
Abstract
BACKGROUND:
People with biomarkers above cut-off values normally have higher risk to develop pre-malignancies and malignancies.
OBJECTIVE:
Here we investigate if serological TK1 protein (STK1p), AFP, CEA and PSA below cut-off values predict development of pre-cancer.
METHODS:
The mean values and the concentration distribution of STK1p, AFP, CEA and PSA were determined in a cohort of 56,178 persons participating a health screening group, consist of people with non-tumor diseases, pre-malignancy and diseases associated with the risk process of malignancy. A health disease-free group (
RESULTS:
The STK1p below cut-off value (
CONCLUSION:
STK1p is a potential proliferating biomarker for early discover of persons in the risk to develop or already have pre-malignancies or diseases associated with the risk process of malignancy.
Introduction
Cancer is a leading cause of death worldwide. An estimated 40 million deaths occurred in 2015 due to non-communicable diseases (NCDs), accounting for 70% of the overall total of 56 million deaths. The majority deaths were caused by the two main NCDs, 17.7 million deaths (45%) of cardiovascular disease and 8.8 million deaths (22%) of cancer [1]. In China, lung, liver, gastric, oesophageal, colorectal, breast and pancreatic cancers are the leading causes of cancer deaths [2, 3]. However, since there is a great geographical span, an uneven economic development, and differences of natural environments influencing lifestyle and eating habits, the types of cancer diseases are rather different in different parts of China, even within local areas. For example, in a study on a cohort in 486,085 people of a routine health screening at the Health Centre, Fujun 180 Hospital, Quanzhou city, south-east part of China, the incident rate of cancer increased rapidly by about five times from 2009 to 2014. The most frequently cancers were lung and liver, and in female cervix cancer. Of the 56,286 persons included in this health screening, 89 persons were discovered with malignancies and of these patients 52 were followed-up during 10–40 months. The average mortality was 48.5%, while the mortalities of the liver and lung cancer patients were 94% [4].
World Health Organization (WHO) reported that during the next 20–25 years the number of new cancer patients world-wide will increase by about 70%, from today of 14 million to about 25 million, i.e. we lost the “war” against the cancer, if we just continue as now. This is not only a tragedy for individual persons, but also a dramatically increases in the expenditures for the health care system. If we can prevent this, we not only help people with the risk of developing cancer, but also reduce the burden in the medical health care system [5]. How do we follow the strategy of WHO “Prevention and early detection of cancers”? Cancer is a long-term chronic and abnormal proliferating disease. Multiple gene mutations associated with cell growth regulation in certain enzymes and proteins leads to uncontrolled proliferation and thus development of malignancies, which may be take 10–30 years. Using tumor proliferating markers are may be the key point. Non-invasive serological methods for early detection of tumor may be give information of pre-malignant process and thus increases the possibility to cure patients. However, there are few tumor markers for early tumor screening in routine health centre today. Example of such markers is CEA (carcinoembryonic antigen) and AFP (alpha-fetaprotein) in commonly used for tumor screening. Since CEA and AFP markers are not directly assessing the rate of tumor proliferation [6], the value of early detection of cancers is still doubt.
Thymidine kinase 1 (TK1) was used as a precision protein molecular target for assessment of cell proliferating rate since 1950s. The TK1 level in tumor cells [7, 8, 9, 10, 11, 12], in tissues [11, 12, 13, 14, 15, 16, 17] or in serum [4, 11, 12, 18, 19, 20, 21, 22, 23] corresponds to cell proliferating rate and is expected to be a favour marker for assessment of tumor proliferating rate. Based on analysis of high number serum samples, serum TK1 concentration (STK1p) combined with early risk symptoms of tumor process, such as pre-cancer or tumor-related diseases, could be used as a strategy of early detection of cancers and thus for risk warning of development of malignancies later in the life [4, 11, 12, 20, 21, 22, 23]. According to a report of Wang et al. [4], elevated STK1p was more sensitive than CEA and AFP for patients who had malignant tumors and was also a reliable prognostic biomarker for death, while CEA and AFP were not.
To further understand how to use STK1p, CEA or AFP markers for early risk screening of pre-malignancy or diseases related cancer in the routing health centre, we determined the concentration distribution of STP1p, AFP and CEA in relation to ages in 56,178 persons participated a health screening. These persons had no symptoms of malignancies. The study was done at a health centre in south-east of China (QuanZhou, Fujian Province), an area with higher frequency of liver, lung and cervix cancers, during 2011–2014. This type of study might provide guidance for pre-cancer risk assessment, and are expected to lead to an early tumor detection in routine health screening.
The mean and median values of STK1, AFP and CEA with progressive ages
The mean and median values of STK1, AFP and CEA with progressive ages
Participants
In 2016, we reported a retrospective study on 56,286 people participated in a health screening during 2009–2014. Eighty-nine persons were found to have malignancies of different types [4]. Here we further analysis data from this study by focus on those persons (
All persons were covered by medical insurance and represented mainly people living and working in this area. A routine health screening system was used, including ultrasound, X-ray, electrocardiography, hepatitis-B virus infection test, blood/urine routine testing, physical examination, etc. In addition, 56,178 were tested for STK1p, 49,441 for AFP, 48,771 for CEA and 13,897 for PSA. In the health control group, 428 were tested for STK1p, 250 persons for AFP, 236 for CEA and 30 for PSA.
The participants were divided into three age groups: 21–40, 41–60 and
Methods
The assessment of pre-malignancy and diseases link to the risk of developing malignancies has not been standardized. The concept of pre-cancers are the earliest morphologically discernible lesions that present the development of invasive cancer. In fact, the term pre-cancer is often confused with many unrelated terms. Currently, the term “intraepithelial neoplasia” is wide usage by pathologists. There are hundreds of different pre-cancers of human. A more extensive listing of pre-cancers could be found in the appendix published by Berman and Moore [24]. In this study, we attempted to tailor multiple available options for assessment of pre-malignancy and diseases link to the risk of development of malignancies described by Berman and Moore in 2010.
Discovery of tumor-related symptom
In order to screen for pre-cancer or diseases link to developing malignancy or suspected malignancy, an advanced Doppler Ultrasound Diagnostic Apparatus (Voluson E8, American General Corporation) was used. For example: Liver and gallbladder diseases (liver fibrosis, liver cirrhosis, or suspicion of liver cancer); uterine diseases (tumors, endometriosis, uterine abnormalities, ovarian mass, pelvic inflammatory mass or abscess, etc.); breast diseases (the size, shape and edge of the lesion, it is an important and convenient method for early diagnosis of breast hyperplasia); prostate diseases (shape, size and position, the diagnosis of prostatic hyperplasia, calculus, calcification disease and prostatic abscess, cyst or chronic prostatitis, suspicion of prostate, cancer. It is also suitable for benign prostatic hyperplasia patients); thyroid diseases (size and volume, to assist the identification of pure, nodular, thyroiditis, hyperthyroidism, thyroid tumor such as adenoma, cyst, thyroid, parathyroid hyperplasia, cyst and parathyroid carcinoma). Additionally, it was also used for preliminary screening of heart diseases, such as internal structure, heart beat and blood flow, and other types of heart disease or cardiomyopathy.
The X-ray was combined with CT/SCT for further detection who had suspicion lung cancer.
Serological assays
All serum samples were collected in the morning on fasting condition. Blood collected without anticoagulant was centrifuged at 800
2.2.2.1. Serum TK1 assay
The concentration of serum TK1 (STK1p) was measured by using a commercial kit based on an enhanced chemiluminescent (ECL) dot blot assay as described by the manufacturer (SSTK Ltd., Shenzhen, China). Samples comprising 3
2.2.2.2. AFP and CEA assay
The levels of AFP and CEA were performed on an electrochemiluminescence automatic immunoassay (Roche Diagnostics e601GmbH, Mannheim, Germany). The reference cut-off values were 10.0 ng/mL and 5.0 ng/mL, respectively. The electrochemiluminescence (ECL) automatic immunoassay analyser is based on paramagnetic particles as a solid phase, biotin-streptavidin-detection system and two-dimensional bar code technology. It is a highly sensitive light detection system that provides excellent low-end sensitivity and broad dynamic measuring ranges.
Concentration distribution of STK1p, AFP and CEA of health disease-free group and of people below cut-off values (low-risk group) in relation to progressive age.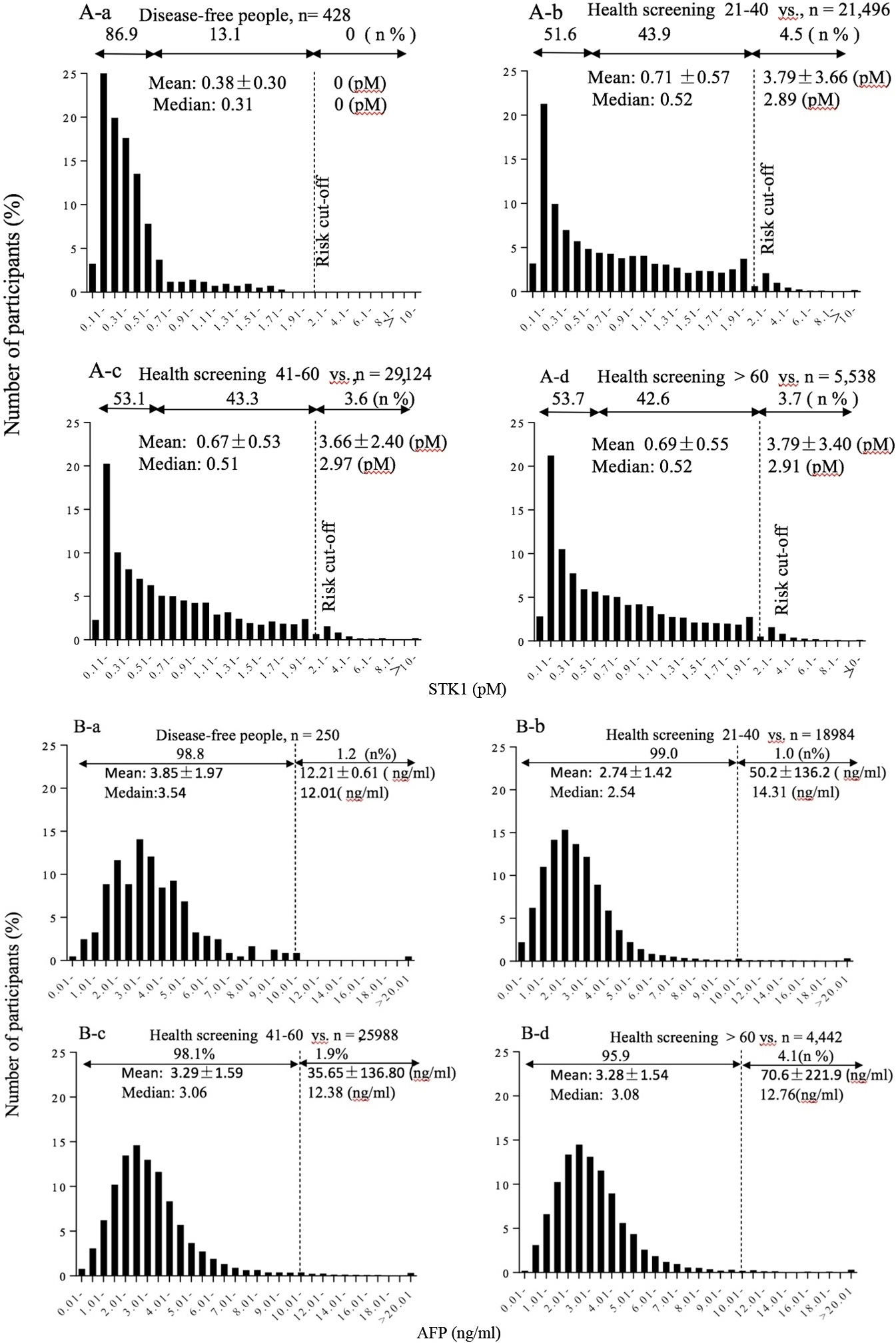
continued.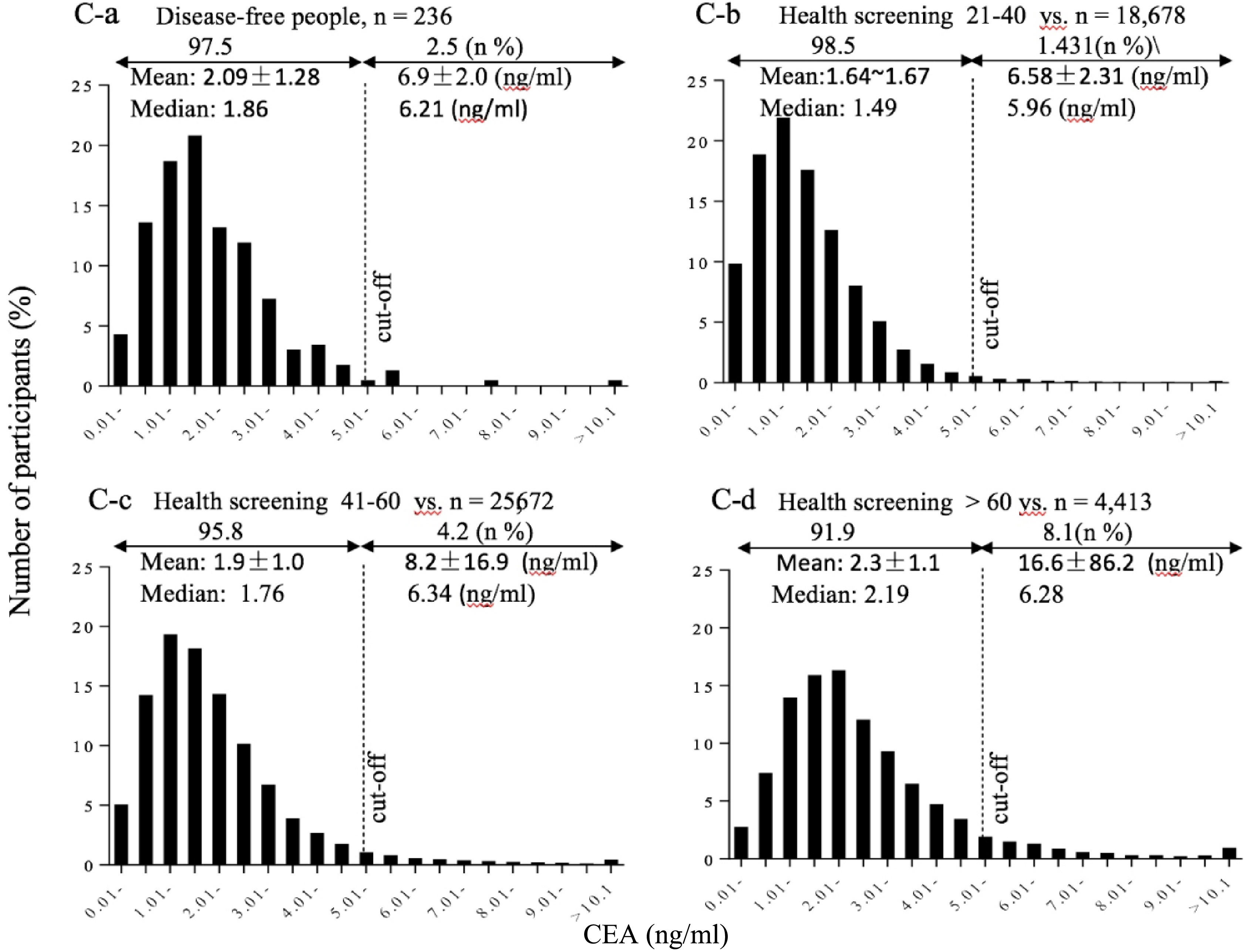
2.2.2.3. PSA assays
PSA was determined by an electrochemiluminescence immunoassay. The electrochemiluminescence automatic immunoassay analyzer is based on paramagnetic particles as a solid phase, biotin-streptavidin-detection system and two-dimensional bar code technology. It is a highly sensitive light detection system that provides excellent low-end sensitivity and broad dynamic measuring ranges. Assays of PSA used Beckman DX1800, Germany. The reference cut-off value was 4.0 ng/ml. The value was considered positive or negative for the marker when the level was above or below the cut-off value.
2.2.2.4. ALT, AST and GGT assays
Three enzymes in serum, alanine aminotransferase (ALT), aspartate aminotransferase (AST),
The mean values of STK1p, AFP and CEA levels were calculated by a mean
Results
The persons participated in the health screening were divided into three age groups: 21–40, 41–60 and
Correlations between STK1p and AFP, STK1p and CEA and between CEA and AFP in serum of people below cut-off values (low-risk group).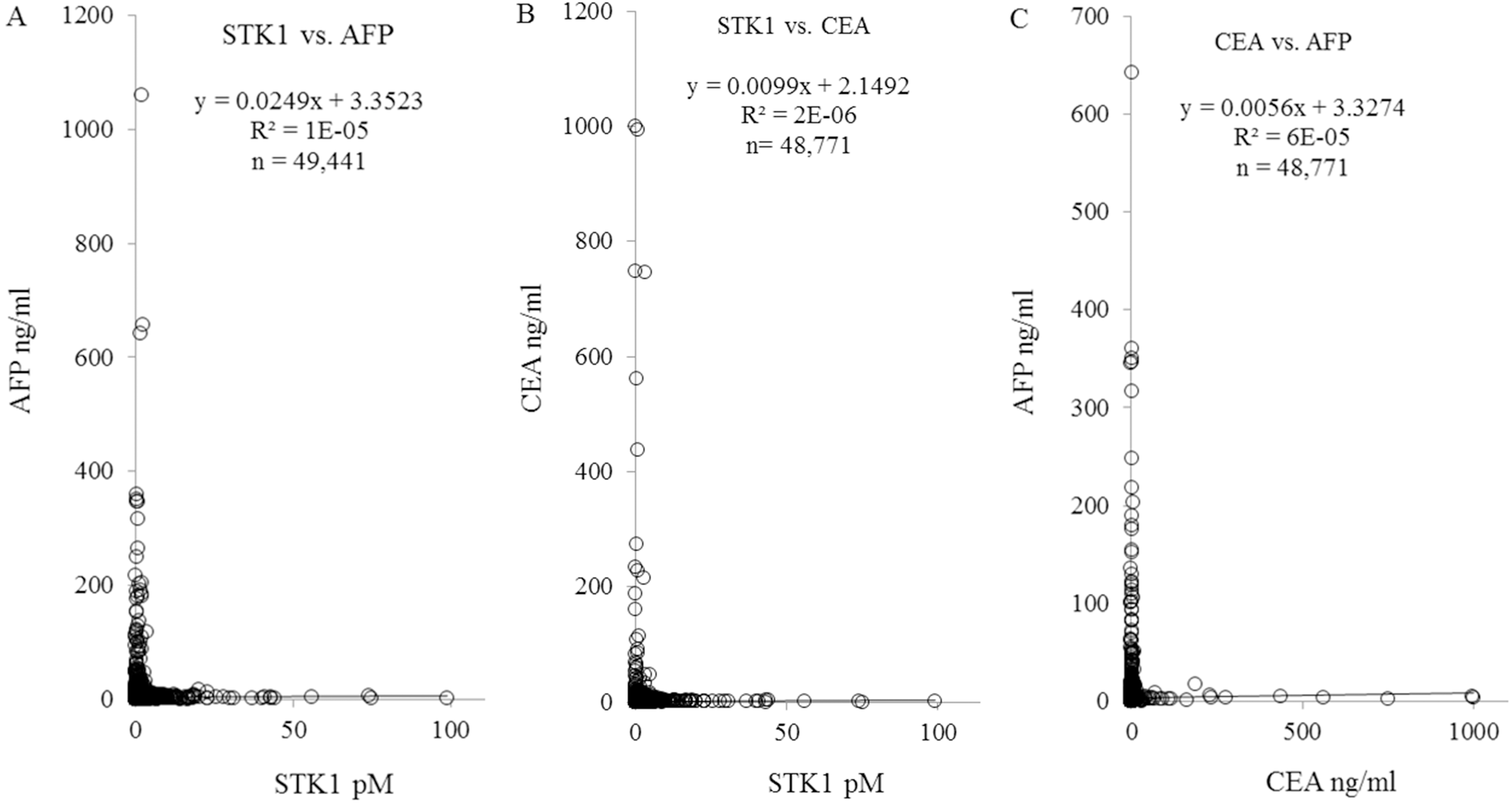
There was a significantly increase in the STK1p, AFP and CEA values by age in the health disease-free group, as well as in the low-risk AFP and CEA group (Table 1). No significant difference was found in the STK1p, AFP and CEA values in the elevated-risk group by age (Table 1).
Comparison of health disease-free and low-risk groups
We further analysis the results by compare the STK1p, AFP and CEA values of the low-risk group (below cut-off) with the health disease-free group to find out if those biomarkers could indicate risk for development of pre-cancer and in the end malignancy.
STK1p
There were significantly higher STK1p values in the low-risk group compared to the health disease-free group (Table 1A) in all age groups (21–40, 41–60,
AFP
In opposite to STK1p, AFP values in the low-risk group (
STK1p, AFP and CEA values in the low-risk group with different types of liver pre-malignancy diseases
STK1p, AFP and CEA values in the low-risk group with different types of liver pre-malignancy diseases
*Disease associated with risk of process of malignancy, **pre-malignancy.
As in the case of AFP, CEA values were also lower in the low-risk group (
Concentration distribution of STK1p, AFP and CEA in different age groups
In this part of the study we extended the analysis of the low-risk groups by determining the distribution of the concentrations of the biomarkers to see if it could give further prognostic information. The low-risk groups were divided into three age groups (21–40, 41–60,
STK1p
In the health disease-free group the STK1p concentration was almost normal distributed between 0.1–0.6 pM (86.9%) with a limited tail up to 2.0 pM (13.6%) (Fig. 1A-a). No persons with STK1p above the cut-off value were found. The mean STK1p value was 0.38
AFP
In the health disease-free group 98.8% of the AFP concentrations were within a normal distribution with a tail up to 10.0 ng/ml of 1.2% (Fig. 1B-a). No person above the cut-off value was found. The concentration distribution of the low-risk group was very similar to the health disease-free group, however, the mean values were lower (Fig. 1B-b, B-c, B-d). No significantly differences between the ages was found.
CEA
An almost normal distribution of the CEA concentration was found in the health disease-free group (97.5% below cut-off, and 2.5% above cut-off) (Fig. 1C-a). An almost normal distribution of the CEA concentration was also found in the low-risk group with increasing number of persons above the cut-off value by age, from 1.4% to 8.1% (Fig. 1C-b, C-c, C-d). The mean values were almost similar between the health disease-free group and the low-risk group.
Correlation between STK1p, AFP and CEA
In order to understand the relation between STK1p, AFP and CEA in serum of person in the low-risk group we determined the correlation between those biomarkers. Here we used the total number of persons, since there was no significantly difference between gender or ages.
There were no significantly correlations between STK1p and AFP, STK1p and CEA, or CEA and AFP (Fig. 2).
STK1p and PSA values in low-risk persons with different types of prostate diseases including
STK1p and PSA values in low-risk persons with different types of prostate diseases including
**Pre-malignancy, *diseases associated with the risk process of malignancy.
The mean value of STK1p of the low-risk group was significantly higher compared to health disease-free group. The concentration distribution of STK1p also differed between low-risk group and health disease-free group with a shift to higher STK1p values. This were not seen for AFP and CEA. In the contrary, the mean AFP and CEA values were lower in the low-risk group compared to the health disease-free group and there was no significant increase in the number of low-risk persons towards higher AFP and CEA values. Thus, did persons with higher STK1p values (0.6–2.0 pM) compared to health disease-free persons (0.3–0.4 pM), but still not above the cut-off value (
In Table 2 we show STK1p, AFP and CEA values of persons who had different liver diseases, including pre-malignancy and diseases associated with the risk process of malignancy. All of them show significantly higher STK1p values (0.6–1.0 pM) compared to the health disease-free group (0.3–0.4 pM), but not for AFP (health 3.9 ng/ml; low-risk 2.9–3.5 ng/ml) and CEA (health 2.0 ng/ml; low-risk 1.7–2.0 ng/ml).
We also investigated the STK1p and PSA values in the low-risk group (below cut-off) with different types of prostate diseases (Table 3). While the STK1p value was significantly higher in all prostate groups compared to the health disease-free group, the PSA values in persons with various prostate disease were even less compared to corresponding PSA values in the health disease-free group.
Discussion
In this study, we further analysed whether mean values and concentration distributions of STK1p, AFP, CEA and PSA among low-risk people (below cut-off values) were related to pre-malignant diseases associated with tumor process. We found that only STK1p correlated to people with pre-malignant diseases, but not AFP, CEA or PSA. This open up for the use of STK1p as a marker for early detection of risk to develop cancer in health screening.
Characterization of concentration distribution of STK1p has been done previously (review Skog et al. [12]) showing a shift from a normal distribution in the health disease-free group to a normal distribution with extensive tail of elevated STK1p values in the low-risk group (people below cut-off value of 2.0 pM). These results were based on three independent health screening studies, totally 38,121 persons [21, 22, 23] and summary by Skog et al. [12]. Here we extended these studies by investigated the correlation to gender and ages.
STK1p in the health disease-free group was almost normal distributed between 0.1–0.6 pM (86.9%) with a limited tail up to 2.0 pM (13.6%). The mean STK1p value was 0.38
Of particular interest in this study is the close correlation between the elevated STK1p values of the low-risk group (0.6–2.0 pM) and the presence of moderate/ severe type of pre-malignancies and diseases linked to development of tumor in liver and prostate. This type of correlation was, however, not found for AFP, CEA and PSA, supporting that STK1p is a more reliable biomarker for early detection of pre-malignancies and diseases linked to development of tumor compared to other tumor-related markers. Furthermore, since STK1p is a proliferation marker [8, 9, 10, 11, 12], it also indicates that these types of pre-malignancies found in the low-risk group are linked to abnormal cell proliferation. Although it is known from previous health screenings [20, 23], that persons with STK1p values above cut-off values (
A similar study on STK1p as presented here was performed by Cao et al. previously [25] using the same assay. The study included 14,960 Chinese participates (9,586 males and 5,374 females) from 20 to 79 years old, excluding people who had pre-cancer (moderate/severe type of hyperplasia of breast, prostate, gastrointestinal, cervix, liver cirrhosis, refractory anemia), or risk-diseases associated with tumor progression such as, liver disease, moderate/severe fatty liver, high risk for hepatitis B, abnormal liver function, obese, benign tumors (such as renal, thyroid), severe cardiac disease, using any medication that could affect STK1 levels such as exogenous hormone therapy, pregnant women, suffer from acute illness such as inflammation/virus infection within 4 weeks. The remaining persons consist of persons with minor proliferating /chronic/ non-tumor diseases that could not affect the STK1p levels. It was found that the STK1p levels decreased from 0.51 to 0.36 pM between 20–40 years, reaching a plateau value of 0.35 pM in late adulthood. The STK1p values were similar to the STK1p values we found among the health disease-free people above 41 years in our study (0.38 pM). Thus, the result from the health disease-free group and people with minor proliferating /chronic/ non-tumor diseases show similar STK1p values, significantly lower compare to people with pre-malignancies or risk diseases associated with tumor progression. Thus, the STK1p could distinguish between people of health disease-free/ minor proliferating /chronic/ non-tumor diseases and people with pre-malignancies or risk diseases associated with tumor progression.
Taking our results and the results of Cao et al. [25] together, it indicates that our STK1p assay is a reliable test below 2.0 pM for pre-malignancies or a variety of diseases associated with the risk of cancer progression later in life. It proved that the STK1p assay developed by us achieves high sensitivity and specificity and therefore should be useful in routine health screening. STK1p can be an alternative or complementary approach to discover the process of early malignant tumors.
According to previous reviews from Cigna [26] based on American Society of Clinical Oncology (ASCO), American Cancer Society (ACS), and National Cancer Institute (NCI), CEA and AFP were not recommended as a health screening tool due to low specificity. A likely explanation is that CEA and AFP, as many other bio-markers, are substances produced, not only by the tumor, but also by other type of cells in the body in response to pre- and malignancy. Tumor markers are found in normal cells and could show higher level compared to tumor cells. Furthermore, tumor markers may not be elevated in the presence of a tumor, especially in early stages of the disease, may not be specific to a particular type of tumor, and/or may be elevated by more than one type tumor. Despite these limitations, tumor-related markers are successfully combined with other diagnostic tools (e.g., laboratory tests, biopsy, radiological imaging) to confirm diagnosis/prognosis.
Opportunities for identifying high-risk individuals may be joined by application of receiver operation characteristic (ROC) statistical analysis. In a ROC test of STK1p between pre-operative malignant patients (
In summary, according to the present and previously published results [20, 23, 25] it is obvious that already at STK1p values below the recommended cut-off value of 2.0 pM, i.e. 0.6–2.0 pM, there is an increased risk to develop pre-malignancy and in the end malignancy. How to use the STK1p in routine health screening? We suggest that the STK1p concentration shall be combined with individuals who had pre-malignancy or diseases associated with the risk process of malignancy specifically. In addition, the individual STK1 value in health screening should be divided into two STK1p sub-groups: 1. Initial risk step of development of pre-malignancy or diseases associated with the risk process of malignancy of STK1p values of 0.6–2.0 pM, recommends health screening annual; 2. High risk step of development of malignancy or diseases associated with the risk process of malignancy of STK1p
Footnotes
Acknowledgments
We acknowledge the Health Management Centre of PLA 180 Hospital, Quanzhou, China. We also appreciate the Sino-Swed Tongkang Biotech. Ltd., Shenzhen, China, for providing technical support.