
Abstract
Breast cancer is one common female specific malignant tumor and has gradually increased incidence. Matrix metalloproteinase-9 (MMMP-9) and its inhibitor TIMP-1 participate in tumor invasion and metastasis. This study analyzed the effect of various treatment approaches on TIMP-1 and MMP-9 levels in terminal stage breast cancer. Post-op breast cancer patients including chemo-radio therapy group, radio-chemo therapy group and simultaneously chemo- and radio-therapy group were compared for efficacy, along with assays for TIMP-1 and MMP-9 levels for analyzing their correlation with clinical-pathological features of breast cancer. Chemo
Introduction
China has increased incidence of breast cancer by years, with younger disease onset age, thus severely affecting female health. Survey showed that about 50% breast cancer patients were at pre-menopause stage, and about 60% of patients showed positive expression for estrogen [1]. An investigation for pathogenic factors showed that it was under the combined effects of genetic, hormonal, diet, radiation, and benign breast lesions. Commonly applied treatment approaches for breast cancer include surgery, chemotherapy, radiation, hormonal replacement and targeted treatment [2]. With progression of medicine technology, the treatment for breast cancer has been evolved from single approach to focal combined with systemic treatment including hormonal, radio- and chemo-therapy, which can significantly suppress the incidence of adverse effects such as radiation esophagitis or pulmonary fibrosis [3].
Major reasons for breast cancer related death are uncontrollable growth of tumors and distal metastasis, during which tumor cells must degrade extracellular matrix (ECM) for penetrating tissue barrier [4]. The degradation of ECM becomes the most important, and involves the action of multiple hydrolytic enzymes. The major type of these enzymes is matrix metalloproteinases (MMPs), in which type IV collagenase, or MMP-9, was the most widely studied one [5]. MMPs can degrade ECM to facilitate infiltration of malignant tumor cells into peripheral tissues, whilst tissue inhibitor of MMPs (TIMPs) could suppress the activity of MMPs and inhibit tumor invasion or metastasis [6]. TIMP-1 is a catalytic inhibitor for MMPs and one type of growth factor. Study showed the correlation between over-expression of MMPs and TIMPs and recurrence or metastasis of breast cancer [7]. In current study we recruited post-op breast cancer patients from Nantong Traditional Chinese Medicine Hospital and gave them post-op radio-therapy, post-op chemo-therapy, and post-op chemo plus radiotherapy, whose treatment efficiency was analyzed to test expression of MMP-9 and TIMP-1.
Materials and methods
Patient information
A total of 120 estrogen receptor positive breast cancer patients who received improved radical surgery in Nantong Traditional Chinese Medicine Hospital from January 2012 to January 2017 were recruited. Patients aged between 30 and 70 years (average age
Inclusive criteria
All patients received confirmed diagnosis by pathology, and did not receive novel auxiliary treatment before surgery. Hormonal replacement therapy was performed after surgery. All participants have signed informed consents and were able to accomplish this study.
Exclusive criteria
No severe dysfunction in vital organs including heart, liver and lungs. No complication with mesenchymal tissue or immune disorders. All patients did not receive radio-, chemo-, immune-, cyro- or laser- therapy before surgery. Patients were not complicated with malignant tumors in other organs or psychiatric disorders.
Reagent and equipment
Anastrozole (Yangzijiang Pharma., Certificate Doc# 000201, China); Tamoxifen (Fudan Fuhua Pharma., Certificate Doc# 031103, China). ELISA kit for MMP 09 and TIMP-1. Ultrapure workstation (Formal, USA). Normal centrifuge (Feige, China).
Patient treatment approach
All patients received hormonal replacement therapy. For menopausal patients, aromase inhibitor Anastrozole (1 mg/d) was applied, whilst other patients received estrogen receptor antagonist Tamoxifen (20 mg/d) for a 5-year course as stipulated by clinicians.
Chemo-radio therapy group
Patients received standard protocol (500 mg/m
Comparison of treatment efficiency
Comparison of treatment efficiency
Note: *,
Radiation therapy started at 2 weeks post-surgery, followed by 2-week rest and chemotherapy. Dosage or radiation field followed those in the chemo-radio therapy group.
Radio
chemo therapy group
Three-week radiotherapy was performed after surgery, followed by routine radiotherapy and another 3-week chemotherapy. Dosage or radiation field followed those in the chemo-radio therapy group.
ELISA for blood MMP-9 and TIMP-1 levels in patients
All patients were collected for fasted venous blood samples before and after treatment. Serum was isolated from venous blood and stored in fridge. ELISA was performed to detect serum levels of MMP-9 and TIMP-1. In brief, the number of wells required was calculated. The test kit was incubated at room temperature for 30 min, and standard samples were diluted. At each concentration, five replicated wells were tested. Samples were added for dilution, incubation, rinsing, development and quenching. Absorbance values at 450 nm wavelength were measured by a microplate reader. A liner regression function was plotted to calculate sample concentration.
Measurement of MMP-9 activity
The MMP-9 activity was measured with a specific MMP-9 monoclonal antibody in combination with an MMP-9 fluorogenic substrate, 5-FAM/QXL™520.
FRET peptide using SensoLyte
Observing indexes
All patients received 5-year follow-up for comparing treatment efficacy, including incidence of focal recurrence, distal metastasis, and 5-year survival rate.
Serum levels of MMP-9 and TIMP-1 of patients were compared before and after treatment.
One-way and multi-variant analysis was performed to reveal the correlation between serum MMP-9 and TIMP-1 levels 1 month post-treatment and clinical-pathological features.
Data processing
SPSS17.0 was used for data processing. Enumeration data were analyzed by chi-square test, and measurement data were processed by analysis of variance (ANOVA) and were presented as mean
Serum MMP-9 and TIMP-1 levels in patients before and after treatment. *, 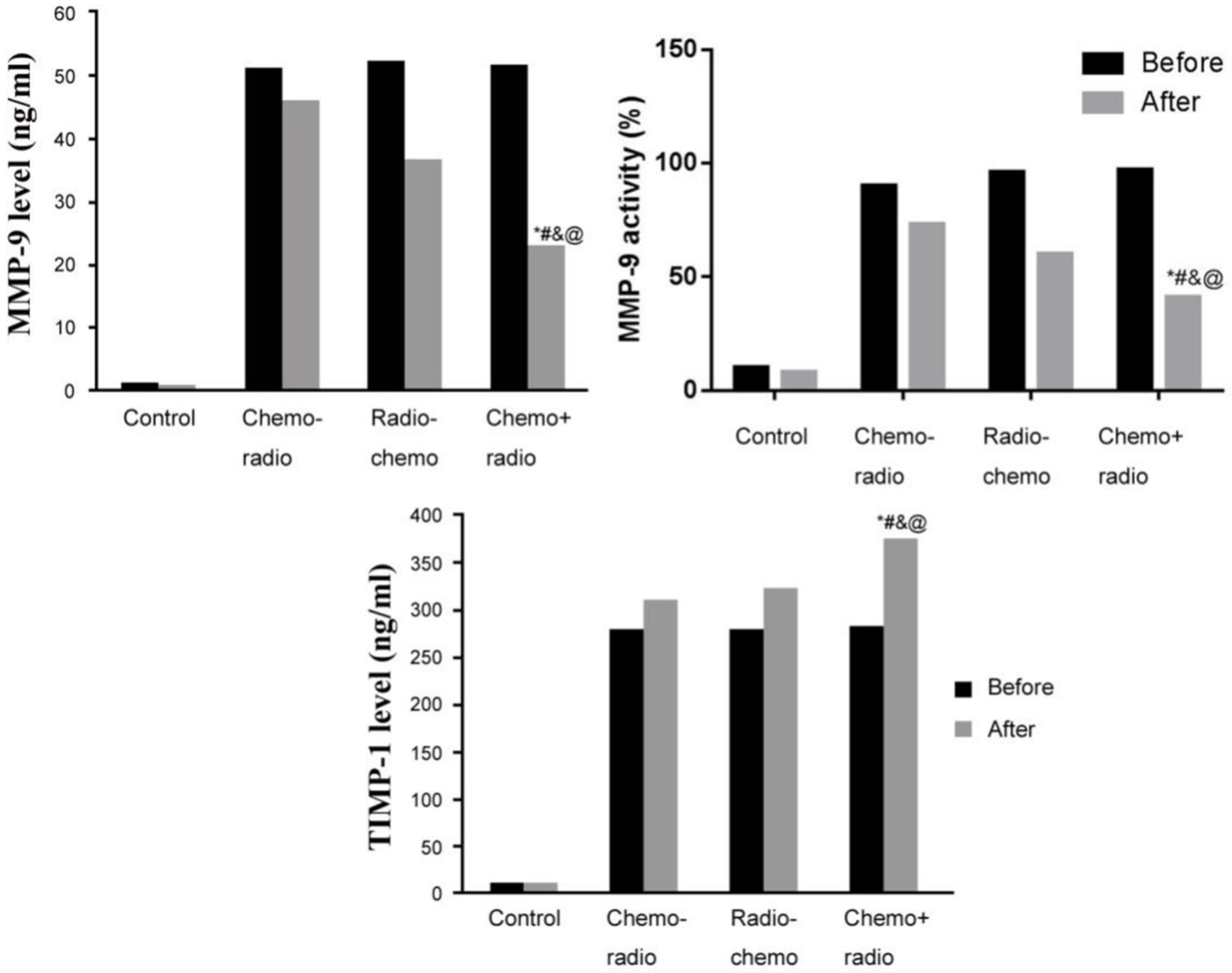
Comparison of treatment efficacy in patients
Treatment efficacy was compared among all groups of patients, including focal recurrent rate, distal metastasis rate and 5-year survival rate. Results showed that radio
Levels of MMP-9 and TIMP-1 in patients before and after treatment
Peripheral venous blood was collected before and after treatment to test serum MMP-9 and TIMP-1 levels. Results showed significantly higher serum MMP-9 and TIMP-1 levels in all three treatment groups compare to normal control group, with no significant difference among those three groups (
Correlation between serum MMP-9 or TIMP-1 levels in patients and clinical pathological features
We further compared the relationship between patient serum MMP-9 levels and clinical pathological features, including age, TNM stage, tumor size and lymph node metastasis. Results showed that post-treatment serum MMP-9 and TIMP-1 levels were correlated with patient age, TNM stage, tumor size and lymph node metastasis (
Multi-variant analysis for patient serum MMP-9/TIMP-1 levels and clinical/pathological features
Multi-variant Logistic analysis was performed to analyze factors including age, TNM stage, tumor size, and lymph node metastasis. Results showed that age, TNM stage, tumor size and lymph node metastasis were all independent risk factors (Table 3).
Correlation between serum MMP-9, TIMP-1 and clinical-pathological features
Correlation between serum MMP-9, TIMP-1 and clinical-pathological features
Multi-variate analysis of serum MMP-9/TIMP-1 levels and clinical/pathological features
The incidence of breast cancer was gradually increasing in recent years with aging population, thus severely threatening female health. The advancement of molecular biology has transformed the treatment for breast cancer from single surgery toward combined treatment including radio-, chemo-, endocrine- and targeted therapy [8]. However, data still showed no significant improvement of recurrent or metastatic rate of breast cancer, with high mortality. MMPs is one group of endopeptidase dependent on bivalent ions [9]. TIMPs is one family of endogenous regulator inhibiting MMPs activity [10]. Previous study showed important roles of MMPs and TIMPs in onset and progression malignant tumors [11, 12]. This study recruited post-op breast cancer patients to analyze treatment efficacy of post-op radiotherapy, post-op chemotherapy and post-op chemo
In this study, all recruited breast cancer patients were divided based on treatment approaches, and follow-ups were performed for comparing treatment efficiency. Radio
In malignant tumors, cytokines for mediating cell proliferation and apoptosis are critical, as their abnormal expression can induce tumor invasion or metastasis. In this study, we measured serum MMP-9 and TIMP-1 levels in patients before and after treatment. No significant difference existed in these parameters in all three groups before treatment. After treatment, all patients had lower serum MMP-9 levels and higher TIMP-1 levels than those before treatment. Chemo
MMP-9 is secreted out of cells in the enzymogen form to degrade type IV collagen, fibronectin, and affect cell adhesion potency, thus participating tumor cell growth, infiltration and metastasis [15, 16]. TIMPs are distributed in tissues and body fluids. As tissue inhibitor for MMPs, TIMPs can specifically bind with catalytic domain of MMP-9 enzymogen or activated enzymes to form tissue complex, for exerting specifically inhibitory functions on MMP-9 activity [17, 18]. This study showed that synchronous chemo- and radio-therapy in post-op breast cancer patients significantly suppressed patient MMP-9 level whilst increased TIMP-1 level.
This study further analyzed the correlation between patient serum MMP-9 and TIMP-1 levels and clinical/pathological features. Post-treatment serum MMP-9 and TIMP-1 levels were correlated with patient age, TNM stage, tumor size and lymph node metastasis. In those patients with older than 55 years, TNM stage at or beyond stage III, tumor maximal diameter larger than 5 cm or lymph node metastasis, serum MMP-9 levels were gradually decreased, with increased TIMP-1 level. Multi-variate analysis showed that age, TNM stage, tumor size and lymph node metastasis were all independent risk factors affecting serum MMP-9 and TIMP-1 levels. Previous study showed that both MMPs and TIMPs had abnormal expression in various malignant tumors including colon cancer, gastric carcinoma and pancreatic cancer, and were involved in tumor metastasis and invasion [19]. Breast cancer is one malignant tumor with epithelium origin, with potent invasion and metastasis ability. The degradation of matrix in basal membrane is closely correlated with MMPs activity and TIMPs levels at various subtypes [20]. Previous study showed elevated expression of MMP-9 and TIMP-1 in breast cancer tissues, and more potent increase with tumor growth and lymph node metastasis [21]. This study indicated that simultaneous radio- and chemo-therapy on post-op breast cancer patients could decrease serum MMP-9 level, increase TIMP-1 level, and suppress the probability of ECM recurrence, thus suppressing the incidence of tumor focal recurrence or distal metastasis.
Conclusion
Simultaneous chemo- and radio-therapy for breast cancer patients after radical resection surgery could decrease focal recurrent or distal metastatic rate, and improved 5-year survival rate. MMP-9 and TIMP-1 levels are correlated with patient age, TNM stage, tumor size and lymph node metastasis. Simultaneous chemo- and radio-therapy after surgery could help to decrease MMP-9 and increase TIMP-1 levels in breast cancer patients, with better efficacy than pure chemo- or radio-therapy after surgery. MMP-9 and TIMP-1 thus may become indicators predicting prognosis of breast cancer. Future studies can be pursued in cell or animal model to investigate detailed functional mechanism.
Footnotes
Acknowledgments
This work was supported by Nantong City Social Development Fund (No. MS12017017-4).
Conflict of interest
None.