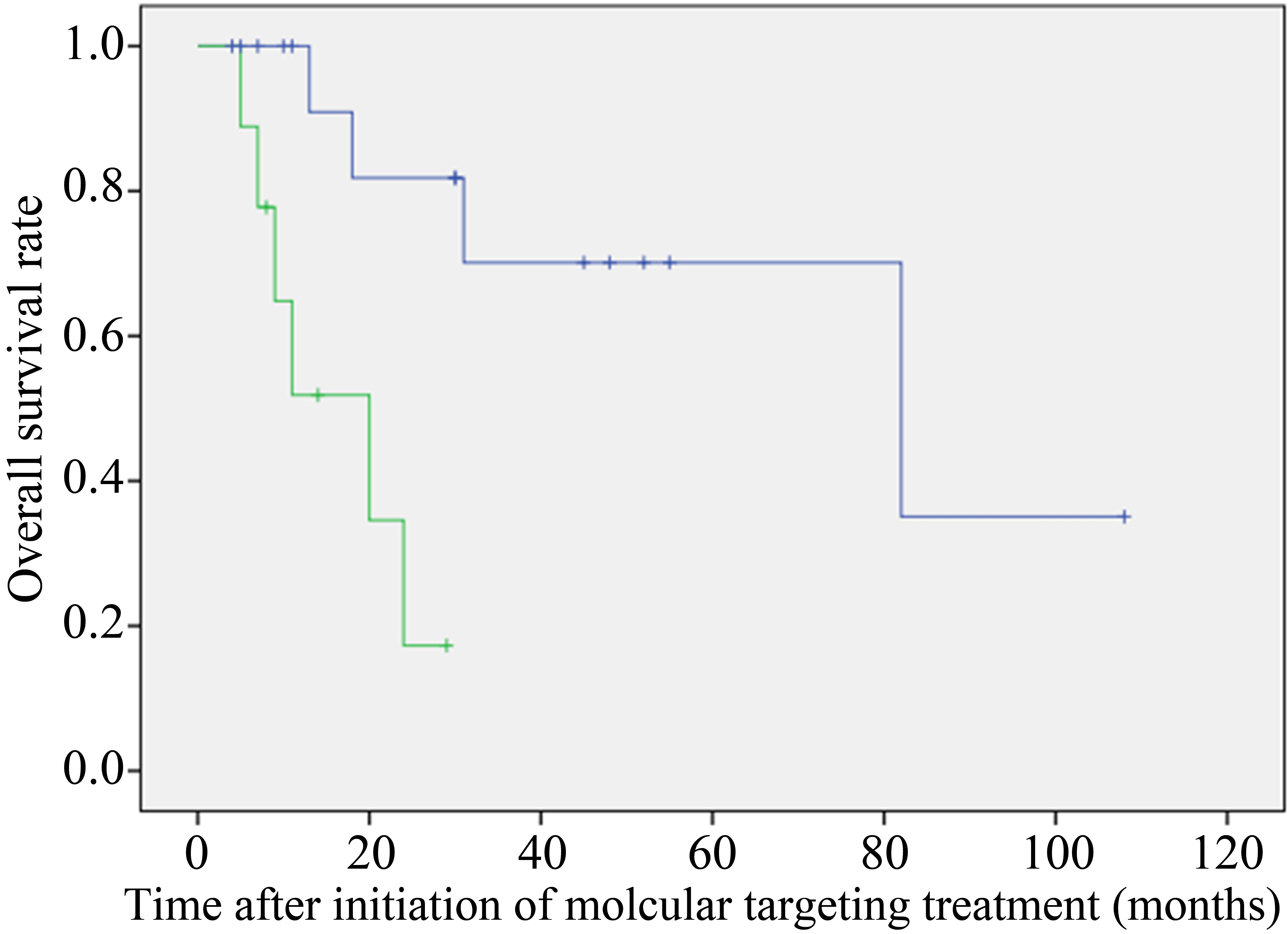
SOD2 is one of the primary mitochondrial antioxidants in a network of detoxification enzymes that neutralize highly reactive superoxide ions (
In this study, implementation of current molecular targeting therapies did not improve the prognoses of cases with high SOD2 tumor expression. The common mechanism of action of the currently applied molecular agents is based on nutrient starvation via the inhibition of tyrosine kinase, VEGFR, mTOR kinase, etc. [2]. RCCs are hypervascularized, and inhibiting angiogenesis is one of main objectives of anticancer molecular targeting therapies [12] and agents inhibiting tumor angiogenesis are widely used in the treatment of metastatic RCC. The mechanism of action of tyrosine kinase inhibitor (TKI) is based on nutrimental deprivation via the inhibition of tumor angiogenesis [12]. Although these newly developed agents have shown a certain degree of tumor volume reduction, complete remission is scarce, suggesting that current molecular targeting therapies are clinically problematic for the management of metastatic RCCs. It has been proposed that SOD2-abundant and starvation-resistant malignant cells can survive hostile environments like nutrimental starvation and one of the reasons for the low efficacy of molecular targeting techniques [13]. Therefore, treatment for metastatic and/or recurrent RCCs harboring cells with high SOD2 expression should be modified immediately. In the Checkmate 025 study [14], patients treated with nivolumab, an anti-PD-1 human immunogloblin [15], had a significantly better survival than the patients treated with everolimus, an mTOR inhibitor. This finding also suggests the need for second-line therapies and that nivolmab should become another therapeutic option after TKI treatment failure for metastatic RCCs [16, 17]. It has been previously demonstrated that two inhibitors targeting mitochondrial oxidative phosphorylation can become therapeutic options in SOD2-abundant RCC cells. Etomoxir, an inhibitor of beta-oxidation, and buformin, a biguanide that has been used for the treatment of diabetes mellitus, can inhibit mitochondrial oxidative phosphorylation and induce death of RCC cells [4]. Therefore, targeting mitochondrial activity with drugs such as etomoxir and biganide could be useful for the treatment of patients with poor prognosis due to SOD2-abundant RCCs and calls for drug repositioning.
In conclusion, we showed that high SOD2 expression is associated with worse clinical outcome and should be considered a useful marker in the follow-up of patients with primary and metastatic RCCs. Therapeutics for metastatic RCCs require further improvement, such as supplementary application of agents targeting mitochondrial SOD2.
Footnotes
Acknowledgments
We are grateful to Hiroko Kita and Masami Katsurai for experimental assistance. This study was supported in part by JSPS KAKENHI Grant Number 17K11131 (TYo. SK, TI), 16K11035 (TYu), 16K11001 (AK) and 18K09192 (SK, TC).
Conflict of interest
None declared.