
Abstract
BACKGROUND:
Aberrant sialylation is a characteristic feature associated with cancer. The four types of mammalian sialidases identified to date have been shown to behave in different manners during carcinogenesis. While NEU1, NEU2 and NEU4 have been observed to oppose malignant phenotypes, the membrane-bound sialidase NEU3 was revealed to promote cancer progression.
OBJECTIVES:
With the aim of improving the knowledge about sialidases deregulation in various cancer types, we investigated the amount of NEU1, NEU3 and NEU4 transcripts in paired normal and tumor tissues from 170 patients with 11 cancer types.
METHODS:
mRNA was extracted from patients’ tissue specimens and retrotranscribed into cDNA, which was quantified by Real-Time PCR.
RESULTS:
We found NEU1 and NEU3 to be up regulated, while NEU4 was down regulated in most cancer types. In particular, colorectal cancer tissues showed the highest increase in NEU3 expression. Both NEU1 and NEU3 showed a strong up-regulation in ovarian cancer.
CONCLUSIONS:
Our data show that human sialidases are expressed at different levels in healthy tissues and are strongly deregulated in tumors. Moreover, sialidases expression in our European cohort showed significant differences from Asian populations. Some of these peculiar features open potential applications of sialidases in cancer diagnosis and therapy.
Introduction
Aberrant sialylation of glycoconjugates in cancer cells is thought to be a characteristic feature associated with malignant phenotype [1, 2, 3]. Indeed, altered glycosylation of functionally important membrane glycoproteins may affect tumor cell adhesion or motility, resulting in invasion and metastasis [4]. Studies carried out since the last decade of the 20
In humans, four sialidases with different subcellular localizations and biochemical features have been described: a lysosomal sialidase (NEU1), a cytosolic sialidase (NEU2), a plasma membrane-associated sialidase (NEU3) and a mitochondrial/endoplasmic reticulum (ER) sialidase (NEU4) [6, 7]. Interestingly, the four types of mammalian sialidases identified to date were found to behave in different manners during carcinogenesis. While NEU1, NEU2 and NEU4 have been observed to oppose malignant phenotypes, the membrane bound sialidase NEU3 was revealed to promote cancer progression [5, 8].
For NEU1, NEU2 and NEU4, only preclinical data are available in cancer. An inverse relationship between NEU1 expression level and metastatic potential was found in mouse and human adenocarcinoma colon cells with different metastatic potentials [9, 10, 11]. Similarly, stable transfection of NEU2 was shown to inhibit lung metastasis, invasion and cell motility [10]. The implication in tumor transformation of NEU4, the sialidase associated to ER and mitochondrial outer membranes [12, 13] has been studied in colon cancer, where siRNA targeting NEU4 has been shown to cause a significant inhibition of apoptosis and a promotion of cellular invasiveness and motility [14].
Conversely, more details are available for NEU3. Up-regulation of NEU3 was shown to promote colorectal carcinogenesis [15] and NEU3 overexpression was also observed in several tumor tissues, such as colorectal, ovarian and prostate cancers [16, 17, 18]. Moreover, NEU3 has been shown to be involved in the regulation of transmembrane signaling at the cell surface, possibly through enzymatic modulation of gangliosides [19, 20] and/or interaction with other signal molecules like caveolin-1, Rac-1, integrin b4, Grb-2, ERK1/2 and EGFR [8].
Considering all the evidence linking sialidases to malignancy, the study of the deregulation of these enzymes in cancer appears of the outmost relevance. Therefore, we decided to carry out a comprehensive analysis concerning the level of sialidases deregulation and the relative expression in 11 different cancer types. Our results are also informative about the possibility to exploit sialidases as potential markers for cancer diagnosis.
Methods
Tissue samples
All the tissue specimens were collected from surgically resected cancer patients at the Institute of Pathology of Locarno from 2008 to 2011.
Overall, 170 patients were included and analysed in the present study. Fresh tissues from both primary colorectal tumours and paired normal mucosa were immediately frozen in liquid nitrogen and subsequently stored at
RNA extraction
From frozen tissue samples, total RNA was isolated using RNeasy Mini Kit (Qiagen, Chatsworth, CA, USA), according to manufacturer’s instructions. Biological samples were first lysed and homogenized in the presence of a highly denaturing guanidine-thiocyanate containing buffer that inactivates RNase, ensuring the purification of intact RNA. DNase digestion step was performed to eliminate genomic DNA contamination. Ethanol was added to ensure appropriated binding conditions for RNA to the silica-based membrane and to wash away contaminants. High-quality purified RNA was eluted in 30
From formalin-fixed paraffin-embedded tissues, total RNA was isolated using RNeasy FFPE Kit (Qiagen), according to manufacturer’s instructions. Briefly, one-two 10-micrometer thick tissue sections were initially treated with a Deparaffinization Solution (Qiagen). Next, samples were incubated in an optimized lysis buffer, which contained proteinase K, for RNA releasing. A short incubation at higher temperature partially reversed formalin crosslinking of the released nucleic acids, improving RNA yield and quality. We subsequently performed a DNase digestion step to eliminate all genomic DNA contamination including very small fragments that are often present in FFPE samples after prolonged formalin fixation and/or long storage times. Ethanol was added to improve RNA binding to the silica membrane and RNA was eluted in 20
cDNA synthesis and Real-Time PCR analysis
RNA (1
Each sample was analysed for sialidase expression and normalized for total RNA content using
The relative expression level was calculated with the 2
Statistical methods
Statistical analysis was performed using the computing environment R [24] and the following extension packages: ggplot2 [25], survival [26], knitr [27].
Raw expression values were normalized against the level of expression of the housekeeping gene.
Within normal tissues, normalized expression values and ratios between genes of the same normal tissue were calculated. Ratios were partitioned using the following intervals, [0, 1/2], [1/2, 2], [2, infinity), so that a 100% change was required as threshold to declare a difference of expression.
The natural logarithm of expression ratio between tumour over normal tissues was partitioned into three intervals [0,1/3], [1/3,3], [3, infinity] and percentages within classes calculated.
Spearman’s rank correlation statistics of tumour/ normal tissues ratio between pair of genes were calculated (permutation statistical test) for each tumour tissue and all pairs.
Bootstrap BC
Results
Cohort characteristics
In our study, we selected 170 tumor samples constituted by 21 colorectal cancers (CRC), 17 gastric cancers, 15 gastrointestinal stromal tumors (GIST), 14 kidney cancers, 17 liver cancers, 16 malignant melanoma (MM), 20 non-small cell lung cancers (NSCLC), 16 ovarian cancers, 16 pancreatic cancers, 8 papillary thyroid cancers (PTC) and 10 prostate cancers. Patient characteristics are summarized in additional Table S1.
Normalized values of NEU1, NEU3, NEU4 mRNA levels in normal (A) and tumor (B) tissues after logarithmic transformation. Estimated median values (black points) are shown given gene (by row) and tissue (by column). Bootstrap 95% confidence intervals (number of bootstrap samples is 10000) of medians are indicated by vertical segments around the point estimate.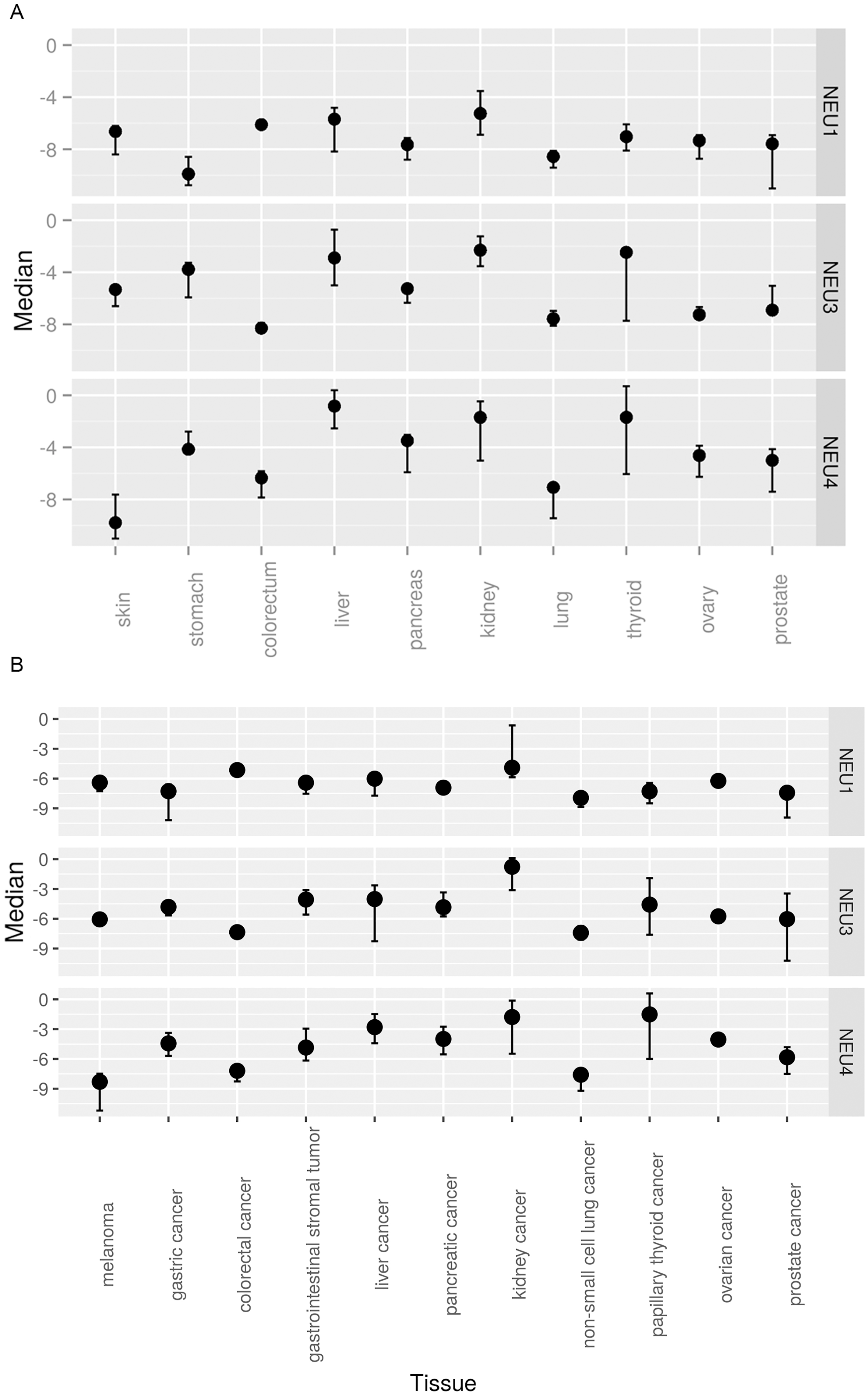
The majority of CRC patients were women (57%), aged between 48 and 88 years. CRC localization was predominantly in colon (90%), in particular in the right side (68%). TNM and grading classification of CRC cases highlighted a predominance of T3 (81%), N+ (57%) and G2 (57%) cancers.
Concerning gastric cancers, the analyzed cases were mainly female (53%) with an age range between 52 and 87 years. All samples were in the gastric region, predominantly in the body of the stomach (59%). The analyzed gastric cancers were mainly adenocarcinomas (AC) and tubular AC (70%) classified as N+ (71%), G2 (53%) and with an equal distribution between the tumor stages (T).
GIST patients were, in prevalence, women (53%), were aged between 43 and 81 years, showing tumors mainly located in the small bowel (67%).
Kidney cancers were equally distributed between male and female (50%) and between right and left kidneys, with an age range between 44 and 79 years. These cases were all clear cell renal cell carcinoma (CCRCC), mainly classified as T1 (64%).
As for liver cancers, the majority of cases were men (76%), aged between 50 and 86 years, usually involving both lobes (65%). Only two cases were associated with hepatitis B virus (HBV) or hepatitis C virus (HCV) (12%). All these cases were morphologically defined as hepatocellular carcinomas (HCC), classified predominantly as T3 (43%) and G2 (64%).
MM patients were mainly men (56%) with age distribution between 31 and 91 years. All the cases developed in skin tissues and 56% of them were classified as superficial spreading melanoma with predominance of T3 (44%) and N+ (60%) grading.
NSCLC cases were equally distributed between male and female and between right and left lung, with a patients’ age range between 46 and 75 years. All NSCLCs were classified as AC, with a prevalence of T1 (45%), N+ (60%) and, G2 (42%) classification.
Ovarian cancer patients displayed an age range between 39 and 86 years, were predominantly classified as serous AC (81%) with T3 (87%), N+ (60%), G3 (93%) grading, usually affecting both ovaries.
The majority of pancreatic cancers included in our cohort occurred in women (75%), with an age distribution between 48 and 85 years. They were all AC and they developed mostly in the head of the pancreas (63%); they were principally classified as T3 (82%), N+ (81%) and G2 (63%).
Among all the types of thyroid cancers, we selected PTC. Only one patient was a man and the age range was between 40 and 81 years. In the majority of PTC samples, the carcinoma developed in the right lobe (76%), with Tir5 (67%), T2 (50%) and N+ (60%) characteristics.
Finally, all patients affected by prostate cancer had an age range between 50 and 65 years and were affected by AC located in both lobes and predominantly classified as T2 (60%) and N0 (89%), with an age range between 50 and 65 years.
Spearman’s rank correlation (Rho)
Markers are listed by column and tumor tissues by row. The point estimated is indicated as
We initially evaluated the relative mRNA levels of NEU1, NEU3 and NEU4 from healthy tissues, namely skin, stomach, colorectum, liver, pancreas, kidney, lung, thyroid, ovary and prostate, by comparing their mRNA level to two housekeeping genes,
In accordance with data published in the literature, the cytosolic sialidase NEU2 could not be considered in our analysis because of its very low expression levels, often below detection [6].
Results are reported in Fig. 1A, as median values of mRNA levels. Human sialidase NEU1 showed similar expression levels in all tissues analyzed, with a slight decrease in the stomach and a slight increase in colorectum, liver and kidney. On the contrary, the levels of mRNA expression of NEU3 and NEU4 showed high differences among the tissues. In particular, high levels of NEU3 mRNA were observed in liver and kidney, as well as in the stomach and thyroid, while the lowest expression was found in colorectum. As for sialidase NEU4, the lowest mRNA levels were observed in skin, colorectum and lung, and the highest in liver, kidney and thyroid.
Ratios of normalized gene transcription values in normal tissues after partitioning. The distribution of ratios between expression values for each pair of genes (NEU3/NEU1, panel A, NEU4/NEU1 panel B, NEU3/NEU4 panel C) given tissue (by column) is partitioned into three classes: below 0.5 (labeled as below), between 0.5 and 2 (labeled as equal), above 2 (labeled as above). The resulting class frequency is represented as a percentage. Note that percentage values over the three classes add to 100% in all tissues for every pair of genes.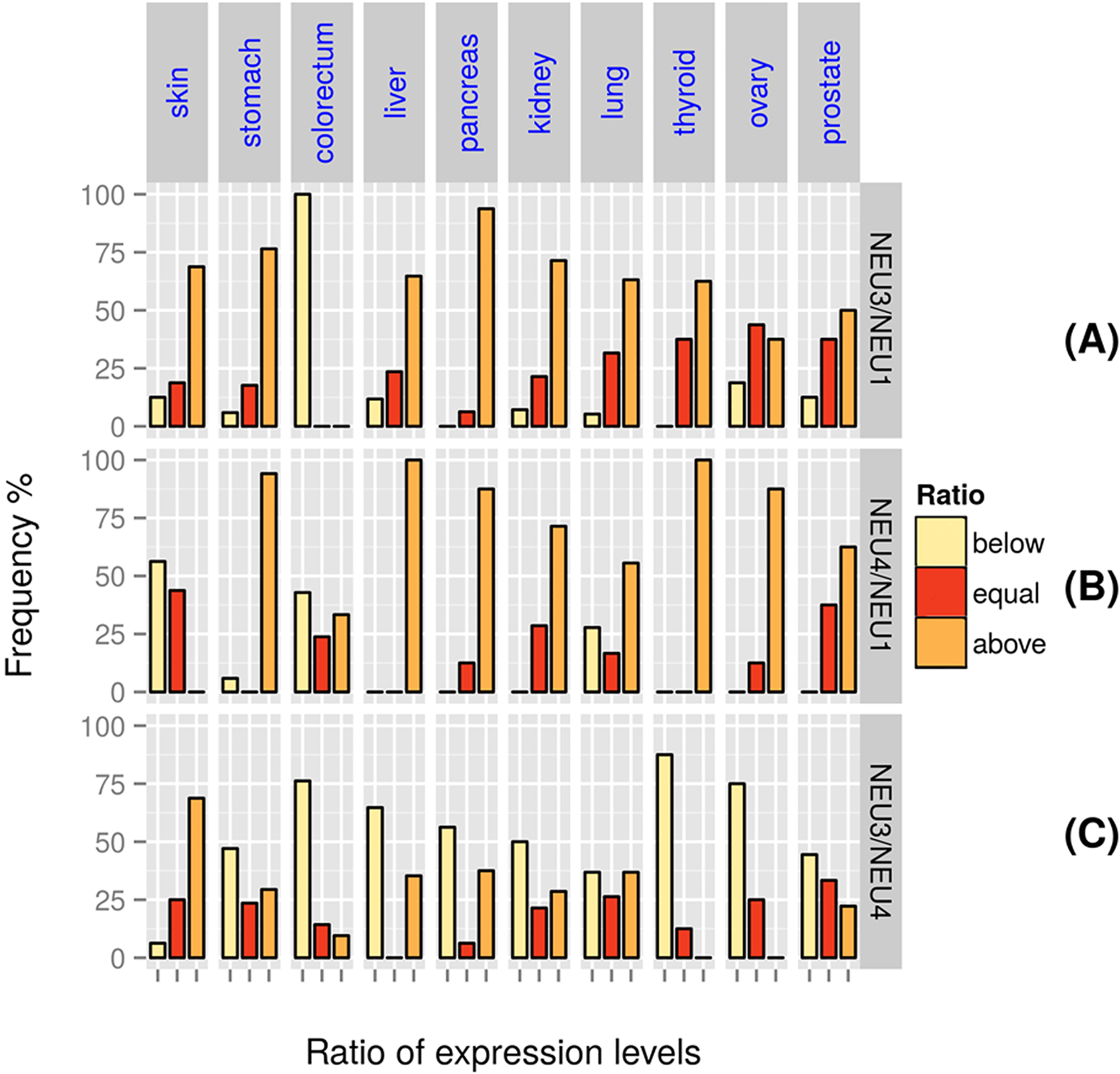
By comparing the expression of NEU1, NEU3 and NEU4 within each tissue, it can be observed that liver and kidney tissues showed the highest expression levels of all the three sialidases, whereas the lung is one of the tissues where the three sialidases are all expressed at lower levels. Intriguingly, very low NEU3 mRNA levels were found in colorectal healthy mucosa.
The above qualitative features based on median values over replicates do not change if mean values are preferred to medians (data not shown).
To compare the relative expression of sialidases among tissues, we calculated the relative expression levels of NEU1 vs NEU3, NEU1 vs NEU4 and NEU3 vs NEU4, with the mRNA fold ratios NEU3/NEU1, NEU4/NEU1 or NEU3/NEU4, each fold being previously normalized on the housekeeping
Our data showed that sialidase NEU3 was found less expressed than NEU1 in 100% of colorectal mucosa samples, but more expressed than NEU1 in all the other types of healthy tissues, except for the ovary and the prostate where the distribution of the three subgroups revealed equal and above fold ratios with similar values together with appreciable below fold ratio values (Fig. 2A). When NEU4 and NEU1 mRNA levels were compared, it was found that NEU4 was transcribed to a higher extent than NEU1 in the majority of the tissues, in particular in 100% of liver and thyroid tissue samples, while the levels were similar for colorectal and lung tissues. On the contrary, NEU4 turned out to be significantly less expressed than NEU1 in skin (Fig. 2B). Finally, the comparison between NEU3 and NEU4 mRNA levels showed that, in general, NEU3 is less expressed than NEU4, particularly in colorectal, thyroid and ovary tissues. On the contrary, the mRNA level of NEU3 is higher compared to NEU4 in skin, while the levels were similar for lung and prostate tissues (Fig. 2C).
We subsequently evaluated the relative quantification of mRNA levels of the different human sialidases in different types of cancer, in order to determine the variation of transcription rate in cancer. The fold increase/decrease in the different tumors was calculated through the 2
Distribution of gene expression ratios between tumor and normal tissues. The distribution of ratios between normalized expression values of the same gene (by row) in different tumor/normal tissues (by column) is partitioned into three classes: below 1/3 (labeled as Low), between 1/3 and 3 (labeled as Normal), above 3 (labeled as High). Note that percentage values add to 100% within each tissue-gene stacked bar.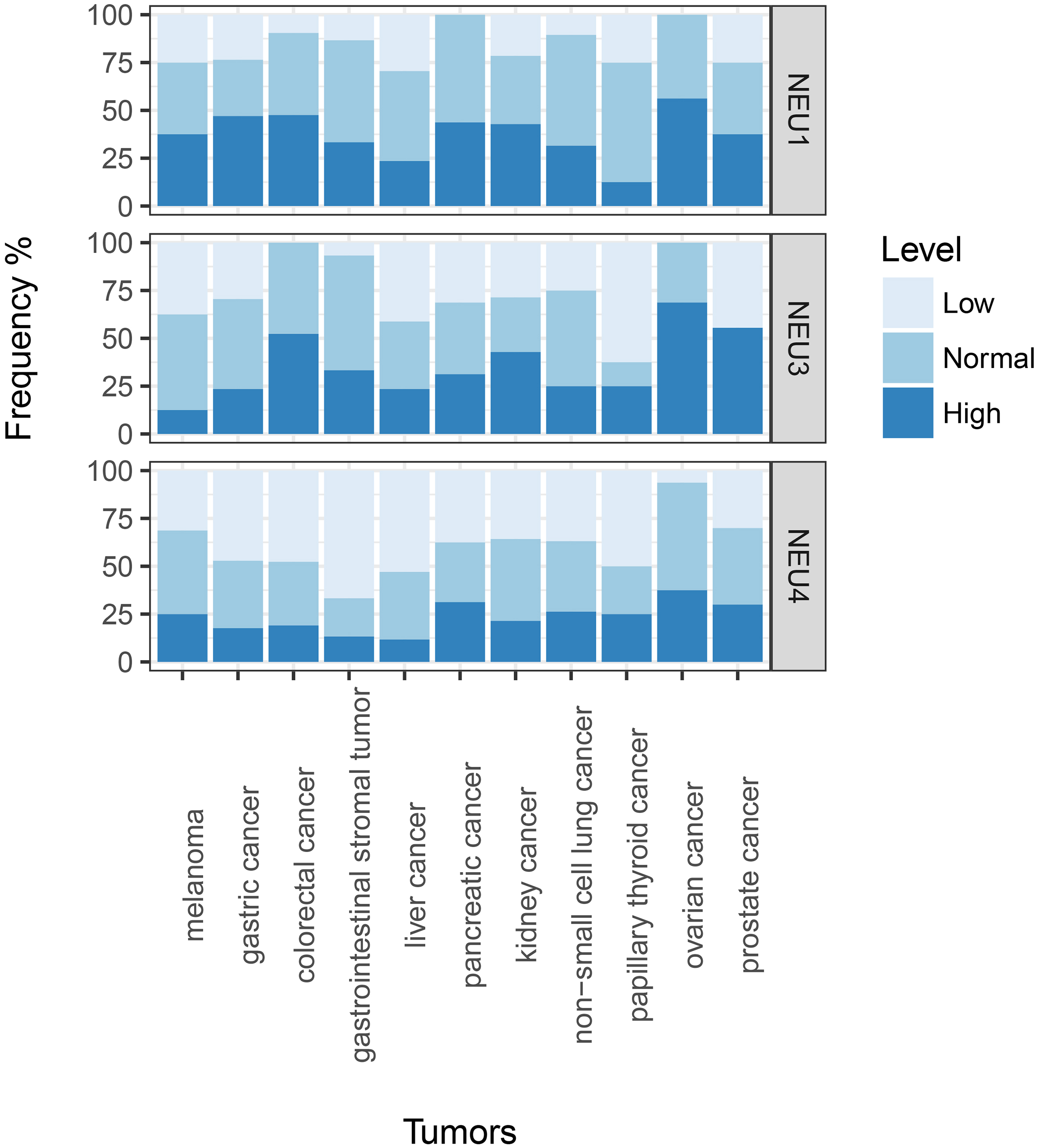
In Fig. 3 the relative mRNA expressions of human sialidases NEU1, NEU3 and NEU4 in different tumors, each normalized on its healthy tissue level, are shown as frequency rates. Relative frequency values are classified into 3 groups: low, normal and high, corresponding to values in the range (
Overall, sialidase NEU1 was found to be rarely down-regulated, the fraction of patients that show low frequency values never amounting to more than 30% in the tumor panel considered in this study. NEU1 overexpression was observed in roughly a half of cases in gastric, colorectal, pancreatic, kidney and ovarian cancer. Sialidase NEU3 showed the most varied behavior. Actually, NEU3 was found overexpressed in more than 50% of colorectal (52.38% high), ovarian (68.75% high) and prostate (55.56% high) cancers and normally or down regulated in all the other cancers, with the most relevant down-regulation detected in papillary thyroid cancer (62.50% low).
As for NEU4, a general down-regulation was observed in all the tumors analyzed, with the exception of ovarian cancer, where NEU4 is down regulated in only 6% of cases. Finally, NEU4 turned out to be up-regulated in a minor fraction of patients, with pancreatic, ovarian and prostate cancers.
The association between two tumor/normal tissues ratios for different genes within a tissue was assessed by calculating the Spearman Rank correlation coefficient, rho values being in the range
Using the two-tailed Fisher’s exact test and setting a value of statistical significance equal to
Discussion
Aberrant glycosylation is gaining increasing relevance in tumorigenic processes, in particular, altered sialylation is associated with malignant properties including invasiveness and metastasis [29, 30]. Sialylation is regulated by the interplay between anabolic sialyltransferases (STs) and catabolic sialidases (NEUs), working on a variety of glycans from oligosaccharides to glycolipids and glycoproteins [31]. Concerning sialidases, four genes, encoding for four different enzymes with distinct expression levels, subcellular localizations and biochemical features, have been discovered, but their role is far to be completely understood, not only in cancer cells, but also in normal conditions [6]. The aim of the present study was to evaluate as mRNA content the expression levels, of the three most expressed human sialidases (namely NEU1, NEU3 and NEU4) in the same cohort of paired normal and tumor tissues, all from a western country population (southern part of Switzerland, central Europe). We decided to use an objective method, real-time PCR, for the assessment of sialidases expression instead of other assays, such as immunohistochemistry, which are observer-dependent and can generate different results on the basis of different fixation times. Sialidase NEU2 was not taken into consideration because its expression levels were found below the detection limit, in agreement with the data previously reported in the scientific literature [6] as well as from those of the Human Protein Atlas [32].
There are different interesting points worth mentioning in the present study. First of all, it is the largest study on sialidases, because 170 cases from 11 cancer types were included, although there are other studies analyzing sialidases in different tumor types [33]. Furthermore, this work includes only Western population cohorts, while the majority of studies so far published have been performed on Asian patients. In this perspective, a comparison between Asian and Western countries can be made. Actually, sialidases can be deregulated in different ways in populations characterized by different life-styles and living in different countries. Moreover, comparisons of sialidases between healthy and tumor tissues in the same patient are not affected by technical bias.
On the contrary, the main weak point is represented by the small representation of each tumour type. However, the clinical-pathological features are adequately representative of larger cohorts.
Sialidase NEU1 was found to be expressed at similar levels in all the samples of our cohort, with the stomach showing the lowest levels, and kidney, liver and colon-rectum as the tissues with the highest expression. On the contrary, a considerable variability in NEU3 and NEU4 expression levels was observed among the analyzed samples, with both these membrane-associated sialidases more expressed in liver and less expressed in colorectum. In the literature, classical Northern-blot [34] or dot-blot on commercial membrane [35, 36] have been used to assess the transcript content in different tissues and, more recently, these data have been updated by RNA-Seq approach [37] and systematically collected in The Human Protein Atlas [32].
Concerning NEU1 expression in normal tissues, as expected from a lysosomal enzyme, the transcript appears to be ubiquitous: in our samples, the stomach is one of the tissues where NEU1 is less abundantly expressed and the kidney is one with the highest expression of NEU1, in agreement with the literature [32]. On the contrary, at odds with our data, previous analyses by Northern-blot revealed NEU1 transcript as most abundant in pancreas and relatively low in brain [34], whereas The Human Protein Atlas reports high levels also in thyroid and middle levels for colon-rectum and liver. For NEU3 transcript, we found high levels in liver, kidney, stomach and thyroid, whereas The Human Protein Atlas reports high levels for prostate and low levels for liver, stomach and kidney. Another study demonstrated a ubiquitous expression of NEU3 with transcript detectable at various level in 50 different human tissues, with the higher signals in testis, skeletal muscle, adrenal gland and thymus [35]. For NEU4, only the expression levels in a few tissues are included in The Human Protein Atlas, which are mirrored by our data, if we exclude the evaluation of kidney levels (high in our cohort and low in The Human Protein Atlas) [32]. Similarly to NEU3, the expression data derived by hybridization reveal a wide expression at low levels in most of the 50 different human tissues dotted on the membrane, with the highest expression in liver [36]. There are several hypotheses for the explanation of the discrepancies between our data and those previously reported in the literature or available in The Human Protein Atlas database. Among them we found: i) the different type of tissue preservation (fresh/frozen vs formalin-fixed paraffin-embedded); ii) the protocols used for mRNA extraction/isolation/quantitation and retro-transcription; iii) the use of different housekeeping genes as internal calibrator; iv) the use of different methods to assess the content of a particular transcript (i.e. RT-PCR versus RNASeq or Northern blotting); v) the use of different cohorts with different ethnicity, alimentary and environmental conditions. However, if we consider the expression data obtained so far altogether, we can draw a few clear conclusions about normal tissues: i) NEU1 transcript is quite constant among tissues; ii) the level of NEU3 transcripts is rather variable and generally low; iii) finally, NEU4 transcript tissue distribution is again variable and generally low and seems to be relevant in liver.
The strength of our study is the possibility to compare the expression levels of NEU1, NEU3 and NEU4 in the same patients’ normal tissues. Interestingly, our data indicate that NEU3 is generally more expressed than NEU1 in all the investigated tissues, with the relevant exception of colorectal mucosa. Actually, in that tissue, 100% of cases displayed NEU3 expression at levels lower than NEU1, probably indicating that only a small amount of the plasma membrane-associated enzyme is needed. The same transcriptional pattern was observed for NEU4, with few exceptions. More than 80% of normal tissues from liver, pancreas, thyroid and the ovary showed a significantly higher level of NEU4 transcript with respect to NEU1 transcript. On the contrary, when we compared NEU3 and NEU4 expression levels, in general the two genes were more equally expressed. Overall, our study of NEUs transcriptional pattern in normal tissues confirms NEU1 as the most important member of the family and supports its role as a possible opponent to the malignant transformation [5, 38]. In this condition, the expression patterns of NEU3 and NEU4 seem to be quite superimposable.
Therefore, these results enhance an in-depth analysis of the role played by the different sialidases and their interplay upon physiological conditions. Of course, our results deserve confirmation on larger cohorts, possibly from countries with different ethnicity, alimentary and environmental conditions.
Intriguing information comes from the analysis of paired cancer tissues. Our results clearly indicate that NEU1 is up regulated in most cases in all cancer types. This is in contrast with other previously published data, demonstrating that NEU1 overexpression may suppress cell migration and invasion in human colon adenocarcinoma HT-29 cell line, whereas its knock-down resulted in the opposite effects. Actually, when NEU1-overexpressing cells were injected transplenically into mice, the in vivo liver metastatic potential was significantly reduced [11]. Furthermore, in rat and murine cell lines an inverse relationship between this sialidase expression level and metastatic potential has been showed [9, 10]. On the other hand, our results agree with those reported for NEU1 in The Human Protein Atlas, showing either high or medium levels of NEU1 expression, as evaluated by immunofluorescence techniques using specific antibodies in almost all the 20 different cancer tissues investigated. Furthermore, due to the pivotal role played by NEU1 in lysosomal degradation of sialoconjugates, it seems reasonable to suppose that its levels are strictly linked to those of these important organelles and to the increased metabolic rate of cancer cell(s), requiring increased autophagy.
About NEU3, our data showed its overexpression in colorectal, ovarian and prostate cancer. These data are in accordance with the supposed role of NEU3, in particular the promotion of cancerogenesis and the protection against apoptosis [15] as well as with data already published on human cancer tissues [17, 18, 39]. Moreover, Kakugawa et al. showed that NEU3 mRNA levels were increased up to 100-fold in human colon cancer tissues compared to adjacent non-tumor mucosa and a significant elevation of the corresponding enzyme activity in the tumors was also observed [16]. NEU3 overexpression in cancer cells, particularly colorectal cancer cells, may be related to its role in activating EGFR and its downstream pathway, as shown by our group [40]. More recently, Miyagi and colleagues showed that in a Japanese cohort of CRC patients NEU3 expression was increased by 3 to 100-fold in all the cases [41]. Conversely, we found that only slightly more than 50% of our cohort of CRC patients (including only Caucasian) showed NEU3 transcript over-expression, although the transcription rate was never found down-regulated. Again, these discrepancies could be mainly explained by ethnical, dietary and/or environmental differences.
Concerning sialidase NEU4, our results show down-regulation in almost all tumor tissues analyzed, in accordance with those reported in the literature, that correlate NEU4 sialidase down-regulation to the inhibition of apoptosis and to the promotion of cellular invasiveness and motility, as well as to tumor progression [42]. In our cohort of CRC patients, NEU4 transcription rate was mostly down-regulated and in about 50% of patients a reduction higher than 3-fold of its mRNA level was detected. Similarly, in a Japanese cohort of 41 CRC patients, NEU4 mRNA expression level showed a marked decrease, with an average reduction of 2.8 fold compared to normal mucosa [14]. Intriguingly, we found that in ovarian cancer NEU4 transcription level was either normal or over-expressed, indicating that the fourth member of the sialidase family could play different roles depending on the tissues where it is deregulated. It is worth noting that in our cohort of patients, all the three sialidases showed a marked transcript increase in ovarian cancer, suggesting that this tumor could have a peculiar sialome and that NEU4 deregulation may be a useful marker of ovarian cancer development.
Data regarding NEU3 and NEU4 reported in The Human Protein Atlas are only partially superimposable with those derived from our tissue samples. Concerning NEU3, the RNA-Seq approach showed the higher transcript content in testis, prostate and skeletal muscle in agreement with the literature [35], and significant protein evidence in kidney, breast and skeletal muscle. Surprisingly, histological evidence in cancer tissues showed a moderate positivity in glioma and melanoma, without any evidence of the protein in CRC. Regarding NEU4, the transcript content assessed by RNA-Seq was found high in the liver and digestive tract in agreement with the literature [36], whereas the protein evidence was high in the digestive tract, kidney, central nervous system, adrenal gland and nasopharynx tract. Histological findings of the protein in cancer tissues are more relevant than in the case of NEU3 but very low when compared to NEU1 (antibody staining in 10%, 4% and 74% of the cancers in case of NEU4, NEU3 and NEU1, respectively) and encompass several carcinoids, breast, pancreatic, endometrial and ovarian cancer, glioma and melanoma. No variations are detectable in liver cancer compared to protein expression in the normal tissue, whereas the enzyme appears down regulated in CRC, head and neck cancer as well as in lung, skin, stomach and thyroid cancer. As already mentioned, these differences could be ascribed to the experimental methods used and underline the extreme variability of biological samples and of the biases that are introduced when a qualitative/quantitative inspection is carried out. For these reasons, multidisciplinary approaches should be used, whenever possible, to describe complex biological systems.
Conclusion
Overall, our results show that NEU1, NEU3 and NEU4 are differently expressed in human healthy tissues, probably reflecting the peculiar roles played by these enzymes. In addition, our results confirm that sialidases transcription rate is strongly deregulated in cancer, suggesting an involvement of these enzyme proteins in malignant transformation. Although the role of NEU3 in colorectal, prostate and ovarian cancer, likely as activator of EGFR pathway, seems to be established, it is still to be elucidated in other neoplastic diseases. On the other hand, our results about NEU1 overexpression in cancer tissues indicate, for this sialidase, a different role as proposed so far, which may be connected to the higher growth rate of cancer cells and to the involvement of lysosomes in autophagy. Regarding NEU4, its downregulation in most tumors may be connected to a still unknown role in mitochondrial signal transduction, possibly related to apoptosis. Particularly interesting is the fact that colorectal and ovarian cancer showed the highest increase in NEU1 and NEU3 transcripts during tumorigenesis.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-170548.
Footnotes
Acknowledgments
This work was mainly supported by Fondazione Ticinese per la Ricerca contro il Cancro (Tessin Foundation against Cancer) to MiFr, and by Ministero dell’Istruzione, dell’Università e della Ricerca (MIUR) ex 60% and FAR funds to EuMo and PF, respectively.
Conflict of interest
The authors declare that they have no competing interests.
Abbreviations
AC: adenocarcinoma
CCRCC: clear cell renal cell carcinoma
CRC: colorectal cancer
ER: endoplasmic reticulum
GIST: gastrointestinal stromal tumors
HBV: hepatitis B virus
HCC: hepatocellular carcinoma
HCV: hepatitis C virus
MM: malignant melanoma
NSCLC: non-small cell lung cancer
PTC: papillary thyroid cancer
TNM: tumor-nodal-metastasis staging